Hypercalcemia workup
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypercalcemia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced material. Let me compile the full response.
Hypercalcemia Workup
Step 1 - Confirm True Hypercalcemia
Before anything else, verify the result is real:
- Serum total calcium > 10.5 mg/dL (2.6 mmol/L), or ionized calcium > 5.3 mg/dL (1.3 mmol/L)
- Rule out false hypercalcemia due to: tourniquet not released during phlebotomy, prolonged venous stasis, hemolysis, or lab error
- Correct for albumin: corrected Ca = measured Ca + 0.8 × (4.0 - serum albumin). Alternatively, measure ionized calcium directly - this bypasses albumin entirely
- Obtain repeat measurements (serum Ca + albumin, at least twice, non-fasting) - this is cost-effective and important before extensive workup
Harrison's Principles of Internal Medicine 22E (2025): "Hyperparathyroidism and cancer account for 90% of all cases."
Step 2 - Clinical History and Chronicity
This is the most important filter before ordering labs:
| Feature | Points toward |
|---|---|
| Chronic hypercalcemia (> 1 year) | Primary hyperparathyroidism (PHPT) |
| Acute or short history | Malignancy (usually becomes evident within months) |
| Asymptomatic | > 90% of PHPT cases |
| "Bones, stones, moans, abdominal groans" | Classic PHPT symptom quadrad |
| Rapid progression, constitutional symptoms | Malignancy |
| Medications (lithium, thiazides, vitamin D, calcium carbonate) | Drug-induced |
| Family history of hypercalcemia | FHH (Familial Hypocalciuric Hypercalcemia) |
| Renal failure + dialysis history | Tertiary HPT or aluminum intoxication |
| Sarcoidosis, TB, fungal infection history | Granulomatous disease |
Step 3 - Initial Laboratory Panel
| Test | Rationale |
|---|---|
| Serum intact PTH (immunometric/two-site assay) | Single most useful test - separates parathyroid from non-parathyroid causes |
| Serum albumin | Correct calcium |
| BMP/CMP (BUN, creatinine, phosphate, CO2) | Assess renal function; low phosphate supports HPT |
| Spot urine Ca:Cr ratio (or 24-hour urine calcium) | Differentiates PHPT from FHH |
