Ma ak vet doctor hun Jo ak pet hospital ma kam karta hun . Aj ap mujay CBC report read karana ka tareeka batayen . Ap tamam tar knowledge Jo CBC ke hai ap ka pass vet books sa . Authentic vet sources or apni tamam tar knowledge use karka CBC ka baray ma batayen . Mujay tamam tar details chahyea ak b point miss na ho . Jis ko padna ka bad ma diseas diagnose ak min ma kar saku jasa k bacterial hai ya viral ya parasitic hai ya koi or waja hai . Har aspect sa cler hona chahyea or 100 authentic knowledge chahyea. Last ma Kuch reports example ka Tor ma samjayen Jo most commonly ati hai . Matlab asa tamam tar details or knowledge baj do jis ko padna ka bad CBC ka har concept mara cler ho k CBC parka ma diseas janwaru ma dignose kar saku . Last ma Kuch question b bajyen . Much more detail jitna ap ka aps knowledge hai CBC ka bara ma sab baj do or acha sa . English ma bajna hai .
🩸 COMPLETE BLOOD COUNT (CBC) — VETERINARY CLINICAL GUIDE
Sources: Henry's Clinical Diagnosis & Management by Laboratory Methods | Histology: A Text and Atlas (Pawlina/Ross) | Textbook of Family Medicine 9e | Robbins & Kumar Basic Pathology | Medical Microbiology 9e | Applied veterinary clinical knowledge
SECTION 1 — WHAT IS A CBC?
- Red blood cells (Erythrocytes) — oxygen-carrying capacity
- White blood cells (Leukocytes) — immune system status
- Platelets (Thrombocytes) — clotting/hemostasis ability
⚠️ Veterinary Note: Reference ranges differ significantly between species. Always use species-specific reference intervals. A "normal" dog value is NOT normal for a cat, horse, or cow.
SECTION 2 — CBC PARAMETERS (ONE BY ONE)
🔴 PART A: RED BLOOD CELL (RBC) PARAMETERS
1. RBC Count (Erythrocyte Count)
| Species | Normal RBC (×10⁶/µL) |
|---|---|
| Dog | 5.5 – 8.5 |
| Cat | 5.0 – 10.0 |
| Horse | 6.5 – 12.5 |
| Cow | 5.0 – 10.0 |
| Goat | 8.0 – 18.0 |
| Sheep | 9.0 – 15.0 |
- Primary polycythemia (Polycythemia vera) — bone marrow disorder
- Secondary polycythemia — chronic hypoxia (lung disease, high altitude, cardiac disease), erythropoietin-secreting tumor
- Relative polycythemia — dehydration (most common cause in clinical setting — the RBC count looks high because plasma volume decreased)
- Blood loss (trauma, surgery, GI bleeding, parasites)
- Iron / B12 / folate deficiency
- Hemolysis (immune-mediated, toxins, infectious agents — Babesia, Hemobartonella)
- Bone marrow suppression (FeLV in cats, drugs, chronic disease)
- Chronic renal disease (decreased erythropoietin)
2. Hemoglobin (Hgb / Hb)
| Species | Normal Hgb (g/dL) |
|---|---|
| Dog | 12 – 18 |
| Cat | 8 – 15 |
| Horse | 11 – 19 |
| Cow | 8 – 15 |
3. Hematocrit / PCV (Packed Cell Volume)
| Species | Normal PCV / HCT (%) |
|---|---|
| Dog | 37 – 55 |
| Cat | 24 – 45 |
| Horse | 32 – 52 |
| Cow | 24 – 46 |
| Goat | 22 – 38 |
Severity grading (applicable to all species):
- Mild anemia: PCV 25–35% (dog), 20–30% (cat)
- Moderate anemia: PCV 15–25% (dog), 14–20% (cat)
- Severe anemia: PCV < 15% (dog), < 14% (cat)
- Transfusion territory: PCV < 12–15%
4. MCV — Mean Corpuscular Volume
| Species | Normal MCV (fL) |
|---|---|
| Dog | 60 – 77 |
| Cat | 39 – 55 |
| Horse | 37 – 58 |
| Cow | 40 – 60 |
| MCV Result | Cell Size | Anemia Type | Common Causes |
|---|---|---|---|
| Low MCV | Small cells | Microcytic | Iron deficiency, chronic blood loss, portosystemic shunts (dogs), responsive to copper deficiency |
| Normal MCV | Normal cells | Normocytic | Acute hemorrhage, chronic disease anemia, hemolysis (early), renal disease, hypothyroidism |
| High MCV | Large cells | Macrocytic | B12/folate deficiency, regenerative anemia (reticulocytes are large), FeLV (cats), myelodysplasia, poodles (breed-related) |
Key Vet Point: A HIGH MCV in a dog with anemia = REGENERATIVE response → bone marrow is working → GOOD sign. Low MCV in an anemic patient = chronic iron deficiency or portosystemic shunt.
5. MCH — Mean Corpuscular Hemoglobin
| Species | Normal MCH (pg) |
|---|---|
| Dog | 19.5 – 24.5 |
| Cat | 12.5 – 17.5 |
- Low MCH = cells are hypochromic (pale, less Hgb per cell) → iron deficiency
- High MCH = spherocytes or macrocytes with more Hgb content
6. MCHC — Mean Corpuscular Hemoglobin Concentration
| Species | Normal MCHC (g/dL) |
|---|---|
| Dog | 32 – 36 |
| Cat | 30 – 36 |
| Horse | 31 – 37 |
- Low MCHC (Hypochromic): Iron deficiency anemia — cells are pale, not fully packed with Hgb
- High MCHC: Intravascular hemolysis → free Hgb raises the reading artificially; lipemia or Heinz bodies can also cause this
- Normal MCHC: Most anemias (normochromic)
| MCV | MCHC | Diagnosis |
|---|---|---|
| Low | Low | Microcytic Hypochromic → Iron deficiency / chronic blood loss |
| Normal | Normal | Normocytic Normochromic → Acute hemorrhage, renal disease, chronic disease |
| High | Normal/Low | Macrocytic → Regenerative response, B12/folate deficiency |
7. RDW — Red Cell Distribution Width
- Normal: ~11–15%
- High RDW: Iron deficiency anemia, regenerative anemia (mix of large reticulocytes + small old cells), B12 deficiency
- Normal RDW with low MCV: Thalassemia-type or breed variation
- High RDW is an early indicator that anemia is developing — often changes before MCV does
8. Reticulocyte Count
This is the KEY parameter to classify anemia as Regenerative vs Non-Regenerative.
| Type | Reticulocyte Count | Meaning |
|---|---|---|
| Regenerative Anemia | High reticulocytes | Bone marrow is responding — blood loss or hemolysis |
| Non-Regenerative Anemia | Low/absent reticulocytes | Bone marrow is not responding — chronic disease, aplasia, FeLV, toxin |
Species Note: Cats release aggregate reticulocytes and punctate reticulocytes. Only aggregate reticulocytes indicate active regeneration. Dogs release polychromatic cells (visible on smear as bluish large cells).
⚪ PART B: WHITE BLOOD CELL (WBC/Leukocyte) PARAMETERS
9. Total WBC Count (Leukocyte Count)
| Species | Normal WBC (×10³/µL) |
|---|---|
| Dog | 6.0 – 17.0 |
| Cat | 5.5 – 19.5 |
| Horse | 5.5 – 12.5 |
| Cow | 4.0 – 12.0 |
| Goat | 4.0 – 13.0 |
- Infection (bacterial most common)
- Inflammation (any tissue injury — trauma, surgery, burns)
- Stress/corticosteroids (physiologic leukocytosis)
- Excitement (epinephrine release, especially dogs & cats)
- Leukemia (very high counts >100,000/µL = hyperleukocytosis → think neoplasia)
- Overwhelming bacterial sepsis (WBCs consumed faster than produced)
- Viral infections (parvovirus destroys bone marrow precursors!)
- Bone marrow depression (FeLV, drugs, toxins, radiation)
- Autoimmune disease
10. WBC DIFFERENTIAL — THE MOST IMPORTANT PART
🔵 A. NEUTROPHILS (Segmented + Bands)
- Bacterial infection — most classic cause
- Acute inflammation / tissue necrosis
- Corticosteroids / stress (no left shift in this case)
- Leukemia (neoplastic)
- Excitement (transient)
- Overwhelming bacterial sepsis (consumed in tissues)
- Viral infection (parvovirus, FeLV, FIV, canine distemper) — virus destroys bone marrow
- Bone marrow failure
- Immune-mediated neutropenia
- Drug toxicity (chemotherapy, estrogen toxicity)
MOST IMPORTANT CONCEPT — LEFT SHIFT: A left shift = presence of BAND neutrophils (immature) in circulation. When infection or severe inflammation is occurring, the bone marrow dumps immature cells (bands) into blood because it can't keep up.
- Regenerative left shift: Total WBC is high + bands present → bone marrow IS coping → bacterial infection, moderate inflammation
- Degenerative left shift: Total WBC is LOW + many bands → more bands than mature neutrophils → bone marrow is OVERWHELMED → severe sepsis, very poor prognosis
- Toxic neutrophils: Cells show toxic granulation, Döhle bodies, vacuolation → severe systemic infection/endotoxemia
| Pattern | WBC | Neutrophils | Bands | Interpretation |
|---|---|---|---|---|
| Stress leukogram | ↑ | ↑ (mature) | None/few | Corticosteroids, anxiety, pain |
| Bacterial infection | ↑↑ | ↑↑ | ↑ (left shift) | Active bacterial process |
| Viral infection | ↓ or normal | ↓ or normal | Few/none | Parvovirus, distemper, FeLV |
| Sepsis (severe) | ↓ | ↓ | ↑↑ (degenerative) | Emergency — poor prognosis |
| Leukemia | ↑↑↑ | Variable | Variable | Neoplastic |
🔴 B. LYMPHOCYTES
- Viral infections (classic! EBV, hepatitis A, CMV in humans; herpesvirus, FIV, FIP in animals)
- Chronic bacterial infections (tuberculosis, brucellosis, pertussis)
- Physiologic lymphocytosis — excitement in cats (epinephrine shifts marginated lymphocytes into circulation — counts can double!)
- Lymphocytic leukemia / lymphoma
- Immune stimulation, vaccination response
- Hypoadrenocorticism (Addison's disease — "reverse stress leukogram": lymphocytosis + eosinophilia)
- Corticosteroids (endogenous stress OR exogenous treatment) — classic! Steroids cause lymphocytes to leave blood
- Viral infections (FIV, FeLV, parvovirus)
- Immunodeficiency diseases
- Loss via lymphatics (lymphangiectasia, chylothorax)
- Radiation / chemotherapy
Key diagnostic clue: Lymphocytosis = think VIRAL. Neutrophilia = think BACTERIAL.
🟡 C. MONOCYTES
- Chronic bacterial infections (especially intracellular bacteria — Brucella, Mycobacterium)
- Chronic inflammation / tissue necrosis — monocytes clean up debris
- Fungal infections (Histoplasma, Blastomyces)
- Neoplastic disease
- Corticosteroids (part of stress leukogram)
- Recovery from bone marrow suppression
Key rule: Monocytosis = chronic or intracellular infection, or ongoing tissue destruction.
