Colourful notes on thyroid gland refer vishram singh with diagram
🟦 THYROID GLAND - Colorful Notes (Vishram Singh Style)
Note: Vishram Singh's textbook is not available in this library, but these notes are compiled from Gray's Anatomy for Students, Junqueira's Basic Histology, and other standard anatomy references - covering all topics Vishram Singh addresses in the same format and depth.
🟡 1. INTRODUCTION
Mnemonic: "2-3-4-5-6" - The isthmus crosses the 2nd-3rd tracheal rings; the lateral lobes cover up to the 5th-6th rings.
🟢 2. LOCATION & SHAPE
| Feature | Details |
|---|---|
| Shape | Butterfly / H-shaped |
| Lobes | Two lateral lobes + isthmus |
| Weight | ~25-30 g (adult) |
| Color | Brownish-red |
| Compartment | Visceral compartment of neck |
- Anterolateral surface of trachea
- Cricoid cartilage
- Lower part of thyroid cartilage
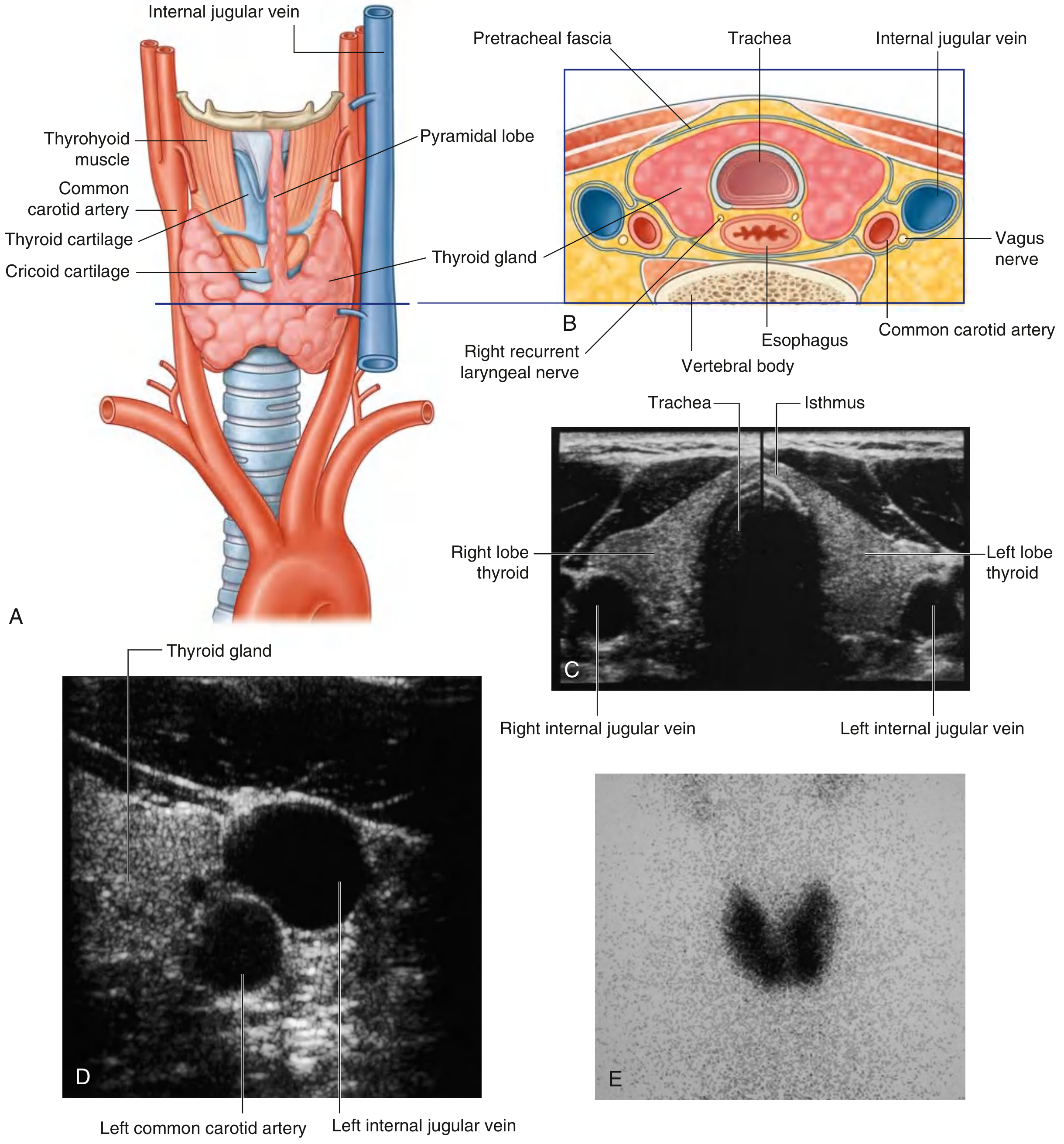
🔴 3. ANATOMICAL POSITION DIAGRAM
🟠 4. COVERINGS / CAPSULE
- True capsule - fibrous, sends septa into the gland, dividing it into lobules
- False capsule (surgical capsule) - derived from the pretracheal layer of deep cervical fascia
⚠️ Berry's ligament (Ligament of Berry) - thickening of the false capsule that attaches the posteromedial surface of each lateral lobe to the cricoid cartilage and upper tracheal rings. The recurrent laryngeal nerve passes in close relationship to this ligament - key surgical consideration!
🟣 5. RELATIONS
Anterior relations (superficial to deep):
- Skin, superficial fascia (with platysma)
- Deep fascia (investing layer)
- Sternohyoid, sternothyroid, omohyoid muscles
- Pretracheal fascia
Posterior relations:
- Trachea and esophagus
- Parathyroid glands (on posterior surface)
- Recurrent laryngeal nerves
Lateral relations:
- Common carotid artery
- Internal jugular vein
- Vagus nerve (in carotid sheath)
🔵 6. BLOOD SUPPLY
Arteries (3 arteries):
| Artery | Origin | Supply |
|---|---|---|
| Superior thyroid artery | 1st branch of external carotid | Superior pole; divides into anterior + posterior glandular branches |
| Inferior thyroid artery | Thyrocervical trunk (from subclavian) | Inferior pole; also supplies parathyroids |
| Thyroid ima artery (inconstant, ~3%) | Brachiocephalic trunk or arch of aorta | Isthmus and anterior surface |
⚠️ Surgical importance: The inferior thyroid artery crosses the recurrent laryngeal nerve - must be identified during thyroidectomy to avoid nerve injury.