| Magnesium | Hypomagnesemia affects PTH secretion |
Step 4 - PTH-Directed Algorithm
The two algorithms below (from Brenner & Rector and Harrison's) guide further testing:
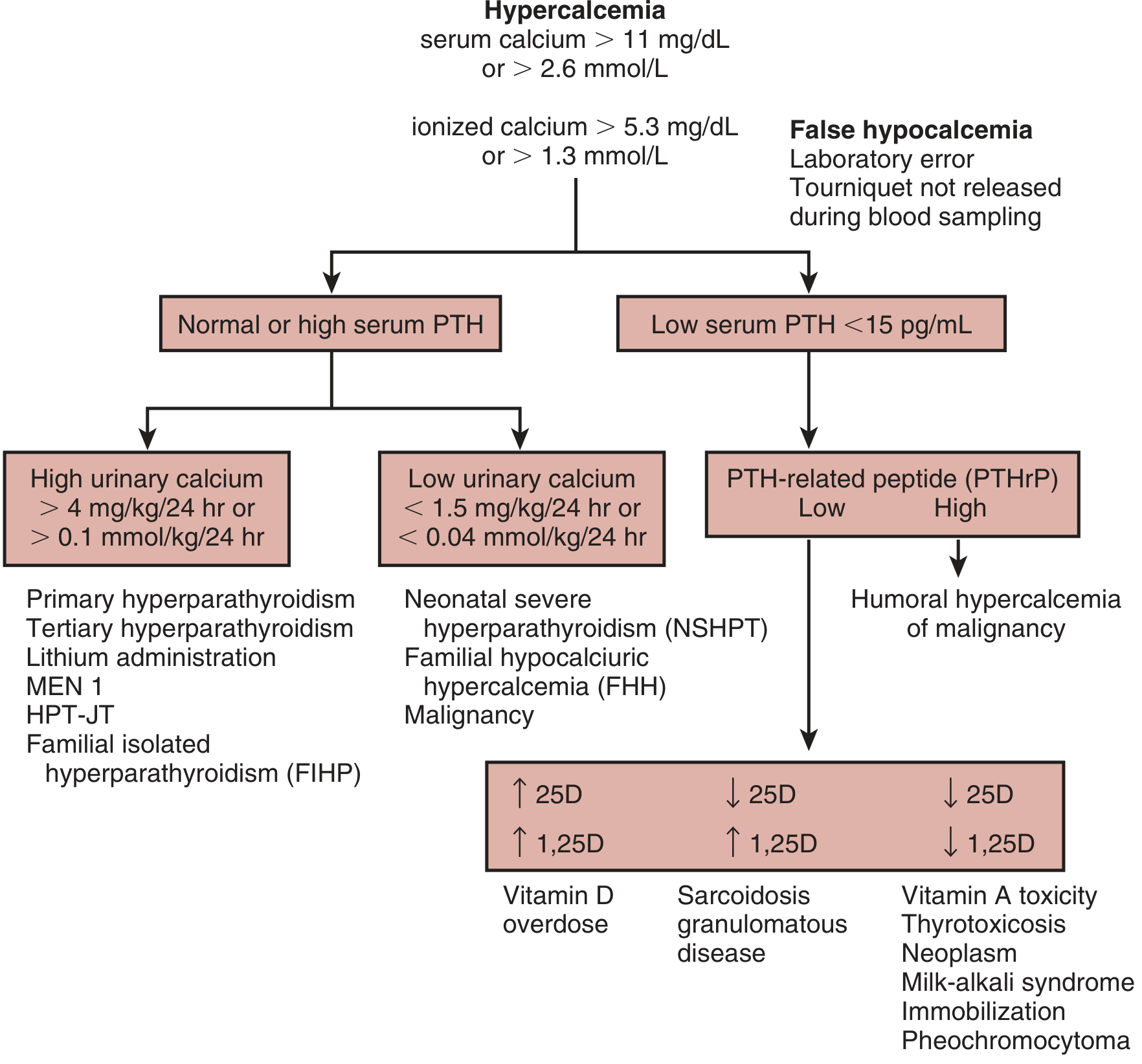
Algorithm for diagnosis of hypercalcemia based on PTH level and urinary calcium excretion - Brenner and Rector's The Kidney
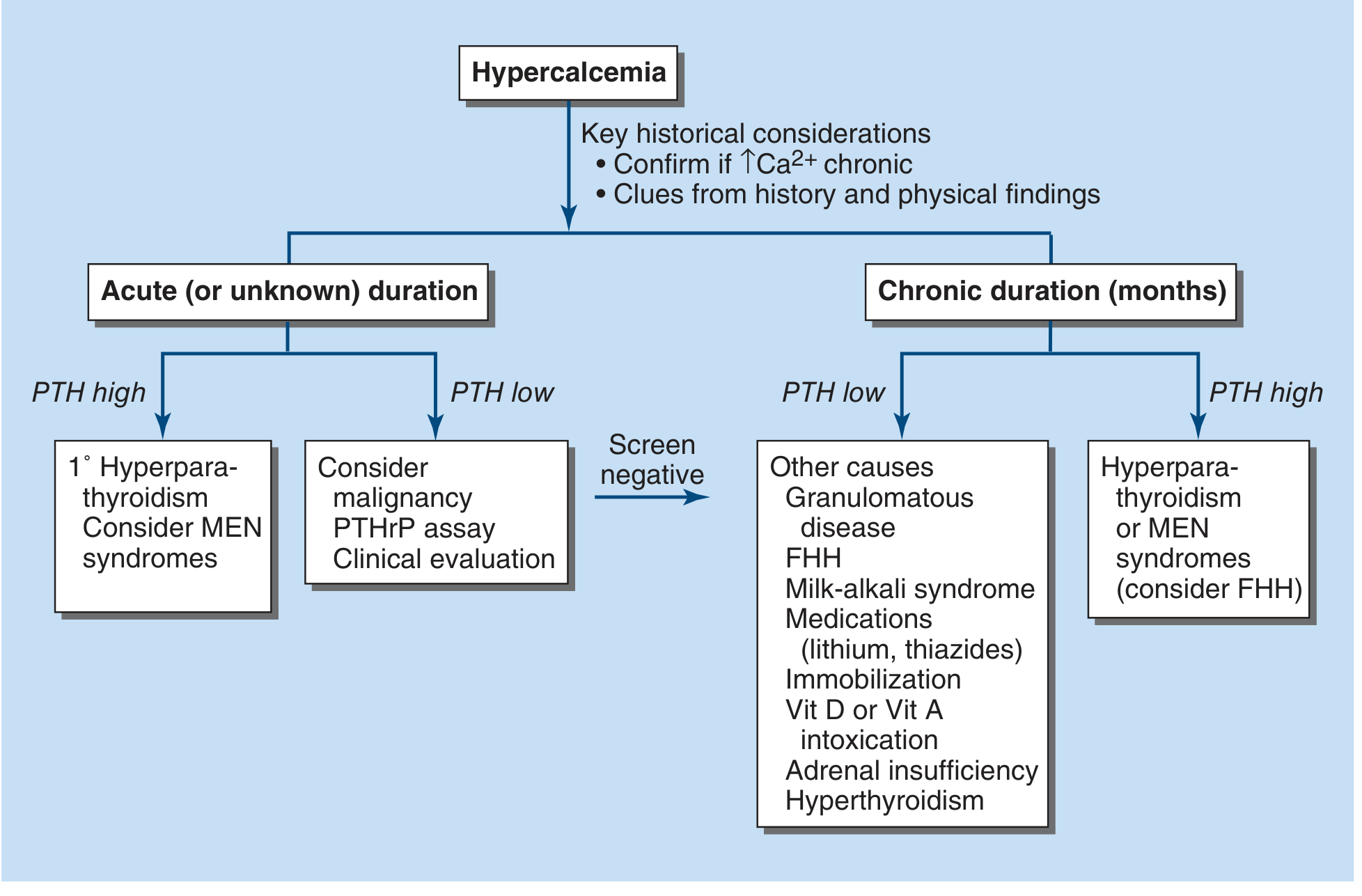
Harrison's Principles of Internal Medicine 22E (2025) - Fig. 422-6: Evaluation by chronicity and PTH level
PTH Elevated or Normal-High (Inappropriately Unsuppressed)
- Check 24-hour urine calcium:
- High urine Ca > 4 mg/kg/24 hr (> 0.1 mmol/kg/24 hr): Primary HPT, tertiary HPT, MEN 1, HPT-JT syndrome, lithium use, familial isolated HPT (FIHP)
- Low urine Ca < 1.5 mg/kg/24 hr (< 0.04 mmol/kg/24 hr): Familial Hypocalciuric Hypercalcemia (FHH) - confirm with family history and genetic testing (CASR mutation)
- Consider MEN syndromes (check for pituitary tumors, pancreatic NETs in MEN1; pheochromocytoma in MEN2A)
PTH Low (< 15 pg/mL) - PTH Suppressed
Check PTHrP:
- PTHrP elevated: Humoral hypercalcemia of malignancy (HHM) - most often squamous cell carcinomas (lung, head/neck, esophagus), renal, bladder
- PTHrP low/normal: Proceed to vitamin D metabolites
Check 25-hydroxyvitamin D (25-OHD) and 1,25-dihydroxyvitamin D (1,25-OHD2):
| 25-OHD | 1,25-OHD2 | Interpretation |
|---|---|---|
| High | High | Vitamin D overdose/intoxication |
| Low/normal | High | Sarcoidosis, granulomatous disease (TB, histoplasma, berylliosis), certain lymphomas |
| Low | Low | Vitamin A toxicity, thyrotoxicosis, neoplasm with osteolytic mets, milk-alkali syndrome, immobilization, pheochromocytoma |
Step 5 - Cause-Specific Additional Tests
If malignancy suspected (suppressed PTH, short history):
- Chest X-ray + CT chest/abdomen/pelvis
- Bone scan (note: may be negative in multiple myeloma)
- SPEP/UPEP + serum free light chains (myeloma)
- PSA, mammography as appropriate
- PTHrP assay
If primary hyperparathyroidism confirmed:
- Localization studies (only if parathyroid surgery planned): Sestamibi parathyroid scan, neck ultrasound, 4D CT