🟠 D. EOSINOPHILS
- Parasitic infections ← MOST CLASSIC CAUSE (heartworm, hookworm, roundworm, toxoplasmosis, lungworm, Giardia with eosinophilic response)
- Allergic / Hypersensitivity reactions (atopy, flea allergy dermatitis, eosinophilic granuloma complex in cats)
- Skin diseases
- Pulmonary eosinophilia (PIE syndrome in dogs)
- Mast cell tumor, lymphoma, other neoplasia
- Hypereosinophilic syndrome (cats)
- Addison's disease (adrenal insufficiency → eosinophilia is a clue)
- Acute stress (physical stress, trauma, illness)
- Corticosteroids — steroids dramatically decrease eosinophils (classic finding on stress leukogram)
- Cushing's disease (hyperadrenocorticism)
KEY DIAGNOSTIC RULE: Eosinophilia in a pet with GI signs, weight loss, coughing, or skin disease = RULE OUT PARASITES FIRST before anything else!
⚫ E. BASOPHILS
- Allergic reactions (Type I hypersensitivity)
- Heartworm disease (classic in dogs!)
- Chronic myeloid leukemia
- Mast cell tumor
- Polycythemia vera
- Hypothyroidism
Basophilia alone is rarely dramatic but basophilia + eosinophilia together strongly suggests parasitism or allergic disease.
🟣 PART C: PLATELET (THROMBOCYTE) PARAMETERS
11. Platelet Count
| Species | Normal Platelets (×10³/µL) |
|---|---|
| Dog | 175 – 500 |
| Cat | 300 – 700 |
| Horse | 100 – 350 |
| Cow | 100 – 800 |
Caveat: Cats are prone to platelet clumping in the tube → falsely low count. ALWAYS check blood smear when cat platelet count looks low.
- Iron deficiency anemia (reactive/secondary thrombocytosis)
- Inflammation / chronic infection
- Splenectomy or splenic disease
- Myeloproliferative disease (bone marrow cancer)
- Rebound after thrombocytopenia
- Immune-mediated thrombocytopenia (IMT/ITP) — most common cause in dogs (especially Cocker Spaniels, retrievers)
- Ehrlichia / Anaplasma — tick-borne diseases → classic thrombocytopenia
- Babesia — destroys platelets
- Bone marrow suppression (FeLV, leukemia, estrogen toxicity, drugs)
- Disseminated Intravascular Coagulation (DIC) — platelets consumed → thrombocytopenia + prolonged clotting times
- Increased consumption (sepsis, vasculitis)
- Decreased production (leukemia, lymphoma invading marrow)
Bleeding risk:
- Platelets < 50,000/µL → spontaneous bleeding possible
- Platelets < 20,000/µL → HIGH risk of spontaneous hemorrhage (petechiae, ecchymoses, epistaxis, melena)
12. MPV — Mean Platelet Volume
- High MPV: Young, large platelets = bone marrow is actively releasing new platelets (regenerative) → seen in IMT, active destruction
- Low MPV: Small platelets → bone marrow failure, Wiskott-Aldrich type syndromes
SECTION 3 — THE DIAGNOSTIC DECISION TREE: HOW TO READ A CBC IN < 1 MINUTE
STEP 1: Look at WBC total
↑ High? → Infection, inflammation, stress, leukemia
↓ Low? → Viral infection, severe sepsis, bone marrow failure, toxin
STEP 2: Run the Differential
Neutrophilia + Left shift? → BACTERIAL infection or severe inflammation
Lymphocytosis? → VIRAL infection, excitement (cats), lymphoma, Addison's
Eosinophilia? → PARASITES first, then allergy, then neoplasia
Monocytosis? → CHRONIC infection/inflammation, intracellular bacteria
Basophilia + Eosinophilia? → PARASITES (especially heartworm)
STEP 3: Assess RBC / PCV
PCV Low? → Anemia present
↓ Check MCV:
Microcytic? → Iron deficiency / chronic blood loss / portosystemic shunt
Normocytic? → Acute hemorrhage / chronic disease / renal disease
Macrocytic? → Regenerative response / B12 deficiency / FeLV (cats)
↓ Check Reticulocytes:
High? → Regenerative → hemorrhage or hemolysis
Low? → Non-regenerative → bone marrow problem
STEP 4: Assess Platelets
Very low (<50k)? → Tick disease (Ehrlichia/Anaplasma), IMT, DIC, FeLV
Very high? → Reactive (inflammation) or myeloproliferative
STEP 5: Put it all together!
SECTION 4 — DISEASE PATTERN RECOGNITION TABLE
| Disease | WBC | Neutrophils | Lymphocytes | Monocytes | Eosinophils | RBC/PCV | Platelets |
|---|---|---|---|---|---|---|---|
| Bacterial infection (acute) | ↑↑ | ↑↑ + Left shift | ↓ or N | N or ↑ | ↓ (stress) | N | N or ↓ |
| Viral infection (parvovirus) | ↓↓ | ↓↓ | ↓ | N | N | ↓ (bleeding) | ↓ |
| Parasitic infection (GI worms) | N or ↑ | N | N | N | ↑↑ | ↓ (if blood loss) | N |
| Heartworm | N or ↑ | N | N | N | ↑ | N | ↓ slightly |
| Stress / Corticosteroids | ↑ | ↑↑ (mature) | ↓ | ↑ | ↓ | N | N |
| Addison's Disease | N | ↓ or N | ↑ | N | ↑ | N (or mild ↓) | N |
| Cushing's Disease | ↑ | ↑↑ | ↓↓ | ↑ | ↓ | N or ↑ | N or ↑ |
| FeLV (cats) | ↓ | ↓ | ↓ | N | N | ↓↓ (non-regen anemia) | ↓ |
| Ehrlichia / Anaplasma | ↓ or N | ↓ | ↓ | ↑ | N | ↓ | ↓↓↓ |
| Babesia | N or ↑ | N | N | N | N | ↓↓ (hemolysis) | ↓ |
| DIC | ↑ | ↑↑ | ↓ | ↑ | ↓ | ↓ | ↓↓↓ |
| Lymphoma / Leukemia | ↑↑↑ | Variable | ↑↑↑ (atypical) | Variable | N | ↓ | Variable |
| IMT (ITP) | N or ↑ | N or ↑ | N | N | N | N (unless hemorrhage) | ↓↓↓ |
| Iron deficiency | N | N | N | N | N | ↓ (microcytic) | N or ↑ |
| Autoimmune hemolytic anemia (IMHA) | ↑ | ↑ | N | N | N | ↓↓ (regenerative) | N or ↓ |
SECTION 5 — BLOOD SMEAR INTERPRETATION (Always Do This!)
| Finding on Smear | Meaning |
|---|---|
| Polychromasia (blue-tinged large RBCs) | Reticulocytes → regenerative anemia |
| Anisocytosis (RBCs of varying sizes) | Regenerative anemia, iron deficiency |
| Hypochromia (pale cells with large central pallor) | Iron deficiency, chronic blood loss |
| Spherocytes (small dense RBCs, no pallor) | IMHA (immune attack clips membrane) |
| Schistocytes (fragmented RBCs) | DIC, iron deficiency, microangiopathy |
| Target cells (codocytes) | Liver disease, iron deficiency, splenectomy |
| Acanthocytes / Echinocytes | Liver disease, renal disease, splenic hemangiosarcoma |
| Heinz bodies (small Hgb precipitates) | Oxidative damage — onion/garlic toxicity, acetaminophen (CATS!), zinc toxicity |
| Howell-Jolly bodies (nuclear remnants) | Regeneration, asplenia, steroid use |
| Rouleaux (stacked coins) | Normal in horses; in dogs/cats → inflammation, myeloma, hyperglobulinemia |
| Microfilaria visible | Heartworm! |
| Morulae in neutrophils | Ehrlichia / Anaplasma infection |
| Babesia inside RBCs | Babesiosis (piroplasms) |
| Hemobartonella (Mycoplasma haemofelis) on RBCs | Cat anemia |
| Toxic neutrophils (Döhle bodies, toxic granulation, vacuolation) | Severe bacterial infection, endotoxemia, sepsis |
| Reactive lymphocytes (large, dark, irregular) | Viral stimulation, antigenic response |
| Blast cells | Leukemia — EMERGENCY |
| Large platelets (macroplatelets) | Active regeneration of platelets → IMT |
| Platelet clumps | Artifact → repeat, don't report as thrombocytopenic |
SECTION 6 — THE STRESS LEUKOGRAM (Very Important in Vet Practice)
- ↑ Neutrophils (mature, NO left shift)
- ↓ Lymphocytes
- ↓ Eosinophils
- ↑ Monocytes
This pattern is caused by cortisol → redistributes WBCs. This is NOT infection. It is a stress response. You must distinguish this from a true infection pattern. The KEY differentiator: stress leukogram has NO left shift (no band cells), while bacterial infection DOES have a left shift.