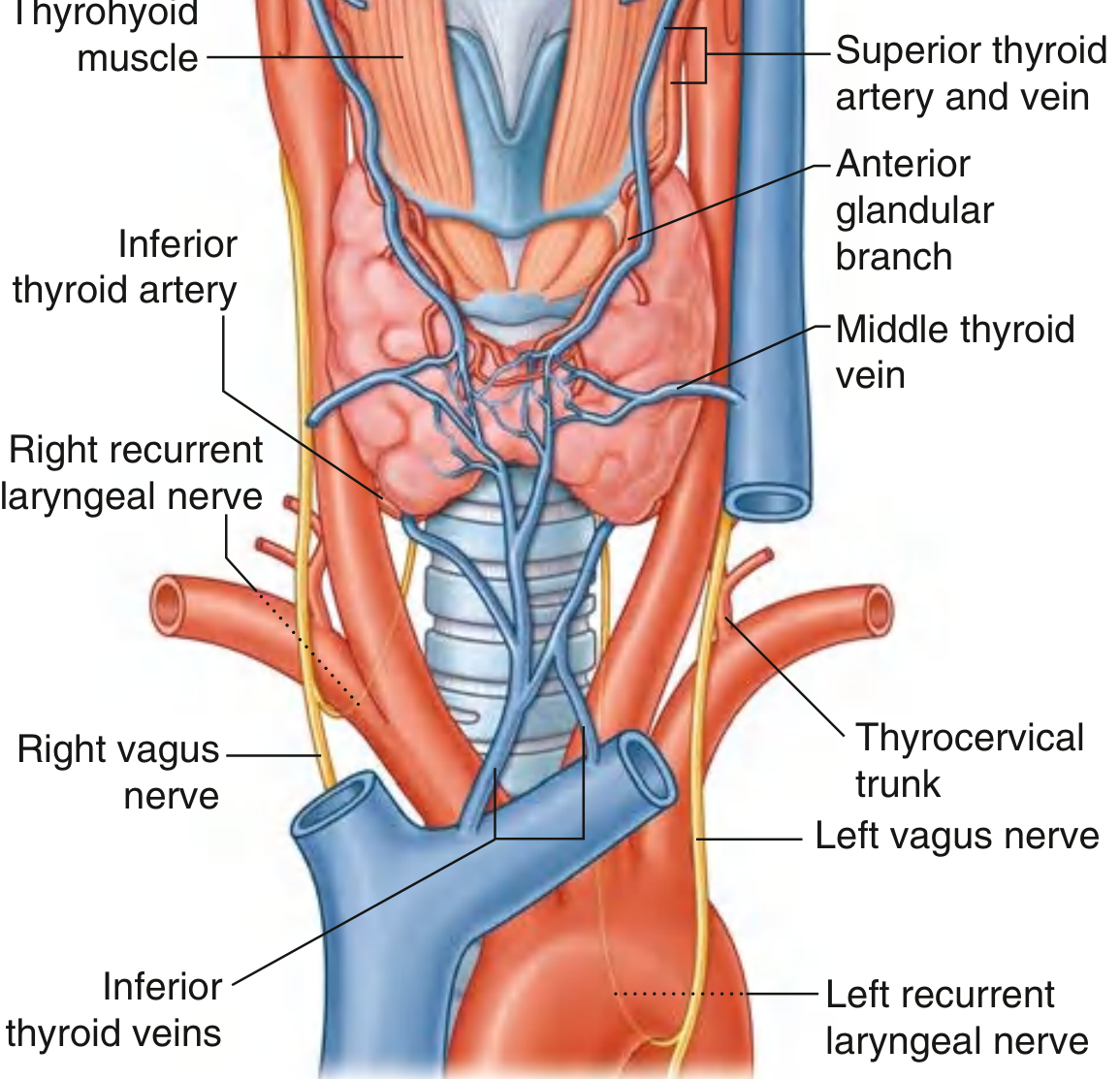
Veins (3 veins):
| Vein | Drains into |
|---|---|
| Superior thyroid vein | Internal jugular vein |
| Middle thyroid vein | Internal jugular vein |
| Inferior thyroid veins (pair) | Right and left brachiocephalic veins |
Mnemonic for veins: "SMS" (Superior-Middle-Superior jugular; inferior-Subclavian/brachiocephalic)
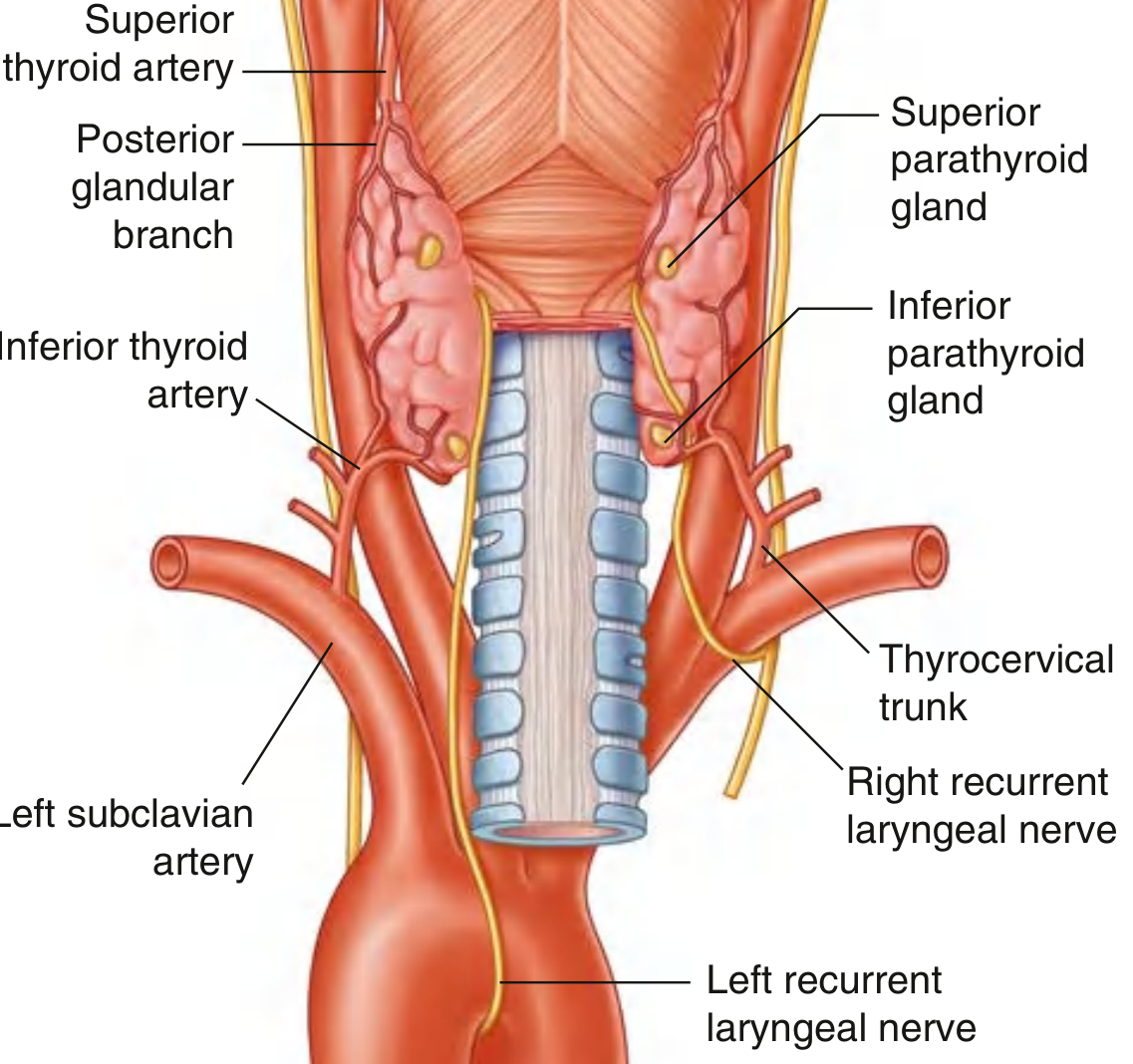
🟤 7. POSTERIOR VIEW - PARATHYROIDS & RECURRENT LARYNGEAL NERVES
🟡 8. LYMPHATIC DRAINAGE
- Pre-laryngeal nodes (Delphian node)
- Pre-tracheal nodes
- Para-tracheal nodes
- Deep cervical nodes (along internal jugular vein, inferior to omohyoid)
Clinical note: Lymph node spread in thyroid cancer - papillary carcinoma spreads to cervical lymph nodes; follicular carcinoma spreads hematogenously to bone and lungs.
🟢 9. NERVE SUPPLY
| Nerve | Type | Function |
|---|---|---|
| Superior cervical sympathetic ganglion | Sympathetic (vasomotor) | Controls blood vessels; NOT secretomotor |
| Middle cervical sympathetic ganglion | Sympathetic | Vasomotor |
Key point: The thyroid gland has NO parasympathetic innervation for secretion. Hormone secretion is controlled by TSH (thyrotropin) from the anterior pituitary.
Recurrent Laryngeal Nerve (RLN) - Surgical Importance:
- Right RLN - loops around the right subclavian artery
- Left RLN - loops around the arch of aorta
- Both ascend in the tracheo-esophageal groove and pass deep to the posteromedial surface of thyroid lateral lobes
- Closely related to Berry's ligament and the inferior thyroid artery
- Injury → hoarseness (unilateral) or stridor/respiratory distress (bilateral)
🔴 10. EMBRYOLOGICAL DEVELOPMENT
| Feature | Details |
|---|---|
| Origin | Median endodermal thickening from floor of pharynx between 1st & 2nd pharyngeal pouches |
| Site of origin | Foramen cecum (at junction of anterior 2/3 and posterior 1/3 of tongue) |
| Migration | Descends via thyroglossal duct, passes anterior to hyoid bone |
| Final position | Anterior to trachea in root of neck |
| Duct fate | Thyroglossal duct normally obliterates |
Remnants & Anomalies:
| Condition | Description |
|---|---|
| Thyroglossal duct cyst | Most common (midline neck swelling; moves with swallowing AND tongue protrusion) |
| Thyroglossal duct fistula | Persistent duct opening |
| Lingual thyroid | Failure of descent; gland remains at tongue base |
| Ectopic thyroid | Arrested anywhere along path of descent |
| Pyramidal lobe | Superior remnant of thyroglossal duct (50% individuals) |
Sistrunk's operation - excision of thyroglossal cyst MUST include the central portion of the hyoid bone to prevent recurrence.