- DEXA bone density (T-score at lumbar spine, hip, distal 1/3 radius)
- 24-hour urine calcium and creatinine
- Serum creatinine, renal ultrasound (nephrolithiasis screening)
- 25-OHD level (vitamin D deficiency common in PHPT)
- Consider 24-hour urine for kidney stone risk panel if nephrolithiasis present
- Genetic testing for MEN1/2, HRPT2, CASR if young patient or family history
If FHH suspected:
- Calcium:creatinine clearance ratio (CCCR) = (urine Ca/serum Ca) ÷ (urine Cr/serum Cr)
- CCCR < 0.01 strongly suggests FHH
- CCCR > 0.02 supports PHPT
- Family history screening
- CASR, AP2S1, GNA11 genetic panel
If granulomatous disease suspected:
- 1,25-OHD2 (elevated due to extrarenal 1-alpha hydroxylase)
- ACE level, chest CT (sarcoidosis)
- BAL or tissue biopsy if needed
Causes Summary (Table)
| Category | Specific Causes |
|---|---|
| Parathyroid-related | PHPT (adenoma 80%, hyperplasia 15%, carcinoma <1%), MEN 1/2A, FHH, HPT-JT syndrome, lithium, tertiary HPT |
| Malignancy | Osteolytic mets (breast, myeloma, lymphoma), HHM via PTHrP (squamous, renal, bladder), hematologic (lymphoma - via 1,25D) |
| Vitamin D-related | Vitamin D intoxication, granulomatous disease (sarcoid, TB, fungal), lymphomas |
| High bone turnover | Hyperthyroidism, immobilization, Paget's disease |
| Renal | Tertiary HPT, aluminum intoxication |
| Drug/Ingestion | Thiazides, lithium, vitamin A toxicity, milk-alkali syndrome (CaCO3 + absorbable alkali) |
| Endocrine | Adrenal insufficiency, pheochromocytoma, VIPoma |
Quick Reference: PTH Interpretation
| Serum PTH | Serum Ca | Interpretation |
|---|---|---|
| Elevated | High | PHPT, tertiary HPT, FHH, lithium |
| Normal (unsuppressed) | High | PHPT (early/mild), FHH |
| Low/undetectable | High | Malignancy, vitamin D toxicity, granulomatous disease, immobilization, thiazides |
| Very high | Low | Secondary HPT (renal disease, malabsorption) - not hypercalcemia |
PTH is elevated in > 90% of parathyroid-related hypercalcemia and undetectable or low in malignancy-related, vitamin D-related, and high-bone-turnover causes. Measurement of PTH is cost-effective in virtually all hypercalcemic patients. - Harrison's Principles of Internal Medicine 22E, 2025