SECTION 7 — REGENERATIVE vs NON-REGENERATIVE ANEMIA
| Feature | Regenerative | Non-Regenerative |
|---|---|---|
| Cause | Blood loss (hemorrhage) OR hemolysis | Bone marrow failure, chronic disease, renal disease, FeLV |
| Reticulocytes | ↑↑ High | ↓ Low or absent |
| MCV | ↑ or normal (large young cells) | Normal or ↓ |
| Polychromasia on smear | Yes | No |
| Response | Bone marrow working | Bone marrow suppressed |
| Prognosis | Better (if cause treated) | Worse (need bone marrow stimulation or transfusion) |
| Common examples in dogs | IMHA, trauma hemorrhage, GI bleeding | FeLV (cats), Ehrlichia, aplastic anemia |
SECTION 8 — CLINICAL CBC EXAMPLES (Most Common Cases in Pet Hospital)
📋 CASE 1: Canine Parvovirus (Unvaccinated Puppy, Vomiting + Bloody Diarrhea)
| Parameter | Value | Normal (Dog) | Interpretation |
|---|---|---|---|
| WBC | 1.8 × 10³/µL | 6–17 | ↓↓ LEUKOPENIA |
| Neutrophils | 600/µL | 3,000–11,500 | ↓ NEUTROPENIA |
| Lymphocytes | 400/µL | 1,000–4,800 | ↓ LYMPHOPENIA |
| PCV | 38% | 37–55 | Normal (early) |
| Platelets | 95,000/µL | 175–500k | ↓ Thrombocytopenia |
📋 CASE 2: Pyometra (Intact Female Dog, Lethargy, PU/PD, Vaginal Discharge)
| Parameter | Value | Normal (Dog) | Interpretation |
|---|---|---|---|
| WBC | 42,000/µL | 6–17k | ↑↑↑ LEUKOCYTOSIS |
| Neutrophils | 35,000/µL (seg) | 3,000–11,500 | ↑↑↑ NEUTROPHILIA |
| Band Neutrophils | 3,500/µL | < 300 | ↑ LEFT SHIFT |
| Toxic Neutrophils | Present on smear | None | ENDOTOXEMIA |
| Monocytes | 2,500/µL | 150–1,350 | ↑ MONOCYTOSIS |
| Lymphocytes | 800/µL | 1,000–4,800 | ↓ LYMPHOPENIA |
| PCV | 31% | 37–55 | Mild anemia of chronic disease |
| Platelets | 180,000/µL | 175–500k | Low-normal |
📋 CASE 3: Feline Heartworm / Eosinophilic Condition (Cat, Chronic Cough)
| Parameter | Value | Normal (Cat) | Interpretation |
|---|---|---|---|
| WBC | 14,500/µL | 5,500–19,500 | Normal |
| Neutrophils | 7,200/µL | — | Normal |
| Eosinophils | 2,800/µL | 100–750 | ↑↑↑ EOSINOPHILIA |
| Basophils | 150/µL | 0–50 | ↑ BASOPHILIA |
| Lymphocytes | 3,000/µL | — | Normal |
| PCV | 32% | 24–45 | Normal |
📋 CASE 4: Ehrlichiosis (Dog, Tick History, Petechiae on Gums, Lethargy)
| Parameter | Value | Normal (Dog) | Interpretation |
|---|---|---|---|
| WBC | 4,200/µL | 6–17k | ↓ mild leukopenia |
| Neutrophils | 2,800/µL | 3,000–11,500 | ↓ mild neutropenia |
| Lymphocytes | 900/µL | 1,000–4,800 | Low-normal |
| Monocytes | 600/µL | 150–1,350 | ↑ monocytosis |
| PCV | 28% | 37–55 | ↓ Anemia |
| Platelets | 18,000/µL | 175–500k | ↓↓↓ CRITICAL THROMBOCYTOPENIA |
📋 CASE 5: Immune-Mediated Hemolytic Anemia — IMHA (Dog, Yellow Gums, Weakness)
| Parameter | Value | Normal (Dog) | Interpretation |
|---|---|---|---|
| WBC | 22,000/µL | 6–17k | ↑ Leukocytosis |
| Neutrophils | 18,000/µL | 3,000–11,500 | ↑ Neutrophilia |
| PCV | 12% | 37–55 | ↓↓↓ SEVERE ANEMIA |
| MCV | 82 fL | 60–77 | ↑ Macrocytic |
| Reticulocytes | 18% | <1% | ↑↑↑ REGENERATIVE |
| MCHC | 31 g/dL | 32–36 | Slightly low |
| Platelets | 95,000/µL | 175–500k | ↓ (Evans syndrome?) |
| Smear | Spherocytes +++ | None | IMHA confirmed |
📋 CASE 6: Chronic GI Parasitism (Young Dog, Weight Loss, Diarrhea, Pot-Belly)
| Parameter | Value | Normal (Dog) | Interpretation |
|---|---|---|---|
| WBC | 12,000/µL | 6–17k | High-normal |
| Eosinophils | 1,800/µL | 100–1,250 | ↑ EOSINOPHILIA |
| PCV | 26% | 37–55 | ↓ Moderate anemia |
| MCV | 55 fL | 60–77 | ↓ MICROCYTIC |
| MCHC | 28 g/dL | 32–36 | ↓ HYPOCHROMIC |
| Reticulocytes | 0.8% | <1% | Non-regenerative |
| Platelets | 620,000/µL | 175–500k | ↑ (reactive) |
SECTION 9 — QUICK REFERENCE: WHAT EACH CELL TELLS YOU
| WBC Type | ↑ Means | ↓ Means |
|---|---|---|
| Neutrophils (seg) | Bacterial infection, stress, inflammation | Viral infection, overwhelming sepsis, bone marrow failure |
| Band neutrophils | Left shift = active acute bacterial infection / endotoxemia | Normal = no left shift |
| Lymphocytes | Viral infection, excitement (cats), lymphoma, Addison's | Stress, corticosteroids, FIV/FeLV, immunodeficiency |
| Monocytes | Chronic infection, intracellular bacteria, tissue necrosis, fungal | Rarely significant |
| Eosinophils | Parasites, allergy, mast cell tumor, Addison's | Stress, corticosteroids, Cushing's |
| Basophils | Parasites (heartworm), allergy, CML | Stress, hyperthyroidism, corticosteroids |
SECTION 10 — PRACTICE QUESTIONS (Test Your Knowledge)
Answer: Pyometra with bacterial endotoxemia. Left shift (bands >300/µL) indicates bone marrow is releasing immature neutrophils due to overwhelming bacterial demand. Toxic changes confirm endotoxin exposure. Emergency ovariohysterectomy + antibiotics required.
Answer: Canine Parvoviral Enteritis. Parvovirus specifically targets rapidly dividing cells, including bone marrow neutrophil precursors → profound leukopenia and neutropenia. This is a hallmark finding. Thrombocytopenia contributes to bloody diarrhea (hemorrhagic gastroenteritis). Supportive care + isolation mandatory.
Answer: (1) Feline heartworm disease (Dirofilaria immitis — antigen + antibody test), (2) Lungworm / Aelurostrongylus abstrusus (Baermann fecal test), (3) Feline allergic bronchitis/asthma (thoracic radiograph + bronchoscopy/BAL). Eosinophilia + basophilia = parasite or allergy. Basophilia is rare in cats and should strongly prompt parasite workup.
Answer: Ehrlichia canis (Canine Monocytic Ehrlichiosis). Morulae in monocytes = pathognomonic. Severe thrombocytopenia causes hemorrhagic signs. Mild pancytopenia typical in acute/chronic phase. Treatment: Doxycycline 10 mg/kg/day PO for 28 days. Supportive care ± transfusion if PCV critical.
Answer: Immune-Mediated Hemolytic Anemia (IMHA). Spherocytes are pathognomonic — they form when macrophages partially phagocytose antibody-coated RBCs, removing part of the membrane, leaving a small dense sphere without central pallor. Concurrent thrombocytopenia = Evans Syndrome. Treatment: Prednisolone + azathioprine/mycophenolate, possible transfusion.
Answer: This is a Stress Leukogram (not infection). Key features: neutrophilia WITHOUT left shift, lymphopenia, eosinopenia, monocytosis. Caused by endogenous cortisol release due to pain/surgery/hospitalization stress. No band cells = no new infection. No treatment needed — treat the underlying cause (pain management, recovery).
QUICK DIAGNOSTIC CHEAT SHEET — BACTERIA vs VIRAL vs PARASITIC vs STRESS
| Bacterial | Viral | Parasitic | Stress/Corticosteroid | |
|---|---|---|---|---|
| WBC | ↑↑ | ↓ or normal | Normal | ↑ (mild-moderate) |
| Neutrophils | ↑↑ + left shift | ↓ | Normal | ↑↑ (NO left shift) |
| Band cells | ↑ (present) | Absent | Absent | Absent |
| Toxic changes | Often present | No | No | No |
| Lymphocytes | ↓ | ↑ or reactive | Normal | ↓↓ |
| Eosinophils | ↓ (stress response) | ↓ (stress) | ↑↑↑ | ↓↓ |
| Monocytes | ↑ (chronic) | Normal | Normal | ↑ |
| Platelets | Normal or ↓ | ↓ (parvovirus) | Normal | Normal |
| PCV/RBC | Normal (acute) or ↓ | ↓ (blood loss) | ↓ (blood loss) | Normal |
Sources: Henry's Clinical Diagnosis & Management by Laboratory Methods (Elsevier); Histology: A Text and Atlas — Pawlina/Ross (Wolters Kluwer); Textbook of Family Medicine 9e (Elsevier); Robbins & Kumar Basic Pathology (Elsevier); Medical Microbiology 9e (Elsevier). Applied to veterinary species-specific reference ranges per standard veterinary clinical hematology.
Jasa mara lya detailed authentic notes baj Raha was he detailed each and everything explained in easy way .. ma Ultrasonography in pets samja do . Jis ma har aspect cler ho k konsi age ma . English ma batayen explain as much as u can
veterinary abdominal ultrasound liver spleen kidney dog cat
ultrasound gallbladder stones acoustic shadowing
cardiac echocardiography heart ultrasound B-mode transducer
🔊 ULTRASONOGRAPHY IN VETERINARY PRACTICE
A Complete Clinical Guide for the Veterinary Professional
Sources: Goldman-Cecil Medicine 2-Vol Set | Textbook of Clinical Echocardiography | Yamada's Textbook of Gastroenterology | Sleisenger & Fordtran's GI and Liver Disease | Histology: A Text and Atlas (Pawlina/Ross) | Harrison's Principles of Internal Medicine 22e | Applied Veterinary Clinical Knowledge
SECTION 1 — WHAT IS ULTRASONOGRAPHY?
How Does It Work? (The Physics — Made Simple)
- Emits high-frequency sound waves into the body
- Receives the echoes (sound waves bounced back) from tissues
- Converts echo data into a grayscale image on screen
| Term | Meaning | Clinical Relevance |
|---|---|---|
| Frequency (MHz) | Cycles per second of sound waves | Higher frequency = better detail, less penetration; Lower frequency = less detail, more penetration |
| Wavelength | Distance between wave peaks | Shorter wavelength (higher MHz) = better resolution |
| Acoustic Impedance | Resistance of tissue to sound | Differences between tissues create echoes = creates image |
| Attenuation | Loss of sound energy as it passes through tissue | Deeper structures lose more signal — gel + correct frequency compensates |
| Reflection | Sound bouncing back from tissue interfaces | The basis of image formation |
| Refraction | Bending of sound at tissue boundaries | Causes artifacts |
| Acoustic Shadow | No signal behind dense structures (bone, stones, gas) | Classic sign of gallstones, calcifications, mineralized lesions |
| Acoustic Enhancement | Brighter signal behind fluid-filled structures | Classic sign of cysts, bladder, fluid-filled gallbladder |
Frequency Selection — The Most Important Machine Setting
HIGH FREQUENCY (7.5 – 15 MHz)
→ Excellent resolution, POOR penetration
→ Use for: Small animals (cats, small dogs, rabbits)
Superficial structures (lymph nodes, skin, eyes, testicles)
Guided biopsy needles (you can see the needle clearly)
MEDIUM FREQUENCY (5 – 7.5 MHz)
→ Good balance of resolution and penetration
→ Use for: Medium-sized dogs (abdominal organs)
Most routine small animal work
LOW FREQUENCY (2 – 5 MHz)
→ Poor resolution, EXCELLENT penetration
→ Use for: Large animals (horses, cattle, large-breed dogs)
Deep abdominal structures
Cardiac imaging (echocardiography)
Simple Rule: Small animal, shallow structure = HIGH frequency. Large animal, deep structure = LOW frequency.