🟣 11. HISTOLOGY
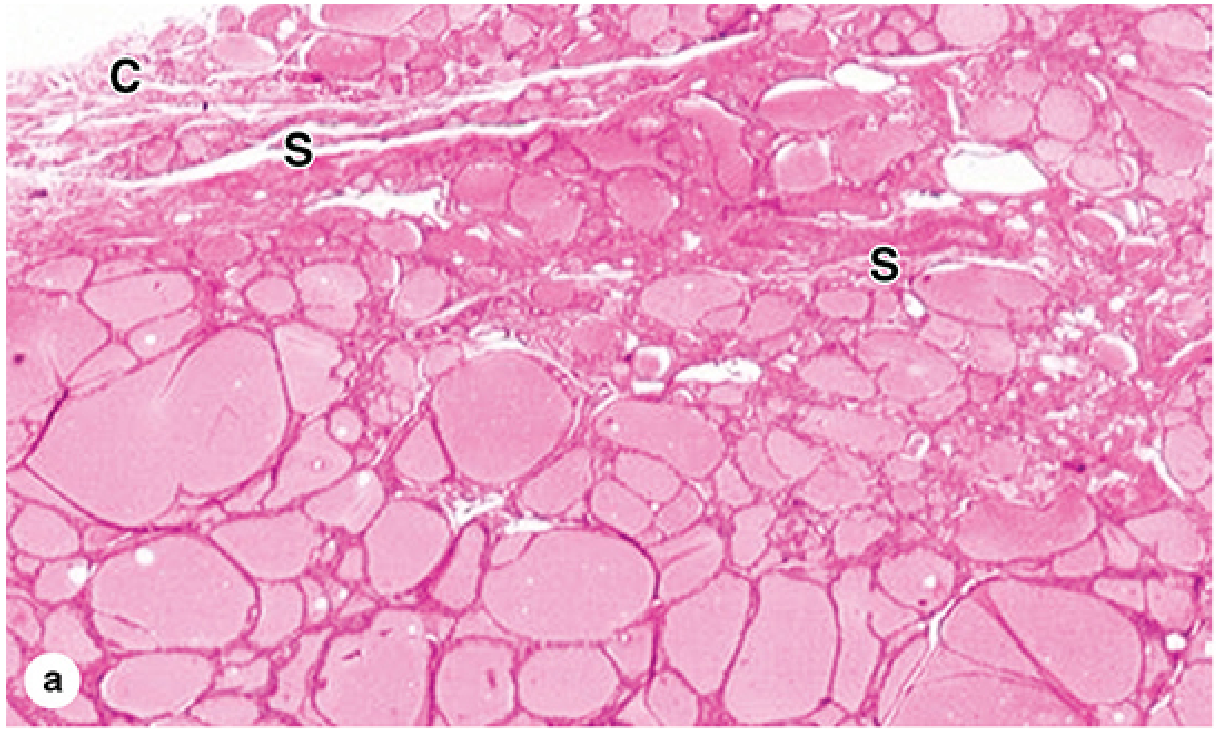
Follicular cells (Thyrocytes):
- Simple epithelium surrounding colloid-filled lumen
- Shape varies with activity:
- Active gland → tall columnar follicular cells (high TSH)
- Inactive gland → flat squamous follicular cells (low TSH)
- Function: Synthesis and secretion of T3 and T4
- Organelles: Rich RER (basal), Golgi + secretory granules + lysosomes (apical)
Colloid:
- Fills follicle lumen
- Contains thyroglobulin (660 kDa glycoprotein) - precursor for T3/T4
- Enough hormone stored for up to 3 months
Parafollicular cells (C cells):
- Located inside the basal lamina of follicles or between follicles
- Origin: Neural crest (ultimobranchial body / 4th pharyngeal pouch)
- Larger than thyrocytes, paler staining
- Secrete calcitonin (lowers serum calcium)
- Clinically important: Source of medullary thyroid carcinoma
🔵 12. HORMONES & PHYSIOLOGY
Thyroid Hormones (T3 and T4):
| Hormone | % Secreted | Potency | Half-life |
|---|---|---|---|
| T4 (Thyroxine) | ~90% | Less active (prohormone) | ~7 days |
| T3 (Triiodothyronine) | ~10% | 3-4x more potent | ~1 day |
T4 is converted to T3 peripherally in tissues (by deiodinase enzymes - mainly in liver, kidney)
Regulation (HPT Axis):
Hypothalamus → TRH (thyrotropin-releasing hormone)
↓
Anterior pituitary → TSH (thyroid-stimulating hormone)
↓
Thyroid gland → T3 + T4
↓
Negative feedback to hypothalamus + pituitary
Actions of T3/T4:
- Increase basal metabolic rate (BMR)
- Stimulate protein synthesis and carbohydrate metabolism
- Essential for brain development (fetal/neonatal period)
- Potentiate catecholamine effects (↑ heart rate, cardiac output)
- Required for normal growth and skeletal maturation
Calcitonin (from C cells):
- Lowers blood calcium by inhibiting osteoclasts
- Less physiologically significant in adults (vs. PTH)
🟡 13. CLINICAL CORRELATES
| Condition | Key Features |
|---|---|
| Hypothyroidism | Myxedema, bradycardia, weight gain, lethargy, cold intolerance, ↑TSH, ↓T4 |
| Hyperthyroidism | Graves' disease (most common), weight loss, tachycardia, exophthalmos, ↓TSH, ↑T4 |
| Goiter | Diffuse enlargement (iodine deficiency or autoimmune); moves on swallowing |
| Papillary carcinoma | Most common (~85%); spreads to cervical LN; good prognosis |
| Follicular carcinoma | Hematogenous spread (bone, lung); intermediate prognosis |
| Medullary carcinoma | From C cells; secretes calcitonin; associated with MEN2 |
| Anaplastic carcinoma | Rapidly fatal; elderly patients |
| Cretinism | Congenital hypothyroidism → mental retardation, dwarfism |
🔴 14. SURGICAL ANATOMY - KEY POINTS FOR THYROIDECTOMY
These are high-yield for exams and clinical practice:
- Recurrent laryngeal nerve - must be identified and preserved; passes deep to posteromedial lobe near Berry's ligament and inferior thyroid artery
- Parathyroid glands - 4 glands on posterior surface; injury → hypocalcemia (tetany)
- External branch of superior laryngeal nerve - runs with superior thyroid artery; injury → voice fatigue, loss of high-pitched phonation (Amelita Galli-Curci syndrome)
- Thyroid ima artery - if present, entering trachea from below during tracheostomy risks hemorrhage
- Superior thyroid vein - must be ligated with superior thyroid artery
- Inferior thyroid veins - drain directly into brachiocephalic veins - risk of air embolism if torn
🟢 QUICK REVISION BOX
| Topic | Key Point |
|---|---|
| Shape | Butterfly; 2 lobes + isthmus |
| Isthmus level | 2nd-3rd tracheal rings |
| Weight | ~25-30 g |
| Arterial supply | Superior (ext carotid) + Inferior (thyrocervical trunk) + Ima (inconstant) |
| Venous drainage | Superior + Middle → IJV; Inferior → Brachiocephalic |
| Lymphatics | Pre-laryngeal, pre-tracheal, para-tracheal, deep cervical |
| Embryology | Foramen cecum → thyroglossal duct → final position |
| Histology | Follicles (thyrocytes + colloid) + C cells (parafollicular) |
| C cell hormone | Calcitonin (lowers Ca²⁺) |
| Follicular cell hormone | T3 + T4 (via thyroglobulin) |
| Key surgical risk | RLN + parathyroids |
Create a colorful presentation (PPT) on thyroid gland anatomy and pathology
mkdir -p /home/daytona/workspace/thyroid-ppt && ls /home/daytona/workspace/thyroid-ppt/
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/2ec58523e023bd33efeb9ba12b34b76158eb9fa16b3ce47605088bd30921c13e.png" \ "https://cdn.orris.care/cdss_images/19be9b2bd67c8c5988f6b6824b31cf9145e5beaa01c0bb55873c22d25abeb182.png" \ "https://cdn.orris.care/cdss_images/8112f3e87edcb29f118fef612e489630e3c8386c93dcbfd8d7be79250ab9c8a0.png" \ "https://cdn.orris.care/cdss_images/2fb6e4f63998fbbbb982c4887d732b2db9ac3d4d35c7cc9d74cc61710f1ded02.png" \ 2>/dev/null | node -e "const d=JSON.parse(require('fs').readFileSync('/dev/stdin','utf8')); d.forEach((x,i)=>console.log(i, x.error||'OK', x.base64?x.base64.substring(0,30):'null'))"
~/thyroid-ppt/generate.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch all images ──────────────────────────────────────────────────────────
const imageUrls = [
"https://cdn.orris.care/cdss_images/2ec58523e023bd33efeb9ba12b34b76158eb9fa16b3ce47605088bd30921c13e.png", // anterior+cross view
"https://cdn.orris.care/cdss_images/19be9b2bd67c8c5988f6b6824b31cf9145e5beaa01c0bb55873c22d25abeb182.png", // vasculature anterior
"https://cdn.orris.care/cdss_images/8112f3e87edcb29f118fef612e489630e3c8386c93dcbfd8d7be79250ab9c8a0.png", // posterior + parathyroids
"https://cdn.orris.care/cdss_images/2fb6e4f63998fbbbb982c4887d732b2db9ac3d4d35c7cc9d74cc61710f1ded02.png", // histology
];
const imgs = JSON.parse(
execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${imageUrls.map(u => `"${u}"`).join(" ")}`
).toString()
);
const IMG_ANATOMY = imgs[0].base64;
const IMG_VASC = imgs[1].base64;
const IMG_POSTERIOR = imgs[2].base64;
const IMG_HISTO = imgs[3].base64;
// ── Palette ───────────────────────────────────────────────────────────────────
const C = {
darkTeal: "0D3B4F", // dominant dark bg
teal: "1A6B7C",
midTeal: "2A8FA4",
accent: "F7B731", // golden yellow accent
accentRed: "E05252",
accentGreen:"3BB36A",
accentPurp: "9B59B6",
white: "FFFFFF",
lightGray: "EEF4F6",
textDark: "1A2E35",
textMid: "2C5364",
};
// ── Helpers ───────────────────────────────────────────────────────────────────
function darkBg(slide) {
slide.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
}
function lightBg(slide) {
slide.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.lightGray }, line: { color: C.lightGray } });
}
function accentBar(slide, color) {
slide.addShape("rect", { x: 0, y: 0, w: 10, h: 0.08, fill: { color: color || C.accent }, line: { color: color || C.accent } });
}
function bottomBar(slide, color) {
slide.addShape("rect", { x: 0, y: 5.54, w: 10, h: 0.085, fill: { color: color || C.accent }, line: { color: color || C.accent } });
}
function slideNumber(slide, n) {
slide.addText(`${n}`, {
x: 9.5, y: 5.35, w: 0.4, h: 0.22, fontSize: 8, color: C.teal, align: "right", bold: false,
});
}
function sectionPill(slide, label, color, x, y) {