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill) | Brenner and Rector's The Kidney | Textbook of Family Medicine 9e | Sabiston Textbook of Surgery
Hypercalcemia workup
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypercalcemia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive data from multiple authoritative sources. Here is the full workup:
Hypercalcemia Workup
Hypercalcemia is defined as serum total calcium > 10.5 mg/dL (2.6 mmol/L) or ionized calcium > 5.3 mg/dL (1.3 mmol/L). Hyperparathyroidism and malignancy together account for 90% of all cases. - Harrison's Principles of Internal Medicine 22E (2025)
Step 1 - Confirm True Hypercalcemia
Before ordering any further tests, rule out spurious results:
- Repeat the measurement - obtain serum calcium + albumin at least twice (non-fasting); this is cost-effective since hypercalcemia is typically chronic
- Correct for albumin: Corrected Ca = measured Ca + 0.8 × (4.0 - serum albumin g/dL)
- Measure ionized calcium directly if albumin correction is unreliable (paraproteinemia, critical illness) - Rosen's Emergency Medicine recommends ionized Ca over total Ca in hypercalcemic patients
- Rule out false hypercalcemia: tourniquet not released during phlebotomy (hemoconcentration), hemolysis, lab error
Step 2 - Severity Classification
| Grade | Total Ca (mg/dL) | Management urgency |
|---|---|---|
| Mild | < 12 | Outpatient, usually hydration |
| Moderate | 12-14 | More aggressive management needed |
| Severe | > 14 | Life-threatening, emergency measures |
Step 3 - History and Clinical Context (Most Important Filter)
| Finding | Suggests |
|---|---|
| Chronic (> 1 year), asymptomatic | Primary hyperparathyroidism (> 90% are asymptomatic) |
| Acute onset, rapid progression, constitutional symptoms | Malignancy (usually evident within months) |
| "Bones, stones, moans, abdominal groans" | Classic PHPT symptom quadrad |
| Family history of hypercalcemia | Familial Hypocalciuric Hypercalcemia (FHH) |
| Sarcoidosis, TB, fungal disease, berylliosis | Granulomatous disease |