SECTION 2 — ULTRASOUND TERMINOLOGY (THE ECHO SCALE)
| Term | Appearance on Screen | What It Means | Examples |
|---|---|---|---|
| Hyperechoic | Bright/White | Reflects lots of sound back | Bone, fat, fibrous tissue, gallstones, calcifications, air interface |
| Isoechoic | Same brightness as reference | Same density as comparison tissue | Normal lymph node vs. surrounding fat |
| Hypoechoic | Dark gray | Reflects less sound, absorbs more | Muscle, inflammation, many tumors, edematous tissue |
| Anechoic | Completely Black | No echoes at all = fluid | Urine, bile, pure cysts, blood (fresh), transudates |
| Heterogeneous | Mixed brightness | Non-uniform internal texture | Neoplasia, hematoma, abscess, complex masses |
| Homogeneous | Uniform texture throughout | Normal organ parenchyma | Normal liver, normal spleen |
The Most Important Echogenicity Rule:
- Black (Anechoic) = FLUID
- White (Hyperechoic) = DENSE STRUCTURE (stone, bone, fat, calcification)
- Gray (Hypoechoic) = SOFT TISSUE
- Dirty/Speckled (Heterogeneous) = PATHOLOGY
SECTION 3 — ULTRASOUND MODES (What the Machine Can Do)
| Mode | Name | What It Shows | Vet Use |
|---|---|---|---|
| B-Mode | Brightness Mode / 2D Mode | Real-time 2D cross-sectional image — THE main mode | Abdominal, reproductive, soft tissue scanning |
| M-Mode | Motion Mode | Time vs. depth — shows movement of structures over time | Measuring heart wall motion, valve movement |
| Color Doppler | — | Blood flow direction (Red = toward probe, Blue = away) | Cardiac valves, vessels, detecting blood flow in masses |
| Pulsed Wave (PW) Doppler | — | Blood flow velocity at a specific point | Cardiac valve stenosis, regurgitation |
| Continuous Wave (CW) Doppler | — | High-velocity blood flow along entire beam | Severe stenosis or regurgitation |
| Power Doppler | — | Detects very low-flow blood vessels (no direction info) | Organ vascularity, tumor blood supply |
| 3D/4D Ultrasound | — | Three-dimensional real-time image | Fetal imaging, advanced cardiac |
For daily vet hospital use: B-Mode is what you'll use 90% of the time. Doppler modes are used for cardiac work.
SECTION 4 — TRANSDUCER (PROBE) TYPES
| Transducer | Shape | Frequency | Use |
|---|---|---|---|
| Linear Array | Rectangular flat head | 7.5–15 MHz | Superficial structures: lymph nodes, skin masses, tendons, eyes, small-breed abdominal work, biopsy guidance |
| Curvilinear (Convex) Array | Curved head | 2–8 MHz | Abdominal organs in medium-large dogs; Large animals |
| Phased Array (Sector) | Small footprint, fan-shaped beam | 2–5 MHz | Cardiac (echocardiography) — fits between ribs |
| Microconvex | Small curved head | 5–8 MHz | Cats, small dogs, neonates |
| Endoscopic/Intraluminal | Long probe with transducer at tip | — | EUS (endoscopic ultrasound) — GI wall, pancreas |
SECTION 5 — PATIENT PREPARATION FOR ULTRASOUND
Clipping the Hair (Mandatory for Good Images)
- Abdominal scan: Clip from xiphoid to pubis, both flanks
- Cardiac scan: Clip both right and left parasternal windows (where ribs meet sternum), subxiphoid area
- Neck (thyroid, lymph nodes): Clip ventral cervical region
- Bladder / reproductive: Clip inguinal and caudal abdominal area
Coupling Gel
Fasting (for Abdominal Ultrasound)
- Ideal: Fast 6–12 hours before scanning (dogs), 4–6 hours (cats)
- Reason: Food and gas in GI tract causes acoustic shadowing that obscures deeper organs (especially pancreas, mesenteric lymph nodes)
- Emergency scans are done without fasting — just accept degraded image quality
Sedation / Restraint
- Most cats and calm dogs: Manual restraint only
- Anxious, aggressive, or painful patients: Mild sedation (butorphanol, dexmedetomidine)
- Heavy sedation (propofol/alfaxalone): For Doppler cardiac work requiring motionless patient
- NEVER use general anesthesia for routine abdominal USG unless necessary
Patient Positioning
- Dorsal recumbency (lying on back): Best for abdominal scanning — organs fall away from spine, bladder is easily visualized, gravity helps orient organs
- Left lateral recumbency: Liver, right kidney (scan from right side)
- Right lateral recumbency: Spleen, left kidney
- Standing: Large animals (horses, cattle) — scan from flank
- Sternal: Cardiac work in cats (some prefer this)
SECTION 6 — UNDERSTANDING THE ULTRASOUND SCREEN
- Top of image = closest to probe (skin surface)
- Bottom of image = deepest structures
- Left side = depends on probe orientation marker (usually cranial or medial)
- Depth marker on the side = distance in centimeters from probe surface
- Gain = overall brightness of image (increase if too dark, decrease if too bright)
- Focus depth = the point where beam is narrowest = clearest image (set this at the organ of interest)
- Freeze button = captures image for measurement and documentation
SECTION 7 — ARTIFACTS (What Fools You on Ultrasound)
| Artifact | Appearance | Cause | Example |
|---|---|---|---|
| Acoustic Shadow | Dark shadow behind a structure | Dense object blocks sound (stone, bone, gas) | Gallstones, bladder stones, calcified lymph nodes, ribs |
| Posterior Acoustic Enhancement | Bright area behind a structure | Fluid transmits sound better → enhances deeper tissue | Cysts, full bladder, gallbladder (no stones) |
| Reverberation | Parallel bright lines repeating | Sound bouncing back and forth between two reflective surfaces | Needle artifacts, air in gut, trapped air |
| Comet Tail Artifact | Bright tapering echoes like a comet tail | Special reverberation from small metallic objects | Surgical clips, microchip, gas in lung |
| Ring-Down Artifact | Continuous bright streak | Gas bubbles in fluid | Gas in bowel, pneumoperitoneum |
| Mirror Image | Organ appears duplicated on other side of reflective surface | Strong reflector (diaphragm) creates mirror image | Liver "appearing" in thorax — NOT a real thoracic mass |
| Refraction shadowing | Edge shadow at sides of curved structures | Sound bends at curved surfaces | Edges of kidney, cyst walls |
| Beam Width Artifact | Echoes in fluid-filled structure | Wide beam includes nearby structures | False "stones" in bladder near bone |
| Dirty Shadow | Incomplete shadow with internal echoes | Gas (not stone) blocking sound | Gas-filled bowel shadows — different from clean stone shadows |
Clean shadow = Stone/Mineral. Dirty shadow = Gas.
SECTION 8 — ORGAN-BY-ORGAN ULTRASONOGRAPHY
🟤 A. LIVER
Normal Liver Ultrasound Appearance:
- Echogenicity: Moderately hyperechoic (slightly brighter than renal cortex, slightly less bright than spleen in dogs; In cats: liver ≈ spleen echogenicity)
- Texture: Homogeneous (uniform, fine granular pattern)
- Margins: Smooth, sharp edges
- Portal veins: Visible as anechoic tubular structures with hyperechoic (bright) walls — wall is bright because it's connective tissue
- Hepatic veins: Anechoic tubular structures WITHOUT bright walls — no connective tissue sheath
- Bile ducts: Should be barely visible (if visible = dilated = pathological)
- Size: Should fit within costal arch (not extend beyond last rib in dog)
Liver Pathology — What to Look For:
| Finding | Appearance | Likely Diagnosis |
|---|---|---|
| Diffusely hyperechoic liver | Brighter than normal, "sparkly" | Hepatic lipidosis (fatty liver) — VERY common in cats on anorexia! |
| Diffusely hypoechoic liver | Darker than normal | Passive congestion (right heart failure), hepatitis, lymphoma infiltration |
| Heterogeneous texture | Mixed bright and dark areas | Cirrhosis, nodular hyperplasia, neoplasia, chronic hepatitis |
| Rounded liver edges | Blunt, rounded margins instead of sharp | Hepatomegaly — congestion, infiltration, neoplasia |
| Small irregular liver | Shrunken, irregular surface | Cirrhosis, hepatic fibrosis, portosystemic shunt (young dogs!) |
| Focal hypoechoic mass | Dark round lesion | Abscess, hematoma, hepatocellular carcinoma, metastasis |
| Focal hyperechoic mass | Bright round lesion | Lipoma, mineralization, old hematoma, some neoplasias |
| Cystic lesion | Anechoic with posterior enhancement + smooth walls | Benign hepatic cyst (common in older patients) |
| Dilated bile ducts | Tortuous anechoic tubular structures near portal triads | Biliary obstruction, cholangiohepatitis |
| Hyperechoic portal vessel walls (exaggerated) | Very prominent bright ring around portal vessels | Hepatitis, early cirrhosis |
| Ascites (fluid around liver) | Anechoic fluid outlining liver lobes | Hypoproteinemia, right heart failure, peritonitis, neoplasia |
Most Important Rule: Compare liver echogenicity to the right renal cortex (kidney cortex). In a normal dog, liver should be slightly brighter than kidney cortex. If liver is much brighter → fatty liver (lipidosis). If liver is darker → congestion or lymphoma.
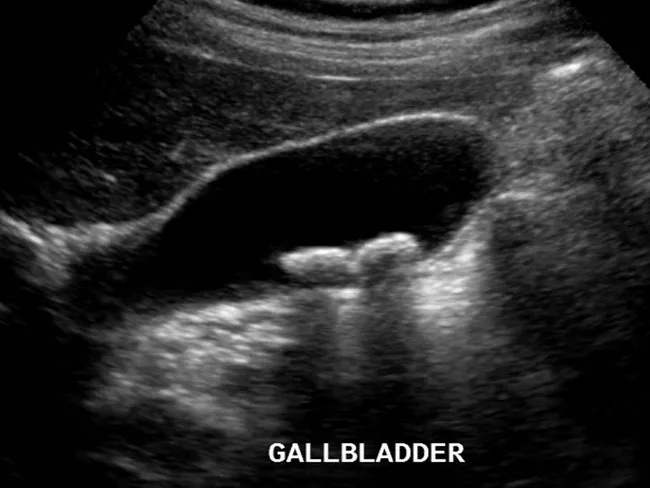
🫁 B. GALLBLADDER & BILE DUCTS
- Anechoic (black) interior — filled with bile (pure fluid)
- Thin, smooth walls (< 3 mm in dogs, < 1 mm in cats)
- Posterior acoustic enhancement behind it (fluid enhances)
- Small amount of bile sludge (echogenic material that moves when patient position changes) can be normal, especially in fasted animals
Gallbladder Pathology:
| Finding | Appearance | Diagnosis |
|---|---|---|
| Cholelithiasis (gallstones) | Hyperechoic (bright) mobile foci with CLEAN posterior acoustic shadow | Cholelithiasis — classic "clean shadow" distinguishes stones from polyps |
| Biliary sludge | Echogenic material in dependent portion, no shadow, moves with gravity | Bile sludge — often normal; excessive = biliary mucocele or inflammation |
| Gallbladder mucocele | Immobile, "kiwi fruit" or stellate pattern of echogenic bile that doesn't move | Biliary mucocele — common in Shelties, Cocker Spaniels. Surgical emergency! |
| Cholecystitis | Thick gallbladder wall (>3 mm dogs, >1 mm cats) + pericholecystic fluid + pain on probe pressure | Cholecystitis — check for gallstones as underlying cause |
| Dilated common bile duct | CBD > 3 mm (dogs), > 4 mm (cats) | Biliary obstruction — pancreatitis, cholelith, neoplasia, biliary stricture |
| Gallbladder polyps | Echogenic wall projections, NO SHADOW, do not move | Cholesterol polyps, adenomatous polyps |
🫘 C. KIDNEYS (RENAL ULTRASONOGRAPHY)
Normal Kidney Appearance:
- Shape: Bean-shaped; smooth capsular margin
- Cortex: Outer layer — hypoechoic (darker gray), homogeneous
- Medulla (Renal Pyramids): Inner layer — even more hypoechoic (darker than cortex) — triangular/wedge shapes visible in cross section
- Pelvis: Central hyperechoic (bright) line = renal sinus fat + collecting system = "renal crest"
- Corticomedullary differentiation (CMD): Healthy kidneys show a clear difference between cortex and medulla. Loss of CMD = renal disease.