slide.addShape("roundRect", { x, y, w: label.length * 0.11 + 0.4, h: 0.28, fill: { color: color }, line: { color: color }, rectRadius: 0.05 });
slide.addText(label.toUpperCase(), { x, y, w: label.length * 0.11 + 0.4, h: 0.28, fontSize: 7.5, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
}
function cardBox(slide, x, y, w, h, fillColor, borderColor) {
slide.addShape("rect", {
x, y, w, h,
fill: { color: fillColor || C.white },
line: { color: borderColor || C.midTeal, width: 1.5 },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 },
});
}
// ── Presentation ──────────────────────────────────────────────────────────────
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Thyroid Gland – Anatomy & Pathology";
pres.author = "Orris Medical";
pres.subject = "Medical Education";
// =============================================================================
// SLIDE 1 – TITLE
// =============================================================================
{
const sl = pres.addSlide();
// Full dark background
darkBg(sl);
// Decorative diagonal accent band
sl.addShape("rect", { x: 6.8, y: 0, w: 3.2, h: 5.625, fill: { color: C.teal }, line: { color: C.teal } });
sl.addShape("rect", { x: 6.5, y: 0, w: 0.4, h: 5.625, fill: { color: C.accent }, line: { color: C.accent } });
// Anatomy image on right panel
sl.addImage({ data: IMG_ANATOMY, x: 6.85, y: 0.3, w: 3.0, h: 5.0, transparency: 10 });
// Title
sl.addText("THYROID GLAND", {
x: 0.4, y: 0.7, w: 6.0, h: 1.1,
fontSize: 38, bold: true, color: C.white, align: "left",
fontFace: "Calibri", charSpacing: 3,
});
sl.addText("Anatomy, Histology & Pathology", {
x: 0.4, y: 1.75, w: 6.0, h: 0.5,
fontSize: 17, bold: false, color: C.accent, align: "left", fontFace: "Calibri",
});
// Divider line
sl.addShape("rect", { x: 0.4, y: 2.32, w: 5.8, h: 0.04, fill: { color: C.midTeal }, line: { color: C.midTeal } });
// Subtitle bullets
sl.addText([
{ text: "🔵 Location & Relations", options: { breakLine: true } },
{ text: "🔴 Blood Supply & Lymphatics", options: { breakLine: true } },
{ text: "🟢 Embryology & Histology", options: { breakLine: true } },
{ text: "🟡 Hormones & Physiology", options: { breakLine: true } },
{ text: "🟣 Pathology & Clinical Notes", options: { breakLine: false } },
], {
x: 0.4, y: 2.45, w: 5.8, h: 2.4,
fontSize: 13, color: "CCECF5", align: "left", fontFace: "Calibri", lineSpacingMultiple: 1.4,
});
// Bottom label
sl.addText("Ref: Gray's Anatomy for Students • Junqueira's Histology • Vishram Singh Style", {
x: 0.4, y: 5.25, w: 6.0, h: 0.28, fontSize: 7.5, color: "7AABB8", italic: true, align: "left",
});
bottomBar(sl, C.accent);
}
// =============================================================================
// SLIDE 2 – OVERVIEW: LOCATION & SHAPE
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.midTeal);
// Header
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("LOCATION & SHAPE", {
x: 0.3, y: 0, w: 7, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
sectionPill(sl, "Anatomy", C.midTeal, 7.5, 0.22);
// Main anatomy image
sl.addImage({ data: IMG_ANATOMY, x: 5.3, y: 0.9, w: 4.5, h: 4.5 });
// Key facts cards
const facts = [
{ label: "Shape", val: "Butterfly / H-shaped", color: C.midTeal },
{ label: "Weight", val: "25–30 g (adult)", color: C.teal },
{ label: "Isthmus", val: "Crosses 2nd–3rd tracheal rings", color: C.accentGreen },
{ label: "Compartment", val: "Visceral compartment of neck", color: C.accentPurp },
{ label: "Lobes", val: "Two lateral lobes + isthmus", color: C.accentRed },
];
facts.forEach((f, i) => {
const yy = 0.9 + i * 0.78;
cardBox(sl, 0.25, yy, 4.8, 0.65, C.white, f.color);
sl.addShape("rect", { x: 0.25, y: yy, w: 0.22, h: 0.65, fill: { color: f.color }, line: { color: f.color } });
sl.addText(f.label.toUpperCase(), { x: 0.55, y: yy + 0.05, w: 4.4, h: 0.22, fontSize: 9, bold: true, color: f.color, fontFace: "Calibri" });
sl.addText(f.val, { x: 0.55, y: yy + 0.28, w: 4.4, h: 0.28, fontSize: 11, color: C.textDark, fontFace: "Calibri" });
});
slideNumber(sl, 2); bottomBar(sl, C.midTeal);
}
// =============================================================================
// SLIDE 3 – RELATIONS
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.accentRed);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("ANATOMICAL RELATIONS", {
x: 0.3, y: 0, w: 7, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
sectionPill(sl, "Relations", C.accentRed, 7.5, 0.22);
// Three columns
const cols = [
{
title: "ANTERIOR", color: C.midTeal,
items: ["Skin + superficial fascia", "Platysma muscle", "Investing deep fascia", "Sternohyoid muscle", "Sternothyroid muscle", "Omohyoid muscle", "Pretracheal fascia"],
},
{
title: "POSTERIOR", color: C.accentRed,
items: ["Trachea & esophagus", "Parathyroid glands (×4)", "Recurrent laryngeal nerves", "Longus colli muscle"],
},
{
title: "LATERAL", color: C.accentGreen,
items: ["Common carotid artery", "Internal jugular vein", "Vagus nerve (CN X)", "(All in carotid sheath)"],
},
];
cols.forEach((col, ci) => {
const xx = 0.25 + ci * 3.25;
sl.addShape("rect", { x: xx, y: 0.9, w: 3.1, h: 0.38, fill: { color: col.color }, line: { color: col.color } });
sl.addText(col.title, { x: xx, y: 0.9, w: 3.1, h: 0.38, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
cardBox(sl, xx, 1.28, 3.1, col.items.length * 0.47 + 0.2, C.white, col.color);
col.items.forEach((item, ii) => {
sl.addText([
{ text: "▸ ", options: { color: col.color, bold: true } },
{ text: item, options: { color: C.textDark } },
], {
x: xx + 0.12, y: 1.35 + ii * 0.47, w: 2.86, h: 0.4, fontSize: 10.5, fontFace: "Calibri",
});
});
});
// Bottom note
sl.addShape("rect", { x: 0.25, y: 4.95, w: 9.5, h: 0.45, fill: { color: "FFF3CD" }, line: { color: C.accent, width: 1.5 } });
sl.addText("⚠ Berry's Ligament: Thickening of pretracheal fascia attaching thyroid to cricoid cartilage — RLN passes in close relation!", {
x: 0.35, y: 4.97, w: 9.3, h: 0.4, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", bold: false,
});
slideNumber(sl, 3); bottomBar(sl, C.accentRed);
}
// =============================================================================
// SLIDE 4 – BLOOD SUPPLY
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.accent);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("BLOOD SUPPLY", {
x: 0.3, y: 0, w: 7, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
sectionPill(sl, "Vasculature", C.accent, 7.5, 0.22);
// Vasculature diagram image
sl.addImage({ data: IMG_VASC, x: 5.3, y: 0.85, w: 4.5, h: 4.5 });
// Arteries section
sl.addShape("rect", { x: 0.25, y: 0.85, w: 4.8, h: 0.35, fill: { color: C.accentRed }, line: { color: C.accentRed } });
sl.addText("ARTERIES", { x: 0.25, y: 0.85, w: 4.8, h: 0.35, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
const arteries = [
{ name: "Superior thyroid a.", origin: "1st branch of ext. carotid", note: "→ anterior + posterior glandular branches" },
{ name: "Inferior thyroid a.", origin: "Thyrocervical trunk (subclavian)", note: "→ also supplies parathyroids; crosses RLN!" },