| Medications: lithium, thiazides, Vit D/A supplements, calcium carbonate + antacids | Drug-induced |
| Dialysis patient | Tertiary HPT or aluminum intoxication |
| Young patient, jaw tumor, renal tumor | HPT-JT syndrome (CDC73 mutation) |
| MEN1 clues (pituitary, pancreatic symptoms) | MEN1 with PHPT |
Step 4 - Initial Laboratory Panel
These should be ordered together at first evaluation:
| Test | Purpose |
|---|---|
| Serum intact PTH (two-site immunometric assay) | Single most useful test - separates parathyroid from non-parathyroid causes |
| Serum albumin | Correct total calcium |
| BMP: creatinine, BUN, phosphate, CO2, potassium | Renal function; low phosphate supports HPT |
| Spot urine calcium:creatinine ratio or 24-hour urine calcium | Distinguish PHPT from FHH |
| Magnesium | Low Mg impairs PTH secretion |
| CBC | Anemia raises concern for myeloma |
Step 5 - PTH-Directed Algorithm
The two diagnostic algorithms below guide the next steps based on PTH result:
Fig. 73.11 - Brenner & Rector's The Kidney (PTH + urinary calcium branch):
Fig. 422-6 - Harrison's Principles of Internal Medicine 22E (2025) (chronicity + PTH branch):
PTH Elevated or Normal-Unsuppressed
PTH is elevated in > 90% of parathyroid-related hypercalcemia.
Check 24-hour urine calcium (or spot urine Ca:Cr ratio):
High urine calcium (> 4 mg/kg/24 hr or > 0.1 mmol/kg/24 hr):
- Primary hyperparathyroidism (PHPT) - adenoma 80%, hyperplasia 15%, carcinoma < 1%
- Tertiary hyperparathyroidism
- Lithium therapy
- MEN 1 or MEN 2A
- HPT-JT syndrome, Familial isolated HPT (FIHP)
Low urine calcium (< 1.5 mg/kg/24 hr or < 0.04 mmol/kg/24 hr):
- Familial Hypocalciuric Hypercalcemia (FHH) - CASR inactivating mutation
- Neonatal severe hyperparathyroidism (NSHPT)
- Some malignancies
To distinguish FHH from PHPT: calculate the Calcium:Creatinine Clearance Ratio (CCCR):
CCCR = (urine Ca / serum Ca) ÷ (urine Cr / serum Cr)
- CCCR < 0.01 = strongly favors FHH
- CCCR > 0.02 = favors PHPT
PTH Low (< 15 pg/mL) - Suppressed
PTH is undetectable or low in malignancy-related, vitamin D-related, and high-bone-turnover causes.