Normal Kidney Size (Approximate):
| Species | Kidney Length |
|---|---|
| Dog | 5.5 – 8.5 cm (left slightly larger) |
| Cat | 3.0 – 4.5 cm |
| Horse | 15 – 18 cm |
| Rabbit | 2.5 – 4.0 cm |
Kidney Pathology:
| Finding | Appearance | Diagnosis |
|---|---|---|
| Enlarged kidneys | Larger than species normal, may be hyperechoic or hypoechoic | Acute renal failure, renal lymphoma (cats!), polycystic kidney disease, pyelonephritis |
| Small kidneys | Smaller than normal, irregular surface | Chronic kidney disease (CKD), renal fibrosis, end-stage kidneys |
| Hyperechoic cortex | Cortex brighter than liver | Acute nephritis, CKD, glomerulonephritis, leptospirosis, nephrotic syndrome |
| Loss of CMD | Cortex and medulla look the same shade | Severe renal disease, CKD, lymphoma infiltration |
| Hydronephrosis | Anechoic (black) dilation of renal pelvis — "black hole" in center of kidney | Ureteral obstruction (stones, stricture, mass) → back-pressure dilates pelvis |
| Renal cysts | Round anechoic structures with posterior enhancement + smooth walls | Benign cysts (common in older cats), PKD (Persian cats — genetic!) |
| Renal calculi (nephrolithiasis) | Hyperechoic foci with acoustic shadow in renal pelvis | Kidney stones |
| Pyelonephritis | Dilated pelvis + echogenic material inside + enlarged kidney | Ascending bacterial infection — often E. coli in dogs |
| Renal mass | Focal heterogeneous disruption of architecture | Renal carcinoma, transitional cell carcinoma, lymphoma |
| Perirenal fluid | Anechoic fluid around kidney capsule | Urinary leakage, subcapsular hematoma, lymphoma |
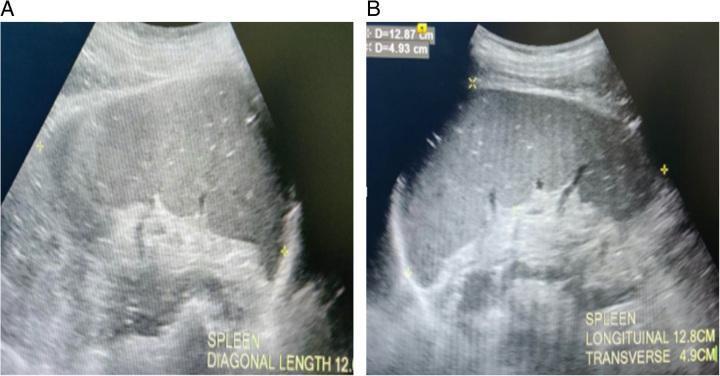
🫀 D. SPLEEN
- Echogenicity: Most hyperechoic (brightest) of all parenchymal organs — this is your reference! Spleen is brightest → then liver → then renal cortex (most hypoechoic of the three)
- Texture: Extremely homogeneous, fine-grained "sandy" appearance
- Margins: Smooth, sharp, well-defined capsule
- Location: Left cranial abdomen, just caudal to stomach
Reference rule for echogenicity: Spleen > Liver > Kidney cortex in brightness (dogs and cats)
Splenic Pathology:
| Finding | Appearance | Diagnosis |
|---|---|---|
| Splenomegaly | Enlarged spleen, may extend far caudally | Hepatitis, portal hypertension, immune-mediated disease, leukemia, lymphoma, splenic congestion, sedation (especially acepromazine in dogs!) |
| Diffuse hypoechoic spleen | Darker than normal | Lymphoma infiltration (especially cats), lymphosarcoma, acute inflammation |
| Focal hypoechoic masses | Dark round lesions in spleen | Splenic hematoma, abscess, nodular hyperplasia |
| "Target lesion" | Dark center + bright rim | Mast cell tumor, lymphoma |
| Splenic torsion | Markedly enlarged, hypoechoic, non-vascular on Doppler | Splenic torsion (emergent surgery!) — loss of flow on color Doppler |
| Hemangiosarcoma | Large heterogeneous mass, often with cavitations (dark pockets) | Splenic hemangiosarcoma — GSDs, Golden Retrievers at high risk. Very common! |
| Extramedullary hematopoiesis | Multiple small nodules throughout parenchyma | Reactive nodular change — common in old dogs, often benign |
The "Meatball" Appearance: Large, round, mixed-echogenicity nodules in the spleen of a middle-aged to old German Shepherd or Golden Retriever = think Splenic Hemangiosarcoma until proven otherwise. This is an oncological emergency.
Important: In dogs given acepromazine sedation, the spleen dramatically enlarges. This is a pharmacologic effect, not disease.
🫁 E. URINARY BLADDER
- Anechoic interior (urine = pure fluid = black)
- Thin, smooth wall (2–4 mm when full)
- Posterior acoustic enhancement behind bladder
- Triangular or oval shape depending on fullness
Bladder Pathology:
| Finding | Appearance | Diagnosis |
|---|---|---|
| Urolithiasis (bladder stones) | Hyperechoic foci with clean acoustic shadow, move when patient repositioned (gravity-dependent) | Struvite, oxalate, urate stones — classic acoustic shadow |
| Cystitis | Thickened bladder wall, irregular inner surface, possible sediment in lumen | Bacterial cystitis, sterile cystitis, FIC (Feline Idiopathic Cystitis) |
| Bladder mass / TCC | Irregular thickened focal wall projection, often at trigone | Transitional cell carcinoma (TCC) — most common bladder tumor in dogs; NSAID therapy |
| Bladder sludge / crystalluria | Fine echogenic material settling at bottom (no shadow) | Crystalluria, inflammatory debris |
| Blood clots | Mobile echogenic material, irregular shape, no shadow | Hematuria — moves but doesn't shadow |
| Intraluminal mass | Non-mobile echogenic mass attached to wall | TCC, polyp, mucosal mass |
| Bladder wall edema | Thickened wall, anechoic (dark) layer within wall layers | Cystitis, edema from adjacent inflammation |
| Ureteral jets | Flash of color on Doppler at ureteral openings | Normal urine entering bladder — absent jets = ureteral obstruction |
TCC (Transitional Cell Carcinoma) Tip: In dogs, the most common location is the trigone (where ureters enter bladder). Biopsy via cytocentesis is contraindicated (risk of seeding). Use urine cytology or traumatic catheter lavage instead.
🫁 F. PANCREAS
- Sits retroperitoneally between stomach and duodenum
- Gas-filled duodenum frequently obscures the right limb
- Very similar echogenicity to surrounding mesenteric fat
Pancreatic Pathology:
| Finding | Appearance | Diagnosis |
|---|---|---|
| Pancreatitis | Enlarged, hypoechoic pancreas + hyperechoic (bright) surrounding mesenteric fat (peripancreatic fat saponification) + free abdominal fluid nearby | Acute/chronic pancreatitis — dogs (high fat diet, Miniature Schnauzers) and cats |
| Pancreatic mass | Focal hypoechoic region disrupting normal architecture | Pancreatic carcinoma, pancreatic insulinoma (insulin-secreting tumor) |
| Pancreatic cysts/pseudocysts | Round anechoic fluid-filled pockets adjacent to or within pancreas | Post-pancreatitis pseudocysts, pancreatic abscesses |
| Pancreatic duct dilation | Visible anechoic tubular structure within pancreatic parenchyma | Pancreatic duct obstruction, chronic pancreatitis |
Clinical note for cats: Triaditis — simultaneous pancreatitis + cholangitis + IBD is common in cats. USG showing thickened small intestine + abnormal pancreas + dilated bile duct in a cat = triaditis until proven otherwise.
🐕 G. GASTROINTESTINAL TRACT
From outside → inside:
1. Serosa → Hyperechoic (bright)
2. Muscularis → Hypoechoic (dark)
3. Submucosa → Hyperechoic (bright) ← Thickest bright layer
4. Mucosa → Hypoechoic (dark)
5. Mucosal surface → Hyperechoic (bright)
- Stomach: 3–5 mm
- Small intestine (dog): 2–5 mm
- Small intestine (cat): 2–4 mm (duodenum up to 5 mm)
- Large intestine: 2–4 mm
GI Pathology:
| Finding | Diagnosis |
|---|---|
| Focal thickening with loss of wall layers | Neoplasia (lymphoma, adenocarcinoma, leiomyosarcoma) |
| Diffuse wall thickening, all layers preserved | IBD (Inflammatory Bowel Disease), enteritis |
| Diffuse thickening, mucosal layer most prominent | Alimentary lymphoma (especially cats) |
| Corrugated (wavy) small intestine | Linear foreign body (string — "plicating bowel" pattern) |
| Gas-filled loops, no motility | Ileus (functional or mechanical) |
| Hyperechoic mass with shadow inside lumen | Foreign body with acoustic shadow |
| Free peritoneal fluid adjacent | Perforation, peritonitis |
🐾 H. ADRENAL GLANDS
- Right adrenal: Craniomedial to right kidney, between caudal vena cava and kidney
- Left adrenal: Craniomedial to left kidney, medial to aorta
- Small, peanut/comma-shaped, hypoechoic structures
- Dog: Length < 3 cm, width < 7.4 mm
- Cat: Smaller, 3–6 mm width
- Hyperechoic cortex with hypoechoic medulla — in ideal images
Adrenal Pathology:
| Finding | Diagnosis |
|---|---|
| Bilateral symmetric enlargement | Pituitary-dependent hyperadrenocorticism (PDH) — most common Cushing's cause |
| Unilateral large mass | Adrenal-dependent hyperadrenocorticism (AH) — adrenal tumor. The other gland is often atrophied (small) |
| Hypoechoic, bilaterally small adrenals | Hypoadrenocorticism (Addison's disease) |
| Mineralization (hyperechoic foci with shadow) | Old adrenal lesion, adrenal cyst, old hematoma |
| Vascular invasion (into caudal vena cava) | Adrenal carcinoma with venous thrombus — poor prognosis |
Normal adrenal width > 7.4 mm in dogs = adrenomegaly. Measure at the widest point.