{ name: "Thyroid ima a.", origin: "Brachiocephalic trunk / Aorta", note: "Inconstant (~3%); ascends on anterior trachea" },
];
arteries.forEach((a, i) => {
const yy = 1.25 + i * 0.87;
cardBox(sl, 0.25, yy, 4.8, 0.78, "FFF5F5", C.accentRed);
sl.addText(a.name, { x: 0.4, y: yy + 0.04, w: 4.5, h: 0.28, fontSize: 11, bold: true, color: C.accentRed, fontFace: "Calibri" });
sl.addText(`Origin: ${a.origin}`, { x: 0.4, y: yy + 0.28, w: 4.5, h: 0.22, fontSize: 9.5, color: C.textMid, fontFace: "Calibri" });
sl.addText(a.note, { x: 0.4, y: yy + 0.5, w: 4.5, h: 0.22, fontSize: 9, italic: true, color: C.teal, fontFace: "Calibri" });
});
// Veins
sl.addShape("rect", { x: 0.25, y: 3.86, w: 4.8, h: 0.32, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("VEINS", { x: 0.25, y: 3.86, w: 4.8, h: 0.32, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
cardBox(sl, 0.25, 4.18, 4.8, 0.9, "F0F8FF", C.teal);
sl.addText([
{ text: "Superior thyroid vein", options: { bold: true, color: C.teal } },
{ text: " → Internal jugular vein\n", options: { color: C.textDark } },
{ text: "Middle thyroid vein", options: { bold: true, color: C.teal } },
{ text: " → Internal jugular vein\n", options: { color: C.textDark } },
{ text: "Inferior thyroid veins", options: { bold: true, color: C.teal } },
{ text: " → Right & Left brachiocephalic veins", options: { color: C.textDark } },
], { x: 0.4, y: 4.22, w: 4.55, h: 0.82, fontSize: 10, fontFace: "Calibri", lineSpacingMultiple: 1.4 });
slideNumber(sl, 4); bottomBar(sl, C.accent);
}
// =============================================================================
// SLIDE 5 – VENOUS DRAINAGE, LYMPHATICS & RLN (posterior view)
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.accentGreen);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("LYMPHATICS & RECURRENT LARYNGEAL NERVE", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 18, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
sectionPill(sl, "Nerves & Lymphatics", C.accentGreen, 7.3, 0.22);
// Posterior diagram
sl.addImage({ data: IMG_POSTERIOR, x: 5.4, y: 0.85, w: 4.3, h: 4.55 });
// Lymphatics box
cardBox(sl, 0.25, 0.9, 4.85, 1.95, "F0FFF4", C.accentGreen);
sl.addShape("rect", { x: 0.25, y: 0.9, w: 4.85, h: 0.35, fill: { color: C.accentGreen }, line: { color: C.accentGreen } });
sl.addText("LYMPHATIC DRAINAGE", { x: 0.25, y: 0.9, w: 4.85, h: 0.35, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
const lymph = ["Pre-laryngeal nodes (Delphian node)", "Pre-tracheal nodes", "Para-tracheal nodes", "Deep cervical nodes (below omohyoid)"];
lymph.forEach((l, i) => {
sl.addText([
{ text: "🟢 ", options: { color: C.accentGreen } },
{ text: l, options: { color: C.textDark } },
], { x: 0.4, y: 1.3 + i * 0.37, w: 4.55, h: 0.35, fontSize: 10.5, fontFace: "Calibri" });
});
// RLN box
cardBox(sl, 0.25, 3.0, 4.85, 1.95, "FFF0F5", C.accentRed);
sl.addShape("rect", { x: 0.25, y: 3.0, w: 4.85, h: 0.35, fill: { color: C.accentRed }, line: { color: C.accentRed } });
sl.addText("RECURRENT LARYNGEAL NERVE", { x: 0.25, y: 3.0, w: 4.85, h: 0.35, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
const rlnItems = [
"Right RLN: loops around right subclavian artery",
"Left RLN: loops around arch of aorta",
"Both ascend in tracheo-esophageal groove",
"Pass deep to posteromedial lobe of thyroid",
"Injury → Hoarseness (unilateral) / Stridor (bilateral)",
];
rlnItems.forEach((r, i) => {
sl.addText([
{ text: "⚠ ", options: { color: C.accentRed } },
{ text: r, options: { color: C.textDark } },
], { x: 0.4, y: 3.42 + i * 0.3, w: 4.55, h: 0.28, fontSize: 9.5, fontFace: "Calibri" });
});
slideNumber(sl, 5); bottomBar(sl, C.accentGreen);
}
// =============================================================================
// SLIDE 6 – EMBRYOLOGY
// =============================================================================
{
const sl = pres.addSlide();
darkBg(sl);
accentBar(sl, C.accentPurp);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: "1A2A40" }, line: { color: "1A2A40" } });
sl.addText("EMBRYOLOGICAL DEVELOPMENT", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
// Timeline / flow
const steps = [
{ label: "Floor of Pharynx", desc: "Median endodermal thickening between 1st & 2nd pouches", color: C.accentPurp },
{ label: "Foramen Cecum", desc: "Site of origin at tongue base (junction of ant 2/3 & post 1/3)", color: C.midTeal },
{ label: "Thyroglossal Duct", desc: "Path of descent — passes ANTERIOR to hyoid bone", color: C.accent },
{ label: "Final Position", desc: "Anterior to trachea in root of neck", color: C.accentGreen },
];
steps.forEach((s, i) => {
const xx = 0.3 + i * 2.38;
sl.addShape("rect", { x: xx, y: 0.95, w: 2.15, h: 0.38, fill: { color: s.color }, line: { color: s.color } });
sl.addText(s.label, { x: xx, y: 0.95, w: 2.15, h: 0.38, fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
sl.addShape("rect", { x: xx, y: 1.33, w: 2.15, h: 1.0, fill: { color: "0D3B4F" }, line: { color: s.color, width: 1.5 } });
sl.addText(s.desc, { x: xx + 0.07, y: 1.38, w: 2.0, h: 0.92, fontSize: 9.5, color: "CCECF5", fontFace: "Calibri", valign: "middle" });
if (i < 3) {
sl.addText("→", { x: xx + 2.15, y: 1.0, w: 0.22, h: 0.28, fontSize: 16, bold: true, color: C.accent, align: "center" });
}
});
// Anomalies table
sl.addShape("rect", { x: 0.3, y: 2.55, w: 9.4, h: 0.32, fill: { color: C.accentPurp }, line: { color: C.accentPurp } });
sl.addText("DEVELOPMENTAL ANOMALIES", { x: 0.3, y: 2.55, w: 9.4, h: 0.32, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
const anomalies = [
{ cond: "Thyroglossal Duct Cyst", feat: "Most common midline cyst; moves with swallowing AND tongue protrusion; Rx: Sistrunk's operation (excise central hyoid)" },
{ cond: "Lingual Thyroid", feat: "Failure of descent; remains at tongue base; may be the only functioning thyroid tissue" },
{ cond: "Ectopic Thyroid", feat: "Arrested anywhere along descent path" },
{ cond: "Pyramidal Lobe", feat: "Present in ~50%; extends superiorly from isthmus (remnant of thyroglossal duct)" },
{ cond: "Thyroglossal Fistula", feat: "Persistent duct opening onto skin; often secondary to infected cyst" },
];
anomalies.forEach((a, i) => {
const yy = 2.92 + i * 0.49;
const bg = i % 2 === 0 ? "0D3B4F" : "112840";
sl.addShape("rect", { x: 0.3, y: yy, w: 9.4, h: 0.46, fill: { color: bg }, line: { color: "1F5068" } });
sl.addShape("rect", { x: 0.3, y: yy, w: 2.6, h: 0.46, fill: { color: "112840" }, line: { color: "1F5068" } });
sl.addText(a.cond, { x: 0.38, y: yy + 0.03, w: 2.45, h: 0.38, fontSize: 10, bold: true, color: C.accentPurp, fontFace: "Calibri", valign: "middle" });
sl.addText(a.feat, { x: 3.0, y: yy + 0.03, w: 6.6, h: 0.38, fontSize: 9.5, color: "D0E8F0", fontFace: "Calibri", valign: "middle" });
});
slideNumber(sl, 6); bottomBar(sl, C.accentPurp);
}
// =============================================================================
// SLIDE 7 – HISTOLOGY
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.accentGreen);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("HISTOLOGY OF THE THYROID GLAND", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