Next: check PTHrP
- PTHrP elevated: Humoral Hypercalcemia of Malignancy (HHM) - accounts for ~80% of malignancy-related hypercalcemia; classic tumors: squamous cell (lung, head/neck, esophagus, cervix), renal cell, bladder, ovarian
- PTHrP low/normal: check vitamin D metabolites
Next: check 25-OHD and 1,25-OHD2
| 25-OHD | 1,25-OHD2 | Diagnosis |
|---|---|---|
| High | High | Vitamin D overdose/intoxication |
| Low/normal | High | Sarcoidosis, granulomatous disease (TB, histoplasmosis, berylliosis), certain lymphomas (Hodgkin, NHL) - via macrophage 1α-hydroxylase |
| Low | Low | Vitamin A toxicity, thyrotoxicosis, osteolytic metastases, milk-alkali syndrome, immobilization, pheochromocytoma, adrenal insufficiency |
Step 6 - Cause-Specific Follow-Up Tests
If PHPT confirmed (elevated PTH, high urine Ca):
- Localization (only if surgery planned): Sestamibi parathyroid scan ± neck ultrasound ± 4D CT
- DEXA bone densitometry (lumbar spine, hip, distal 1/3 radius - the latter most sensitive for cortical loss in PHPT)
- 24-hour urine calcium/creatinine + stone risk panel if nephrolithiasis
- 25-OHD level (vitamin D deficiency is common and must be repleted carefully)
- Serum creatinine + renal imaging (nephrolithiasis, nephrocalcinosis)
- Genetic testing if age < 40, multiglandular disease, family history, or jaw tumor: MEN1, CDC73 (HRPT2), CASR, AP2S1
If malignancy suspected (low PTH, short history, rapid course):
- PTHrP assay
- SPEP/UPEP + serum free light chains (multiple myeloma - note bone scan may be negative)
- CT chest/abdomen/pelvis
- Chest X-ray
- Bone scan (lytic mets)
- PSA, mammography as clinically indicated
- 1,25-OHD2 (lymphoma)
If granulomatous disease suspected:
- 1,25-OHD2 (elevated due to extrarenal 1α-hydroxylase in macrophages)
- ACE level, chest CT (sarcoidosis)
- Tissue biopsy or BAL if needed
If FHH suspected:
- CCCR calculation
- Family history screening (autosomal dominant; calcium often mildly elevated in relatives)
- Genetic panel: CASR, AP2S1, GNA11
Summary: Causes by PTH Status
| PTH Status | Causes |
|---|---|
| Elevated / Unsuppressed | PHPT (adenoma, hyperplasia, carcinoma), MEN 1/2A, lithium, FHH, tertiary HPT, NSHPT, HPT-JT, ectopic PTH (rare) |
| Suppressed + PTHrP high | Humoral hypercalcemia of malignancy (squamous, renal, bladder) |
| Suppressed + 1,25D high | Sarcoidosis, TB, lymphoma, granulomatous disease |
| Suppressed + both Vit D low | Osteolytic mets, thyrotoxicosis, Vit A toxicity, milk-alkali, immobilization, adrenal insufficiency, pheochromocytoma |
| Suppressed + 25D and 1,25D both high | Vitamin D intoxication |
ECG Pearl
In severe/acute hypercalcemia: shortened QT interval progressing to dysrhythmias and heart block. - Rosen's Emergency Medicine
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill)
- Brenner and Rector's The Kidney, 2-Volume Set
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Textbook of Family Medicine 9e
- 2025 Practice Guideline: Bouillet B et al., "Primary Hyperparathyroidism: diagnosis," Ann Endocrinol (Paris) [PMID: 39818287]
Treatment
Finding Sources
Finding Sources
Searching PubMed
"hypercalcemia"[MeSH Terms] AND "therapy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - I have the full treatment table from Harrison's 22E and dosing from multiple authoritative sources. Here is the complete treatment guide:
Hypercalcemia Treatment
Treatment is stratified by severity and guided by the underlying cause. The immediate priority is lowering calcium to relieve symptoms; treating the cause is the second priority.