💗 I. ECHOCARDIOGRAPHY (CARDIAC ULTRASOUND)
- Heart is surrounded by ribs and lungs → acoustic windows are limited
- Patient must be still — cardiac motion is rapid
- Acoustic windows: Right parasternal, left parasternal, subcostal, apical
- 2D B-Mode: Anatomy, chamber size, wall thickness, valves
- M-Mode: Precisely measures wall thickness and chamber dimensions over time
- Color Doppler: Valve regurgitation (backflow) and stenosis (narrow flow)
- Pulsed Wave Doppler: Measures blood flow velocities (mitral E/A wave, aortic outflow)
- Continuous Wave Doppler: Measures high-velocity flows through stenotic valves
Standard Views in Veterinary Echocardiography:
| View | What You See |
|---|---|
| Right Parasternal Long Axis | Left ventricle, mitral valve, aorta, left atrium in one view |
| Right Parasternal Short Axis (at papillary level) | Cross-section of LV — "donut" shape of LV — measure wall thickness here |
| Right Parasternal Short Axis (at heart base) | Aorta, pulmonary artery, tricuspid valve |
| Left Apical 4-Chamber | All 4 chambers simultaneously — assess atrial size, mitral/tricuspid valves |
| Subcostal View | Diaphragm, pericardial space, inferior vena cava |
Key Measurements (M-Mode, Right Parasternal Short Axis):
| Measurement | Abbreviation | What It Measures |
|---|---|---|
| Left Ventricular Internal Diameter in Diastole | LVIDd | Size of LV when relaxed (enlarged = DCM) |
| Left Ventricular Internal Diameter in Systole | LVIDs | Size of LV when contracted (enlarged = poor function) |
| Interventricular Septum Thickness | IVSd/IVSs | Wall thickness (increased = HCM) |
| Left Ventricular Free Wall Thickness | LVFWd/LVFWs | Wall thickness (increased = HCM) |
| Fractional Shortening | FS = (LVIDd - LVIDs) / LVIDd × 100 | Measure of systolic function (normal: 25–45%) |
| Ejection Fraction | EF | Overall pump function (normal: > 50%) |
| Left Atrium : Aorta Ratio | LA:Ao | Left atrial enlargement (normal < 1.5:1 in dogs, < 1.6:1 in cats) |
Common Cardiac Diseases on Echo:
| Disease | Species | Echo Findings |
|---|---|---|
| Dilated Cardiomyopathy (DCM) | Dogs (Dobermans, Great Danes, Irish Wolfhounds) | LVIDd ↑, thin walls, FS ↓ (<25%), both chambers dilated |
| Hypertrophic Cardiomyopathy (HCM) | Cats (Maine Coon, Ragdoll — genetic) | LV wall thickness ↑ (> 6 mm), small LV cavity, LA:Ao often ↑ |
| Mitral Valve Disease (MVD/MMVD) | Dogs (Cavalier KCSs, small breeds) | Mitral valve thickened/irregular + Doppler shows mitral regurgitation |
| Pericardial Effusion | Dogs (especially Goldens — hemangiosarcoma) | Anechoic fluid surrounding heart ("floating heart"), cardiac tamponade |
| Aortic Stenosis | Dogs (Rottweilers, Boxers, German Shepherds) | Sub-aortic narrowing + high velocity aortic outflow on CW Doppler |
| Pulmonic Stenosis | Dogs (Bulldogs, Mastiffs, Beagles) | Post-stenotic pulmonary artery dilation + high velocity pulmonary flow |
| Patent Ductus Arteriosus (PDA) | Dogs (Poodles, Shelties, German Shepherds) | Continuous turbulent flow on color Doppler in main pulmonary artery |
| Ventricular Septal Defect (VSD) | Dogs, cats | Defect in septum + left-to-right shunting on color Doppler |
🐾 J. REPRODUCTIVE ULTRASONOGRAPHY
Female — Uterus and Ovaries
| Finding | Appearance | Diagnosis |
|---|---|---|
| Pyometra | Severely enlarged fluid-filled uterine horns (anechoic/echogenic fluid) | Pyometra — emergency surgery or medical management |
| Mucometra / Hydrometra | Anechoic fluid-distended uterus, thin wall, no pus | Accumulation of mucus/fluid — benign but can be large |
| Pregnancy | Gestational sacs (anechoic fluid spheres) with fetal structures visible | Pregnancy — first visible at ~21–25 days post-conception in dogs |
| Fetal viability | Fetal heart movement visible by Day 24–28 in dogs | Live vs. dead fetuses — no heartbeat = fetal death |
| Ovarian cyst | Anechoic round structure at ovary | Follicular cyst, luteal cyst |
| Ovarian mass | Complex heterogeneous mass | Granulosa cell tumor, teratoma, adenocarcinoma |
| Gestational Age | USG Finding |
|---|---|
| Day 20–23 | Gestational sacs visible (anechoic spheres) |
| Day 24–28 | Embryo visible + heartbeat detectable |
| Day 28–35 | Fetal head, body, heart chambers |
| Day 35–45 | Fetal movement, organ development |
| Day 45–63 | Full skeletal detail, count ribs and limbs |
Male — Testes and Prostate
| Finding | Diagnosis |
|---|---|
| Hypoechoic area within testis | Testicular abscess, tumor (Sertoli cell tumor, interstitial tumor) |
| Testicular atrophy (small, hypoechoic) | Sertoli cell tumor in contralateral testis (hormone-producing) |
| Undescended testis (cryptorchidism) | Scan inguinal canal and pre-scrotal region for small hypoechoic oval |
| Prostatic enlargement — symmetrical | Benign Prostatic Hyperplasia (BPH) — intact old dogs |
| Prostatic cysts | Anechoic cysts within prostate |
| Prostatic heterogeneous texture + mineralization | Prostatic carcinoma or prostatic abscess |
👁️ K. OCULAR ULTRASONOGRAPHY
| Finding | Diagnosis |
|---|---|
| Bright linear structure within vitreous | Retinal detachment (complete = "V" or "T" shape = pathognomonic) |
| Hyperechoic mass within eye | Uveal melanoma, ciliary body adenoma/carcinoma |
| Hyperechoic lens with shadowing | Lens luxation/subluxation with mineralization |
| Fluid behind eye | Retrobulbar abscess, orbital mass |
🦷 L. LYMPH NODE ULTRASONOGRAPHY
- Oval or elongated
- Hypoechoic cortex, hyperechoic hilum (central bright line = fat + vessels)
- Long:Short axis ratio > 2:1 (elongated = normal)
| Finding | Diagnosis |
|---|---|
| Rounded (L:S ratio < 2:1), hypoechoic, loss of hilum | Lymphoma, metastatic carcinoma |
| Enlarged but maintains normal architecture | Reactive hyperplasia (infection, vaccination) |
| Hyperechoic lymph node | Mineralization, old infection, fungal (Histoplasma) |
| Anechoic center with irregular wall | Lymph node abscess |
- Submandibular: Caudal to mandible, medial side
- Prescapular: Cranial to shoulder
- Axillary: Medial axilla
- Inguinal: Inguinal canal
- Popliteal: Caudal stifle
- Mesenteric/Sublumbar: Deep abdominal (requires high penetration)
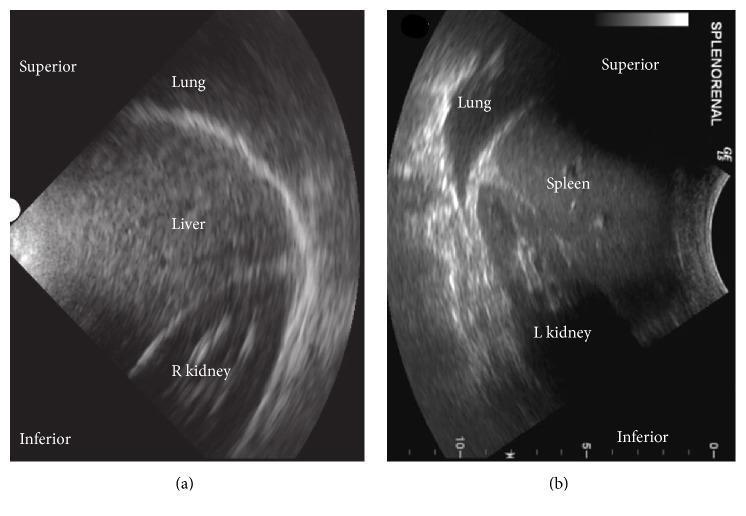
SECTION 9 — ABDOMINAL FLUID (FREE FLUID / EFFUSION)
- Between the liver and right kidney (hepatorenal recess)
- Between the spleen and left kidney (splenorenal recess)
- Around the bladder
- Between intestinal loops
- In the falciform ligament area
| Fluid Type on USG | Appearance | Likely Diagnosis |
|---|---|---|
| Pure anechoic fluid | Completely black, no echoes | Transudate — hypoproteinemia, heart failure, cirrhosis |
| Slightly echogenic fluid | Mildly gray, few swirling echoes | Modified transudate — early FIP, liver disease, protein-rich fluid |
| Echogenic/complex fluid | Gray with strands, fibrin, debris | Exudate — bacterial peritonitis, uroabdomen, bile peritonitis, FIP (infectious peritonitis) |
| Fluid with hyperechoic particles | Bright dots floating in fluid | Hemoabdomen (blood), FIP, chylous effusion |
FAST Exam (Focused Assessment with Sonography for Trauma): A rapid 4-quadrant scan to detect free fluid in emergencies:
- DH (Diaphragmaticohepatic) — right side, liver + right kidney
- SS (Splenorenal) — left side, spleen + left kidney
- UR (Urinary Bladder) — caudal midline
- HG (Hepatogastric) — cranial midline
Any anechoic fluid in these windows in a trauma patient = emergency abdominal exploration.