sectionPill(sl, "Histology", C.accentGreen, 7.5, 0.22);
// Histology image
sl.addImage({ data: IMG_HISTO, x: 5.35, y: 0.85, w: 4.4, h: 3.5 });
// Follicular cells
cardBox(sl, 0.25, 0.9, 4.85, 1.95, "F0FFF4", C.accentGreen);
sl.addShape("rect", { x: 0.25, y: 0.9, w: 4.85, h: 0.35, fill: { color: C.accentGreen }, line: { color: C.accentGreen } });
sl.addText("FOLLICULAR CELLS (THYROCYTES)", { x: 0.25, y: 0.9, w: 4.85, h: 0.35, fontSize: 10.5, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
const folItems = [
"Simple epithelium surrounding colloid-filled lumen",
"Active gland → tall columnar; Inactive → squamous",
"Apical: Golgi, secretory granules, lysosomes, microvilli",
"Basal: rich RER (protein synthesis)",
"Function: Synthesize T3 & T4 via thyroglobulin",
"Colloid stores enough hormone for ~3 months",
];
folItems.forEach((f, i) => {
sl.addText([
{ text: "● ", options: { color: C.accentGreen, bold: true } },
{ text: f, options: { color: C.textDark } },
], { x: 0.38, y: 1.3 + i * 0.25, w: 4.6, h: 0.24, fontSize: 9.5, fontFace: "Calibri" });
});
// C cells
cardBox(sl, 0.25, 3.0, 4.85, 1.75, "FFF0F5", C.accentPurp);
sl.addShape("rect", { x: 0.25, y: 3.0, w: 4.85, h: 0.35, fill: { color: C.accentPurp }, line: { color: C.accentPurp } });
sl.addText("PARAFOLLICULAR C CELLS", { x: 0.25, y: 3.0, w: 4.85, h: 0.35, fontSize: 10.5, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
const cCellItems = [
"Inside basal lamina of follicles or between follicles",
"Origin: Neural crest (ultimobranchial body / 4th pouch)",
"Larger than thyrocytes, paler staining",
"Secrete CALCITONIN → lowers serum Ca²⁺",
"Clinical: Source of Medullary Thyroid Carcinoma",
];
cCellItems.forEach((c, i) => {
sl.addText([
{ text: "◆ ", options: { color: C.accentPurp, bold: true } },
{ text: c, options: { color: C.textDark } },
], { x: 0.38, y: 3.42 + i * 0.26, w: 4.6, h: 0.24, fontSize: 9.5, fontFace: "Calibri" });
});
// Caption under image
sl.addText("H&E — Thyroid follicles with colloid (C) and follicular epithelium. Low power ×12 | Junqueira's Histology", {
x: 5.35, y: 4.4, w: 4.4, h: 0.4, fontSize: 8, italic: true, color: C.textMid, align: "center", fontFace: "Calibri",
});
slideNumber(sl, 7); bottomBar(sl, C.accentGreen);
}
// =============================================================================
// SLIDE 8 – HORMONES & PHYSIOLOGY
// =============================================================================
{
const sl = pres.addSlide();
darkBg(sl);
accentBar(sl, C.accent);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: "1A2A40" }, line: { color: "1A2A40" } });
sl.addText("HORMONES & PHYSIOLOGY", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
// T3 vs T4 comparison
const hormones = [
{ name: "T4 (Thyroxine)", detail: ["~90% secreted", "Less active (prohormone)", "Half-life: ~7 days", "Converted → T3 peripherally"], color: C.midTeal },
{ name: "T3 (Triiodothyronine)", detail: ["~10% secreted", "3–4× more potent", "Half-life: ~1 day", "Active form in tissues"], color: C.accent },
];
hormones.forEach((h, ci) => {
const xx = 0.3 + ci * 4.5;
sl.addShape("rect", { x: xx, y: 0.9, w: 4.2, h: 0.38, fill: { color: h.color }, line: { color: h.color } });
sl.addText(h.name, { x: xx, y: 0.9, w: 4.2, h: 0.38, fontSize: 13, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
sl.addShape("rect", { x: xx, y: 1.28, w: 4.2, h: 1.5, fill: { color: "0D3B4F" }, line: { color: h.color, width: 1.5 } });
h.detail.forEach((d, i) => {
sl.addText([{ text: "• ", options: { bold: true, color: h.color } }, { text: d, options: { color: "CCECF5" } }],
{ x: xx + 0.15, y: 1.32 + i * 0.36, w: 3.9, h: 0.33, fontSize: 11, fontFace: "Calibri" });
});
});
// HPT Axis
sl.addShape("rect", { x: 0.3, y: 2.95, w: 9.4, h: 0.33, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("HYPOTHALAMO-PITUITARY-THYROID (HPT) AXIS", {
x: 0.3, y: 2.95, w: 9.4, h: 0.33, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0,
});
const hptSteps = [
{ label: "Hypothalamus", sub: "TRH ↓", color: C.accentPurp },
{ label: "Ant. Pituitary", sub: "TSH ↓", color: C.midTeal },
{ label: "Thyroid Gland", sub: "T3 + T4", color: C.accentGreen },
{ label: "Target Tissues", sub: "↑ BMR etc.", color: C.accent },
{ label: "Neg. Feedback", sub: "↑T3/T4 → ↓TRH/TSH", color: C.accentRed },
];
hptSteps.forEach((s, i) => {
const xx = 0.3 + i * 1.88;
sl.addShape("rect", { x: xx, y: 3.32, w: 1.75, h: 0.85, fill: { color: s.color }, line: { color: s.color } });
sl.addText(s.label, { x: xx, y: 3.35, w: 1.75, h: 0.38, fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
sl.addText(s.sub, { x: xx, y: 3.7, w: 1.75, h: 0.3, fontSize: 9, color: C.white, align: "center", valign: "middle", margin: 0, italic: true });
if (i < 4) sl.addText("→", { x: xx + 1.75, y: 3.5, w: 0.12, h: 0.35, fontSize: 14, bold: true, color: C.accent, align: "center" });
});
// Actions
sl.addShape("rect", { x: 0.3, y: 4.3, w: 9.4, h: 0.3, fill: { color: C.accentGreen }, line: { color: C.accentGreen } });
sl.addText("KEY ACTIONS OF T3 / T4", {
x: 0.3, y: 4.3, w: 9.4, h: 0.3, fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle", margin: 0,
});
const actions = ["↑ BMR", "↑ Protein synthesis", "↑ Carbohydrate metabolism", "Essential for brain development", "Potentiates catecholamines", "Skeletal maturation"];
actions.forEach((a, i) => {
sl.addShape("rect", { x: 0.3 + i * 1.57, y: 4.62, w: 1.48, h: 0.72, fill: { color: "112840" }, line: { color: C.accentGreen, width: 1.5 } });
sl.addText(a, { x: 0.3 + i * 1.57, y: 4.62, w: 1.48, h: 0.72, fontSize: 9.5, color: "CCECF5", align: "center", valign: "middle", fontFace: "Calibri" });
});
slideNumber(sl, 8); bottomBar(sl, C.accent);
}
// =============================================================================
// SLIDE 9 – PATHOLOGY (HYPO / HYPER)
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.accentRed);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("THYROID PATHOLOGY — FUNCTIONAL DISORDERS", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 18, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
// Hypothyroidism
sl.addShape("rect", { x: 0.25, y: 0.88, w: 4.65, h: 0.38, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("HYPOTHYROIDISM (↓ T3/T4, ↑ TSH)", { x: 0.25, y: 0.88, w: 4.65, h: 0.38, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
cardBox(sl, 0.25, 1.26, 4.65, 3.1, "F0F8FF", C.teal);
const hypoItems = [
["Cause", "Hashimoto's thyroiditis (most common adult)"],
["Cause", "Iodine deficiency / post-thyroidectomy"],
["Cause", "Cretinism (congenital — mental retardation + dwarfism)"],
["Symptom", "Weight gain, cold intolerance, fatigue"],
["Symptom", "Bradycardia, constipation, dry skin"],
["Symptom", "Myxedema (non-pitting edema)"],
["Labs", "↑ TSH + ↓ T4 (primary)"],
["Rx", "Levothyroxine (T4 replacement)"],
];
hypoItems.forEach((h, i) => {
const tagColor = h[0] === "Cause" ? C.midTeal : h[0] === "Symptom" ? C.accentRed : h[0] === "Labs" ? C.accentGreen : C.accentPurp;