Severity Thresholds
| Severity | Total Ca (mg/dL) | Approach |
|---|---|---|
| Mild | < 12 | Hydration; outpatient management often adequate |
| Moderate | 12-14 | Aggressive IV fluids + antiresorptive agents |
| Severe / crisis | > 14 | Emergency combination therapy; may need dialysis |
Acute Management - Step-by-Step Order
1. IV Normal Saline (First and Always)
- Mechanism: expands ECF, increases GFR, reduces proximal tubular Na⁺ and Ca²⁺ reabsorption, promotes calciuresis
- Most patients are volume-depleted at presentation from hypercalcemia-induced polyuria and natriuresis
- Dose: 200-500 mL/hr based on cardiovascular status; maintain urine output 100-150 mL/hr
- Expected effect: serum Ca falls ~1-3 mg/dL within 24 h
- Monitor closely for volume overload, especially in cardiac/renal impairment
- Onset: hours; Duration: only during infusion
2. Loop Diuretics (after euvolemia is restored)
- Mechanism: block NKCC2 in the thick ascending limb, disrupting the electrochemical gradient for passive paracellular Ca²⁺ reabsorption
- Furosemide 20-40 mg IV; dose adjusted for renal function
- Critical: must be given only after adequate volume resuscitation - loop diuretics before hydration will worsen hypercalcemia by causing further dehydration
- Replete K⁺ and Mg²⁺ aggressively
- Combined saline + furosemide can increase urine Ca excretion to ≥ 500 mg/day
3. IV Bisphosphonates (backbone of antiresorptive therapy)
Bisphosphonates are pyrophosphate analogues with high affinity for bone in areas of high turnover. Amino-bisphosphonates interfere with protein prenylation and induce osteoclast apoptosis.
| Drug | Dose | Infusion | Notes |
|---|---|---|---|
| Pamidronate | 60 mg (Ca 12-13.5 mg/dL) or 90 mg (Ca > 13.5 mg/dL) | Over 2-4 hrs | Onset 1-2 days; duration 10-14 days to weeks |
| Zoledronate | 4 mg | Over ≥ 15 min | More potent; duration > 3 weeks; preferred agent |
- Clinical response seen in 2-4 days; Ca nadir reached in 4-7 days
- Can repeat pamidronate after 7 days if hypercalcemia recurs
- Hydrate before infusing - rapid infusion without hydration risks acute kidney injury
- Renal insufficiency is a relative contraindication; dose-adjust or avoid
- Adverse effects: fever (~20%), hypophosphatemia, hypocalcemia, hypomagnesemia; rarely osteonecrosis of the jaw
4. Calcitonin (adjunct for rapid bridging)
- Mechanism: inhibits osteoclast-mediated bone resorption AND increases renal calcium excretion
- Dose: Salmon calcitonin 4-8 IU/kg IM or SC every 6-12 hours
- Lowers Ca by 1-2 mg/dL within hours in 60-70% of patients
- Key limitation: rapid tachyphylaxis - effect lost after 1-2 days; use as bridge while waiting for bisphosphonates to kick in
- Advantages: safe in renal failure, may have analgesic effect in bone mets, no serious toxicity
- Onset: hours; Duration: 1-2 days only
5. Denosumab (for refractory or bisphosphonate-ineligible patients)
- Mechanism: RANKL inhibitor - blocks osteoclast differentiation and function (most potent antiresorptive)
- Dose: 120 mg SC every 4 weeks (some protocols: weekly × 4 weeks then monthly for malignancy)
- Indications: hypercalcemia refractory to bisphosphonates; CKD where bisphosphonates are contraindicated
- Adverse effects: severe hypocalcemia (especially in CKD), jaw osteonecrosis, skin infections
- Monitor calcium closely after administration
6. Glucocorticoids (specific indications)
- Mechanism: inhibit extrarenal 1α-hydroxylase (which converts 25-OHD to 1,25-OHD2 in macrophages), and direct antitumor effect in hematologic malignancies
- Dose: Prednisone 20-60 mg/day PO; taper to minimum effective dose once Ca stabilizes
- Effective specifically in:
- Granulomatous disease (sarcoidosis, TB, fungal)
- Vitamin D intoxication
- Hematologic malignancies (myeloma, lymphoma)