SECTION 10 — ULTRASOUND-GUIDED PROCEDURES
Fine Needle Aspirate (FNA) / Core Biopsy:
- Use high-frequency linear probe
- Visualize needle tip entering the lesion in real time
- Freehand technique: Probe in one hand, needle in other hand
- Needle guide: Bracket attachment on probe for guided biopsy
- Avoid: Vessels (use color Doppler to check before needle entry), major ducts, gas-filled bowel
What Can Be Aspirated / Biopsied Under USG:
- Liver (diffuse disease FNA, focal mass)
- Spleen (lymphoma, mast cell tumor)
- Kidney (cortex biopsy for CKD classification)
- Lymph nodes (reactive vs. neoplastic)
- Masses anywhere
- Cysts (drainage)
- Joint fluid (guided arthrocentesis)
- Thoracic fluid (guided thoracocentesis)
- Abdominal fluid (guided abdominocentesis/paracentesis)
Cystocentesis (Bladder Urine Sampling):
- Visualize full bladder
- Insert needle directly through ventral abdominal wall into bladder center
- Aspirate 1–5 mL urine into sterile syringe
- Avoids contamination — gold standard for urine culture
SECTION 11 — AGE-RELATED ULTRASONOGRAPHIC FINDINGS
| Age Group | Species | Common/Expected USG Findings | Clinical Significance |
|---|---|---|---|
| Neonates (0–4 weeks) | All | Organs are hypervascular, relatively hyperechoic compared to adults. Less CMD in kidneys. | Normal for age — do not over-interpret |
| Pediatric (4 weeks – 1 year) | Dogs | Liver relatively hyperechoic. Spleen proportionally large. Thymus visible in cranial mediastinum. | Thymus is NORMAL — not a mass! |
| Pediatric (< 6 months) | Cats | Liver relatively hyperechoic, not always lipidosis | Physiologic — confirm with clinical context |
| Young adult (1–3 years) | Dogs | Begin screening large breeds for cardiac disease (Doberman → Holter/Echo yearly) | Early DCM screening |
| Young adult (1–2 years) | Cats | Screen Maine Coons, Ragdolls for HCM (genetic mutation testing + echo) | HCM can present early in these breeds |
| Middle-aged (5–8 years) | Dogs | Splenic nodules common — often benign nodular hyperplasia | Do not automatically assume cancer; aspirate |
| Middle-aged (6+ years) | Intact female dogs | Pyometra risk high after diestrus. Cystic endometrial hyperplasia on USG | Pre-surgical screening for breeding females |
| Senior (8+ years) | Dogs | Adrenal enlargement (Cushing's), nodular liver, prostatic changes, splenic masses more common | Routine senior wellness screen with USG |
| Senior (10+ years) | Cats | Renal CKD (small irregular kidneys), hepatic lipidosis (anorexia), hyperthyroidism (thyroid nodules), HCM | Annual USG + T4 level recommended |
| Any age | Persian/Exotic cats | PKD — bilateral renal cysts | Screen at 10 months — autosomal dominant disease |
| Any age | Cavalier KCS | MMVD — cardiac USG from age 1 year (Cavalier Health Protocol) | Pre-breeding cardiac screening required |
| Any age | Golden Retriever | Splenic + cardiac hemangiosarcoma risk | Any acute collapse → immediate FAST scan |
| Any age | Doberman Pinscher | DCM — annual echocardiography from age 4 years | Pre-clinical DCM is detectable before symptoms |
SECTION 12 — ARTIFACTS AND MISTAKES TO AVOID
| Mistake | What Happens | How to Avoid |
|---|---|---|
| Not clipping properly | Hair traps air → no image | Always clip thoroughly, even thin fur |
| Not enough gel | Air between probe and skin → artifact shadows | Use generous gel, re-apply during scan |
| Wrong frequency | Deep organs not seen, or superficial organs over-processed | Match frequency to depth and patient size |
| Mirror artifact from diaphragm | Liver "appears" in thorax | Recognize the strong diaphragm reflection — it's an artifact |
| Mistaking bowel gas for stones | Dirty acoustic shadow from gas-filled bowel | Dirty shadow (gas) vs. clean shadow (stone) — reposition patient |
| Platelet clumping artifacts (cat bladder) | Apparent bladder wall thickening | Reposition cat, rescan — true wall thickening doesn't change with position |
| Sedation splenomegaly | Spleen enlarged from acepromazine | Note if patient was sedated — this is NOT disease |
| Near-field artifact | Structures close to probe look blurred | Increase standoff distance or use a standoff pad |
SECTION 13 — DOCUMENTATION AND REPORTING
- Patient info: Name, species, breed, age, sex, weight, date
- Clinical indication: Why was USG done?
- Machine settings: MHz used, mode (B/M/Doppler)
- Patient prep: Fasted or not? Sedated? Clipped?
- Organ-by-organ systematic findings: Even if normal — document "normal" for each organ
- Measurements: Size of organs, masses, lymph nodes, wall thickness
- Images captured: Save representative images for each organ
- Interpretation: Summary of findings
- Recommendations: Further tests, guided procedures, follow-up
SECTION 14 — PRACTICE QUESTIONS
Answer: Severely distended uterine horns bilaterally, filled with anechoic to mildly echogenic fluid (pus). The horns are visible as large tortuous fluid-filled tubular structures caudal to the kidneys and around/caudal to the bladder. Wall may be thickened. Free abdominal fluid may be present if uterus has ruptured. Diagnosis: Open-cervix pyometra. Emergency ovariohysterectomy required.
Answer: Hepatic Lipidosis (Fatty Liver Syndrome). The extreme hyperechogenicity is due to fat accumulation in hepatocytes. This is an emergency in cats — prolonged anorexia triggers rapid fat mobilization into liver. Next steps: FNA of liver (confirms hepatic lipidosis on cytology — large hepatocytes stuffed with lipid vacuoles), CBC/biochemistry (ALT, bilirubin ↑), and start aggressive nutritional support (esophagostomy tube or NE tube feeding immediately).
Answer: Splenic Hemangiosarcoma with hemoabdomen. The heterogeneous mass with cavitated (blood-filled) areas is classic for hemangiosarcoma in a Golden Retriever. The echogenic free abdominal fluid = blood (hemoperitoneum). Emergency stabilization (IV fluids, blood transfusion if needed) + emergency splenectomy. Poor prognosis — mean survival with surgery + chemotherapy ~4–6 months. Cardiac USG also recommended (concurrent cardiac hemangiosarcoma in right atrium is common).
Answer: Polycystic Kidney Disease (PKD). Autosomal dominant — one copy of mutant PKD1 gene causes the disease. Cysts gradually enlarge and replace functional renal tissue → eventually causing CKD. All Persian cats and Persian-derived breeds (Exotic Shorthair, British Shorthair) should be screened by USG at ≥10 months of age. At this age, sensitivity is >90%. Genetic testing (DNA test for PKD1 mutation) is also available and more sensitive. Affected cats should not be bred.
Answer: Transitional Cell Carcinoma (TCC) of the urinary bladder. The trigone location is the most common site for TCC in dogs. No shadow differentiates this from a stone. Diagnostic approach: Urine cytology (free-catch or traumatic catheter lavage — NOT cystocentesis, as needle aspiration risks needle-track seeding of tumor cells into the abdominal wall). A urine BRAF mutation test (VetMAX) is now available for non-invasive molecular diagnosis. Cystoscopic biopsy with histopathology is confirmatory if needed. Treatment: Piroxicam (NSAID — anti-tumor effect) ± mitoxantrone chemotherapy.
Answer: Pre-clinical Dilated Cardiomyopathy (Occult DCM). The enlarged LVIDd + decreased fractional shortening indicates systolic dysfunction with ventricular dilation before clinical signs develop. This is Stage B DCM in a Doberman. The dog is not symptomatic yet but is heading towards CHF. Recommend: Holter monitoring to detect occult ventricular premature contractions (VPCs) — Dobermans with occult DCM often have arrhythmias first. Treatment: Recent evidence supports starting pimobendan in pre-clinical DCM when LVIDd exceeds body-size-corrected threshold. Recheck echo every 6 months. Advise against breeding.
QUICK REFERENCE — AT-A-GLANCE ORGAN ECHOGENICITY
ECHOGENICITY BRIGHTNESS SCALE (Bright → Dark):
BRIGHTEST: Fat/Peritoneal fat, Bone cortex, Stones, Calcifications, Air interface
↓
Spleen ← MOST HYPERECHOIC solid organ
↓
Liver ← Should be slightly brighter than kidney cortex
↓
Renal Cortex ← Should be slightly darker than liver
↓
Renal Medulla ← Darker than cortex
↓
Muscle ← Hypoechoic
↓
DARKEST: Urine, Bile, Cyst fluid ← ANECHOIC (pure black)
QUICK REFERENCE — ACOUSTIC SHADOW CHART
| Causes Clean Shadow (Stone-type) | Causes Dirty Shadow (Gas-type) |
|---|---|
| Gallstones, bladder stones, kidney stones | Gas-filled bowel loops |
| Calcified lymph nodes | Pneumoperitoneum (free abdominal air) |
| Mineralized masses | Subcutaneous emphysema |
| Bone cortex | Gas-producing bacterial abscess |
| Microchip (with comet-tail) | Gastric contents |
Sources: Goldman-Cecil Medicine 22e; Textbook of Clinical Echocardiography (Otto, 5e); Yamada's Textbook of Gastroenterology 7e; Harrison's Principles of Internal Medicine 22e; Sleisenger and Fordtran's GI and Liver Disease; Histology: A Text and Atlas (Pawlina/Ross); Applied veterinary clinical knowledge for species-specific interpretation.
Jasa ultrasound keya explain wasa mujay x ray b kar do . Images lazmi dalna . Jitna ho sakay detailed . X ray in pets .
chest X-ray radiograph normal anatomy lung fields dog cat thorax
chest radiograph pneumonia consolidation lung opacity alveolar pattern
pleural effusion chest radiograph blunting costophrenic angle
pneumothorax chest radiograph collapsed lung visceral pleural line
cardiomegaly enlarged heart radiograph cardiac silhouette congestive heart failure
bone fracture X-ray radiograph long bone cortex disruption
abdominal radiograph bowel obstruction intestinal gas loops dilated
interstitial lung pattern pulmonary edema radiograph bronchovascular markings
☢️ RADIOGRAPHY (X-RAY) IN VETERINARY PRACTICE
A Complete Clinical Guide for the Veterinary Professional
Sources: Goldman-Cecil Medicine 2-Vol Set | Grainger & Allison's Diagnostic Radiology | Murray & Nadel's Textbook of Respiratory Medicine | Rosen's Emergency Medicine | Fishman's Pulmonary Diseases | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Harriet Lane Handbook | Applied Veterinary Clinical Knowledge
SECTION 1 — WHAT IS RADIOGRAPHY?
Why X-ray is Different from Ultrasound
| Feature | X-ray | Ultrasound |
|---|---|---|
| Radiation | Yes — ionizing | No |
| Best for | Bones, chest (lung/air), foreign bodies | Soft tissue, fluid, organs, pregnancy |
| Real-time | No (static image) | Yes (real-time) |
| Cost | Lower | Higher equipment cost |
| Gas/Air visualization | Excellent (black on X-ray) | Poor (gas blocks sound) |
| Bone visualization | Excellent | Limited (only surface) |
| Soft tissue detail | Limited | Excellent |
| Patient prep | Minimal | Clipping, gel, sometimes fasting |
Golden Rule: X-ray = bones, chest, air, foreign bodies. Ultrasound = soft tissue, fluid, organs.
SECTION 2 — PHYSICS OF X-RAY (MADE SIMPLE)
How X-rays Work
- An X-ray tube produces a beam of high-energy photons (X-rays)
- X-rays pass through the patient's body
- Different tissues absorb (attenuate) X-rays differently
- The remaining X-rays hit a detector (digital plate or film)
- Areas where more X-rays were absorbed = white (opaque) on image
- Areas where fewer X-rays were absorbed = black (lucent) on image
The 5 Radiographic Densities — The Foundation of X-ray Reading
WHITE ←————————————————————————————→ BLACK
Metal Bone Soft Tissue Fat Air/Gas
(most) (least)
absorbs absorbs
X-rays X-rays
| Density | Appearance | Examples |
|---|---|---|
| Metal/Mineral | Bright White (most opaque) | Surgical implants, bullets, foreign bodies, calcifications, stones |
| Bone | White/Light gray | All bones, calcified structures, teeth |
| Soft Tissue/Fluid | Medium gray | Organs (liver, heart, spleen, muscle), fluid, blood clots |
| Fat | Dark gray | Retroperitoneal fat, subcutaneous fat, fat pads |
| Air/Gas | Black (most lucent) | Lung alveoli, gas in GI tract, free air in abdomen |
The most important rule: Air is BLACK. Fluid is GRAY. Bone is WHITE. Metal is BRILLIANT WHITE.