sl.addShape("rect", { x: 0.32, y: 1.3 + i * 0.37, w: 0.7, h: 0.28, fill: { color: tagColor }, line: { color: tagColor } });
sl.addText(h[0], { x: 0.32, y: 1.3 + i * 0.37, w: 0.7, h: 0.28, fontSize: 7.5, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
sl.addText(h[1], { x: 1.1, y: 1.32 + i * 0.37, w: 3.7, h: 0.28, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "middle" });
});
// Hyperthyroidism
sl.addShape("rect", { x: 5.1, y: 0.88, w: 4.65, h: 0.38, fill: { color: C.accentRed }, line: { color: C.accentRed } });
sl.addText("HYPERTHYROIDISM (↑ T3/T4, ↓ TSH)", { x: 5.1, y: 0.88, w: 4.65, h: 0.38, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
cardBox(sl, 5.1, 1.26, 4.65, 3.1, "FFF5F5", C.accentRed);
const hyperItems = [
["Cause", "Graves' disease (most common — TSH receptor Ab)"],
["Cause", "Toxic multinodular goiter / Toxic adenoma"],
["Cause", "Thyroiditis (De Quervain's, subacute)"],
["Symptom", "Weight loss, heat intolerance, sweating"],
["Symptom", "Tachycardia, palpitations, tremor"],
["Symptom", "Exophthalmos (Graves'), goiter"],
["Labs", "↓ TSH + ↑ T4/T3"],
["Rx", "Antithyroids / RAI / Surgery"],
];
hyperItems.forEach((h, i) => {
const tagColor = h[0] === "Cause" ? C.accentRed : h[0] === "Symptom" ? C.accent : h[0] === "Labs" ? C.accentGreen : C.teal;
sl.addShape("rect", { x: 5.17, y: 1.3 + i * 0.37, w: 0.7, h: 0.28, fill: { color: tagColor }, line: { color: tagColor } });
sl.addText(h[0], { x: 5.17, y: 1.3 + i * 0.37, w: 0.7, h: 0.28, fontSize: 7.5, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
sl.addText(h[1], { x: 5.95, y: 1.32 + i * 0.37, w: 3.7, h: 0.28, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "middle" });
});
// Divider
sl.addShape("rect", { x: 4.98, y: 0.88, w: 0.04, h: 3.5, fill: { color: C.accent }, line: { color: C.accent } });
slideNumber(sl, 9); bottomBar(sl, C.accentRed);
}
// =============================================================================
// SLIDE 10 – THYROID CANCERS
// =============================================================================
{
const sl = pres.addSlide();
darkBg(sl);
accentBar(sl, C.accentRed);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: "1A2A40" }, line: { color: "1A2A40" } });
sl.addText("THYROID MALIGNANCIES", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
const cancers = [
{
name: "Papillary Carcinoma",
freq: "~85% of cases",
origin: "Follicular cells",
spread: "Lymphatic → cervical LN",
features: ["\"Ground glass\" / Orphan Annie nuclei", "Psammoma bodies", "Papillary projections"],
prognosis: "Excellent (>95% 10-yr survival)",
assoc: "Radiation exposure; RET/PTC rearrangement",
color: C.accentGreen,
},
{
name: "Follicular Carcinoma",
freq: "~10% of cases",
origin: "Follicular cells",
spread: "Hematogenous → bone, lung",
features: ["Capsular + vascular invasion", "Cannot distinguish FNA from adenoma", "Cold nodule on scan"],
prognosis: "Good (70–80% survival)",
assoc: "Iodine deficiency areas; RAS mutation",
color: C.midTeal,
},
{
name: "Medullary Carcinoma",
freq: "~5% of cases",
origin: "C cells (parafollicular)",
spread: "Lymphatic + hematogenous",
features: ["Secretes calcitonin (↑ serum calcitonin)", "Amyloid deposits in stroma", "Bilateral if familial"],
prognosis: "Intermediate",
assoc: "MEN2A / MEN2B; RET mutation (familial)",
color: C.accentPurp,
},
{
name: "Anaplastic Carcinoma",
freq: "<1–2% of cases",
origin: "Follicular cells (undifferentiated)",
spread: "Rapid local invasion + distant mets",
features: ["Elderly patients", "Rapidly enlarging hard mass", "Compresses trachea/esophagus"],
prognosis: "Very poor (median survival <6 months)",
assoc: "Arises in pre-existing goiter; TP53 mutation",
color: C.accentRed,
},
];
cancers.forEach((c, i) => {
const xx = 0.22 + i * 2.4;
sl.addShape("rect", { x: xx, y: 0.9, w: 2.25, h: 0.4, fill: { color: c.color }, line: { color: c.color } });
sl.addText(c.name, { x: xx, y: 0.9, w: 2.25, h: 0.4, fontSize: 9.5, bold: true, color: C.white, align: "center", valign: "middle", margin: 0, wrap: true });
sl.addShape("rect", { x: xx, y: 1.3, w: 2.25, h: 3.95, fill: { color: "0D3B4F" }, line: { color: c.color, width: 1.5 } });
const rows = [
{ label: "Freq", val: c.freq },
{ label: "Origin", val: c.origin },
{ label: "Spread", val: c.spread },
{ label: "Features", val: c.features.join("; ") },
{ label: "Prognosis", val: c.prognosis },
{ label: "Assoc.", val: c.assoc },
];
rows.forEach((r, ri) => {
sl.addText(r.label, { x: xx + 0.06, y: 1.35 + ri * 0.63, w: 0.58, h: 0.25, fontSize: 7.5, bold: true, color: c.color, fontFace: "Calibri" });
sl.addText(r.val, { x: xx + 0.06, y: 1.59 + ri * 0.63, w: 2.1, h: 0.32, fontSize: 8.5, color: "C0DDE8", fontFace: "Calibri", wrap: true });
});
});
slideNumber(sl, 10); bottomBar(sl, C.accentRed);
}
// =============================================================================
// SLIDE 11 – SURGICAL ANATOMY & CLINICAL PEARLS
// =============================================================================
{
const sl = pres.addSlide();
lightBg(sl);
accentBar(sl, C.accent);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addText("SURGICAL ANATOMY & CLINICAL PEARLS", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 18, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
const pearls = [
{
num: "01",
title: "Recurrent Laryngeal Nerve",
body: "Must be identified & preserved during thyroidectomy. Passes near Berry's ligament and inferior thyroid artery. Unilateral injury → hoarseness; bilateral → stridor/airway obstruction.",
color: C.accentRed,
},
{
num: "02",
title: "Parathyroid Glands",
body: "4 small glands on posterior surface of lateral lobes. Accidental removal or devascularization → hypoparathyroidism → hypocalcemia → tetany. Monitor Ca²⁺ post-op.",
color: C.accentGreen,
},
{
num: "03",
title: "External Branch of Superior Laryngeal Nerve",
body: "Runs with superior thyroid artery (last 1 cm). Injury → voice fatigue, loss of high-pitched phonation (Semon's law).",
color: C.midTeal,
},
{
num: "04",
title: "Thyroid Ima Artery",
body: "Present in ~3%. Enters trachea from below — serious hemorrhage risk during emergency tracheostomy if undetected.",
color: C.accentPurp,
},
{
num: "05",
title: "Inferior Thyroid Veins",
body: "Drain directly into brachiocephalic veins. If torn during surgery → risk of AIR EMBOLISM. Always ligate before dividing.",
color: C.accent,
},
{
num: "06",
title: "Goiter",
body: "Diffuse enlargement (iodine deficiency or autoimmune). A midline neck swelling that moves on swallowing = thyroid/thyroglossal origin. Thyroglossal cyst also moves on tongue protrusion.",
color: C.teal,
},
];
pearls.forEach((p, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const xx = 0.25 + col * 4.88;
const yy = 0.9 + row * 1.55;
cardBox(sl, xx, yy, 4.6, 1.4, C.white, p.color);
sl.addShape("rect", { x: xx, y: yy, w: 0.55, h: 1.4, fill: { color: p.color }, line: { color: p.color } });
sl.addText(p.num, { x: xx, y: yy, w: 0.55, h: 1.4, fontSize: 18, bold: true, color: "FFFFFF", align: "center", valign: "middle", margin: 0 });