- Not effective for PHPT or solid-tumor humoral hypercalcemia
7. Dialysis (last resort)
- Indications: severe hypercalcemia (Ca > 16 mg/dL) with concurrent CHF or renal insufficiency where aggressive saline loading is not feasible
- Hemodialysis or peritoneal dialysis with low-calcium dialysate
- Onset: hours; can immediately reverse life-threatening hypercalcemia
- Reserved for extreme or special circumstances
Summary Table (Harrison's 22E, Table 422-4)
| Treatment | Onset | Duration | Best use |
|---|---|---|---|
| IV NS | Hours | Infusion only | Always first; universal |
| Forced diuresis (NS + loop diuretic) | Hours | During treatment | Moderate-severe; after rehydration |
| Calcitonin | Hours | 1-2 days | Bridge in severe/acute; safe in renal failure |
| Pamidronate | 1-2 days | 10-14 days to weeks | Malignancy, moderate-severe |
| Zoledronate | 1-2 days | > 3 weeks | Preferred bisphosphonate |
| Denosumab | 1-2 days | > 3 weeks | Refractory; CKD; strongest antiresorptive |
| Glucocorticoids | Days | Days-weeks | Granulomatous disease, lymphoma, Vit D toxicity |
| Oral phosphate | 24 hrs | During use | Hypophosphatemia + chronic low-level management |
| Dialysis | Hours | 24-48 hrs after | Renal failure + severe hypercalcemia |
Cause-Specific Chronic Management
Primary Hyperparathyroidism (PHPT)
Parathyroidectomy is the definitive treatment. Indications (per 5th International Workshop guidelines):
- Corrected serum Ca > 1.0 mg/dL above the upper limit of normal
- Creatinine clearance < 60 mL/min
- Age < 50 years
- T-score ≤ -2.5 at lumbar spine, total hip, femoral neck, or distal 1/3 radius on DXA, or prior fragility fracture
- 24-hour urine Ca > 400 mg/day with elevated stone risk
- Imaging-confirmed nephrolithiasis or nephrocalcinosis
- Patient preference (does not meet criteria but declines surveillance)
Surgery has ~95% success rate with low morbidity.
Medical management (for non-surgical candidates):
- Liberal oral hydration + high-salt diet
- Daily physical activity (reduces bone resorption from immobility)
- Avoid thiazide diuretics and prolonged immobilization
- Cinacalcet (calcimimetic): allosteric activator of CaSR that mimics high Ca, suppressing PTH secretion
- Dose: 30 mg BID titrated up to 90 mg BID; give with food to reduce nausea
- Reduces PTH and serum Ca; does not improve bone density
- Oral bisphosphonates (alendronate): improves bone density but minimal effect on Ca levels
- Estrogen/raloxifene in postmenopausal women: modest bone-protective effect
Surveillance (if not meeting surgical criteria): annual serum Ca + creatinine, DXA every 1-2 years, vertebral fracture imaging
Malignancy-Associated Hypercalcemia
- IV bisphosphonates (zoledronate preferred) + denosumab for refractory cases
- Glucocorticoids + Ca-restricted diet (< 400 mg/day) for lymphoma/myeloma
- These measures rarely give long-term control unless the malignancy itself responds to treatment
- Median survival after malignancy-associated hypercalcemia is < 2 months (reflects advanced disease)
Granulomatous Disease / Vitamin D Toxicity
- Glucocorticoids are first-line alongside saline diuresis
- Dietary calcium restriction is beneficial (unlike malignancy, pathogenesis is intestinal hyperabsorption)
- Avoid sunlight exposure (reduces endogenous Vit D production) in active granulomatous disease
- Hydroxychloroquine is an alternative for steroid-sparing in sarcoidosis
FHH
- No treatment needed - benign, parathyroidectomy does not cure it
- Avoid unnecessary parathyroid surgery
Sources:
- Harrison's Principles of Internal Medicine 22E (2025) - Table 422-4
- Washington Manual of Medical Therapeutics
- NKF Primer on Kidney Diseases 8e
- Rosen's Emergency Medicine
- Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.