sl.addText(p.title, { x: xx + 0.62, y: yy + 0.06, w: 3.9, h: 0.3, fontSize: 11, bold: true, color: p.color, fontFace: "Calibri" });
sl.addText(p.body, { x: xx + 0.62, y: yy + 0.36, w: 3.9, h: 0.98, fontSize: 9, color: C.textDark, fontFace: "Calibri", wrap: true, valign: "top" });
});
slideNumber(sl, 11); bottomBar(sl, C.accent);
}
// =============================================================================
// SLIDE 12 – QUICK REVISION TABLE
// =============================================================================
{
const sl = pres.addSlide();
darkBg(sl);
accentBar(sl, C.accentGreen);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.75, fill: { color: "1A2A40" }, line: { color: "1A2A40" } });
sl.addText("QUICK REVISION — HIGH-YIELD SUMMARY", {
x: 0.3, y: 0, w: 9, h: 0.75, fontSize: 20, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
const rows = [
["Topic", "Key Fact", "Clinical Relevance"],
["Shape", "Butterfly; 2 lobes + isthmus", "Isthmus = 2nd–3rd tracheal rings"],
["Arterial supply", "Superior (ext. carotid) + Inferior (thyrocervical trunk)", "Ima artery = inconstant; risk in tracheostomy"],
["Venous drainage", "Superior + Middle → IJV; Inferior → Brachiocephalic", "Inferior veins: air embolism risk if torn"],
["Embryology", "Foramen cecum → thyroglossal duct → final position", "Cyst: Sistrunk's op; lingual thyroid = only TT"],
["Histology", "Follicles (thyrocytes + colloid) + C cells", "Active = tall columnar; Inactive = squamous"],
["C cell hormone", "Calcitonin → ↓ Ca²⁺", "Medullary carcinoma marker"],
["T3 vs T4", "T4 = prohormone; T3 = active; peripheral conversion", "Half-life T4 = 7 days; T3 = 1 day"],
["HPT Axis", "TRH → TSH → T3/T4 → neg. feedback", "Primary hypothyroid = ↑TSH; secondary = ↓TSH"],
["Surgical risk 1", "RLN — posteromedial to lateral lobe / Berry's lig.", "Hoarseness (uni) / Stridor (bilateral)"],
["Surgical risk 2", "Parathyroid glands (×4) on posterior surface", "Hypocalcemia → tetany if devascularized"],
];
rows.forEach((r, i) => {
const yy = 0.82 + i * 0.43;
const bg = i === 0 ? C.teal : i % 2 === 0 ? "0D3B4F" : "112840";
const textColor = i === 0 ? C.white : "C8E6F0";
const fontWeight = i === 0;
sl.addShape("rect", { x: 0.2, y: yy, w: 9.6, h: 0.41, fill: { color: bg }, line: { color: "1F5068" } });
const widths = [1.5, 4.4, 3.5];
const xs = [0.25, 1.8, 6.25];
r.forEach((cell, ci) => {
sl.addText(cell, {
x: xs[ci], y: yy + 0.02, w: widths[ci], h: 0.37,
fontSize: i === 0 ? 9.5 : 9,
bold: fontWeight,
color: i === 0 ? C.white : ci === 0 ? C.accent : textColor,
fontFace: "Calibri", valign: "middle",
});
});
});
slideNumber(sl, 12); bottomBar(sl, C.accentGreen);
}
// =============================================================================
// SLIDE 13 – THANK YOU / END
// =============================================================================
{
const sl = pres.addSlide();
darkBg(sl);
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.darkTeal }, line: { color: C.darkTeal } });
sl.addShape("rect", { x: 0, y: 0, w: 10, h: 0.08, fill: { color: C.accent }, line: { color: C.accent } });
sl.addShape("rect", { x: 0, y: 5.545, w: 10, h: 0.08, fill: { color: C.accent }, line: { color: C.accent } });
// Decorative anatomy image, faded
sl.addImage({ data: IMG_POSTERIOR, x: 5.5, y: 0.4, w: 4.2, h: 5.0, transparency: 60 });
sl.addText("THYROID GLAND", {
x: 0.5, y: 1.1, w: 5.5, h: 0.9, fontSize: 34, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 3,
});
sl.addText("Anatomy, Histology & Pathology", {
x: 0.5, y: 1.95, w: 5.5, h: 0.45, fontSize: 15, color: C.accent, fontFace: "Calibri",
});
sl.addShape("rect", { x: 0.5, y: 2.52, w: 4.8, h: 0.04, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText([
{ text: "Key References:\n", options: { bold: true, color: C.accent, breakLine: true } },
{ text: "• Gray's Anatomy for Students, 4th Ed\n", options: { color: "9FC8D8", breakLine: true } },
{ text: "• Junqueira's Basic Histology, 17th Ed\n", options: { color: "9FC8D8", breakLine: true } },
{ text: "• Vishram Singh — Head, Neck & Brain (Anatomy)\n", options: { color: "9FC8D8", breakLine: true } },
{ text: "• Robbins & Cotran Pathologic Basis of Disease", options: { color: "9FC8D8" } },
], {
x: 0.5, y: 2.65, w: 5.0, h: 1.8, fontSize: 10.5, fontFace: "Calibri", lineSpacingMultiple: 1.5,
});
sl.addText("Thank You", {
x: 0.5, y: 4.55, w: 5.0, h: 0.65, fontSize: 28, bold: true, color: C.midTeal, fontFace: "Calibri",
});
}
// ── Write file ────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/thyroid-ppt/Thyroid_Gland_Anatomy_Pathology.pptx" })
.then(() => console.log("✅ Presentation saved!"))
.catch(err => { console.error("❌ Error:", err); process.exit(1); });
cd /home/daytona/workspace/thyroid-ppt && node generate.js 2>&1
cd /home/daytona/workspace/thyroid-ppt && \ node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/2ec58523e023bd33efeb9ba12b34b76158eb9fa16b3ce47605088bd30921c13e.png" \ "https://cdn.orris.care/cdss_images/19be9b2bd67c8c5988f6b6824b31cf9145e5beaa01c0bb55873c22d25abeb182.png" \ "https://cdn.orris.care/cdss_images/8112f3e87edcb29f118fef612e489630e3c8386c93dcbfd8d7be79250ab9c8a0.png" \ "https://cdn.orris.care/cdss_images/2fb6e4f63998fbbbb982c4887d732b2db9ac3d4d35c7cc9d74cc61710f1ded02.png" \ > /home/daytona/workspace/thyroid-ppt/images.json && echo "Saved" && wc -c /home/daytona/workspace/thyroid-ppt/images.json
~/thyroid-ppt/generate.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/thyroid-ppt/generate.js'
~/thyroid-ppt/generate.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/thyroid-ppt/generate.js'
cd /home/daytona/workspace/thyroid-ppt && node generate.js 2>&1
ls -lh /home/daytona/workspace/thyroid-ppt/Thyroid_Gland_Anatomy_Pathology.pptx
Thyroid Gland Anatomy Pathology
Presentation · PPTX
What's inside - 13 slides, dark teal + gold colour scheme
| Slide | Title | Highlights |
|---|---|---|
| 1 | Title Slide | Dark design with anatomy diagram on right panel |
| 2 | Location & Shape | Colour-coded fact cards + labelled anatomy diagram |
| 3 | Anatomical Relations | 3-column layout: Anterior / Posterior / Lateral with Berry's ligament warning |
| 4 | Blood Supply | Arteries + veins with vasculature diagram |
| 5 | Lymphatics & RLN | Lymph nodes + RLN surgical importance with posterior view |
| 6 | Embryology | Step-by-step flow + anomalies table (thyroglossal cyst, lingual thyroid, etc.) |
| 7 | Histology | Follicular cells vs C cells with real H&E micrograph |
| 8 | Hormones & Physiology | T3 vs T4 comparison + HPT axis + actions |
| 9 | Functional Disorders | Hypothyroidism vs Hyperthyroidism side-by-side |
| 10 | Thyroid Cancers | All 4 types: Papillary, Follicular, Medullary, Anaplastic with key features |
| 11 | Surgical Anatomy | 6 numbered clinical pearls (RLN, parathyroids, ima artery, air embolism etc.) |
| 12 | Quick Revision Table | High-yield exam summary table |
| 13 | References / End | Vishram Singh, Gray's, Junqueira's, Robbins |