SECTION 3 — TERMINOLOGY YOU MUST KNOW
| Term | Meaning | Example |
|---|---|---|
| Radiopaque / Opaque | Absorbs X-rays → appears WHITE | Bone, metal, mineral, fluid |
| Radiolucent / Lucent | Doesn't absorb X-rays → appears BLACK | Air, gas |
| Opacity | White area on X-ray = something there | Consolidation, fluid, mass |
| Lucency | Black area on X-ray = air or less dense tissue | Normal lung, free abdominal air |
| Silhouette sign | When two equal-density structures touch, their border disappears | Heart border lost when lung next to it fills with fluid |
| Air bronchogram | Visible dark air-filled bronchi within a white opacity | Consolidation (air in bronchi surrounded by fluid/pus-filled alveoli) |
| Density | How bright/white something appears | Increased density = more white = more fluid/tissue/mineral |
| View / Projection | The direction X-rays travel through the patient | VD, DV, Lateral, Oblique |
SECTION 4 — RADIOGRAPHIC VIEWS / POSITIONS (Very Important!)
Standard Views in Small Animal Radiography
| View Abbreviation | Full Name | Position | What It Shows Best |
|---|---|---|---|
| VD | Ventrodorsal | Patient on back (dorsal recumbency), X-ray enters ventral surface | Thorax: cardiac silhouette, lung fields symmetrically. Abdomen: symmetrical abdominal organs |
| DV | Dorsoventral | Patient on sternum (sternal recumbency), X-ray enters dorsal surface | Cardiac shape (more natural — heart settles differently), less stressful for dyspneic patients |
| RL Lat | Right Lateral | Patient lying on RIGHT side | Right lateral thorax and abdomen |
| LL Lat | Left Lateral | Patient lying on LEFT side | Left lateral thorax and abdomen |
| Oblique | Angled view | Various | Joints, specific areas |
| Skyline | Tangential view | Structure parallel to beam | Patella, nasal passages, tympanic bullae |
Why two views for every case? Always take a minimum of 2 views (lateral + VD/DV) for any body region. A mass visible only on one view may be real or may be summation artifact. Two views = 2D confirmation.
Large Animal Radiography Positions
- Standing lateral: Horse, cow — X-ray machine brought to the animal
- Portable unit: Used for limbs and head
- Horizontal beam: For thorax, abdomen in standing large animals
SECTION 5 — X-RAY MACHINE SETTINGS
The Three Exposure Factors (The Exposure Triangle)
| Setting | What It Controls | Effect |
|---|---|---|
| kVp (kilovoltage peak) | Energy of X-ray beam | Higher kVp → more penetrating beam → more contrast differences visible |
| mAs (milliampere-seconds) | Quantity of X-rays produced | Higher mAs → more X-rays → brighter image (used for thick body parts) |
| FFD/SID (focus-film distance) | Distance from tube to detector | Standard 100 cm for most views |
- Thick body part → Increase mAs
- Dense structure (bone) → Need higher kVp
- Motion blur → Reduce exposure time (increase mA, reduce seconds)
- Obese patient → Significantly increase mAs
Image Quality Terms
| Term | Problem | Fix |
|---|---|---|
| Overexposed (too dark) | Too many X-rays hit detector | Reduce mAs or kVp |
| Underexposed (too light/white) | Not enough X-rays | Increase mAs or kVp |
| Motion blur | Patient moved during exposure | Sedate patient, use faster exposure |
| Grid lines | Scattered radiation stripes | Use grid correctly, check grid alignment |
SECTION 6 — PATIENT PREPARATION FOR X-RAY
Positioning and Restraint
- Patient must be positioned accurately — a rotated or tilted view is uninterpretable
- Sedation: Often needed for proper positioning (especially lateral thoracic views)
- Manual restraint: Only when absolutely necessary — radiation protection for staff
- Foam wedges and sandbags: Used to prop the patient in position without hands in beam
Radiation Safety (CRITICAL — Every Vet Must Follow)
- Never hold a patient in the beam without lead protection — professional standard
- Lead apron, thyroid collar, and lead gloves are mandatory when near beam
- 2 meter rule: Move at least 2 meters from primary beam when possible
- Dosimetry badge: All staff working with X-rays must wear a radiation monitoring badge
- Minimize repeat exposures: Correct positioning first time — don't just "take another quick one"
- Pregnancy: Pregnant staff should NOT handle X-ray patients (even with lead protection, by policy)
- Age limit: Young animals are more radiosensitive (rapidly dividing cells) — minimize exposures
Contrast Media (For Special Studies)
- Barium sulfate: Oral or enema, shows GI tract (thick white in lumen)
- Iohexol (Omnipaque): Iodine-based water-soluble contrast — used for myelography, fistulography, cystourethrography, AngioX-ray
- DO NOT use barium if perforation suspected — use water-soluble contrast instead
SECTION 7 — HOW TO READ ANY X-RAY SYSTEMATICALLY
The ABCDE System for Chest X-ray:
A — Airway: Trachea midline? Tracheal deviation? Tracheal narrowing?
B — Bones: Rib fractures? Vertebral lesions? Scapula?
C — Cardiac silhouette: Size, shape, borders
D — Diaphragm: Both visible? Blunted angles? Elevated?
E — Everything else: Mediastinum, soft tissue, extra-thoracic structures
The ABCDE System for Abdominal X-ray:
A — Air pattern: Normal gas? Dilated loops? Free air?
B — Bones: Spine, pelvis, ribs — any lesions?
C — Contrast/Organs: Liver, spleen, kidneys visible? Normal size/position?
D — Density abnormalities: Calcifications, stones, mineral opacities?
E — Everything else: Foreign bodies, masses, extra-abdominal structures
Always complete the whole system before reporting!
SECTION 8 — THORACIC (CHEST) RADIOGRAPHY
📸 NORMAL CHEST X-RAY
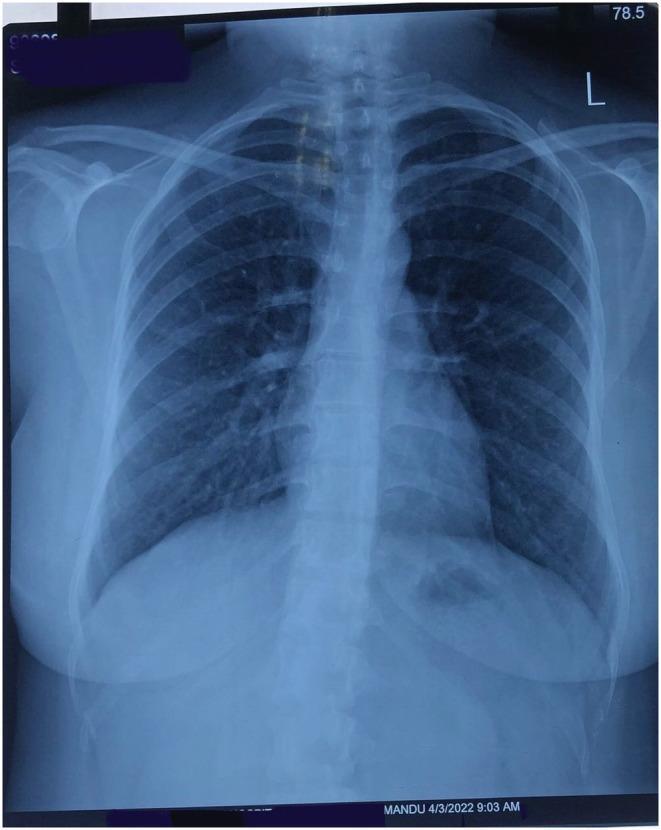
- Lungs: Black (air-filled) with faint white vascular markings spreading from hilum to periphery
- Cardiac silhouette: White/gray, clear sharp borders
- Trachea: Midline dark tubular structure
- Diaphragm: White curved lines at lung bases, both visible
- Costophrenic angles: Sharp, acute angles where diaphragm meets chest wall
- Ribs: White curved structures, symmetric
- Spine: White vertebral column in midline
🫀 CARDIAC SILHOUETTE
Vertebral Heart Scale (VHS) — The Standard Method for Dogs and Cats
- Measure the long axis of the heart from the carina to the apex
- Measure the short axis at the widest point perpendicular to long axis
- Both measurements are expressed in thoracic vertebral body lengths starting from T4
| Species | Normal VHS |
|---|---|
| Dog (most breeds) | 8.5 – 10.5 vertebral lengths |
| Cavalier CKCS | Up to 10.5 (breed variation) |
| Cat | 6.7 – 8.1 vertebral lengths |
Cardiomegaly — Enlarged Heart on X-ray
- Heart shadow wider than normal
- Cardiothoracic ratio > 0.5 (heart takes up more than 50% of chest width)
- Cardiac borders pushed against thoracic wall
- Loss of clear cardiac-lung interface
- Dilated Cardiomyopathy (DCM) — all chambers dilated → large globular heart (Dobermans, Great Danes)
- Hypertrophic Cardiomyopathy (HCM) — walls thickened (cats) → less dramatic X-ray change
- Pericardial effusion — fluid around heart → round "basketball" shape
- Valvular disease → specific chamber enlargement
- Congestive Heart Failure — combined cardiomegaly + pulmonary changes
Left Atrial Enlargement (LAE)
- On lateral view: Dorsal elevation of left mainstem bronchus
- On VD view: Bulging at 2–3 o'clock position of heart shadow
- Classic sign in dogs with Mitral Valve Disease (MMVD) — Cavalier CKCS, other small breeds
Right Heart Enlargement
- Reverse D shape (D-shaped heart on VD with flat left side)
- Seen with pulmonary hypertension, tricuspid valve disease, heartworm disease
🫁 LUNG FIELD PATTERNS
PATTERN 1: ALVEOLAR PATTERN (Consolidation)

- Bacterial Pneumonia — most common cause of lobar consolidation
- Pulmonary edema (cardiogenic — from heart failure)
- Pulmonary hemorrhage
- Lung neoplasia
- Aspiration pneumonia (common in dogs — "megaesophagus" patients)
- Contusion (trauma to lung)
- Lobar consolidation (one whole lobe) → bacterial pneumonia, aspiration
- Bilateral perihilar (near hilum) → cardiogenic pulmonary edema
- Ventral distribution → aspiration pneumonia (gravity-dependent)
- Diffuse bilateral → viral pneumonia, ARDS, severe pulmonary edema
PATTERN 2: INTERSTITIAL PATTERN

- Cardiogenic pulmonary edema — most common in veterinary patients! Left heart failure → fluid backs up into interstitium
- Non-cardiogenic pulmonary edema — toxins, near-drowning, head trauma
- Viral pneumonia
- Feline Infectious Peritonitis (FIP) — interstitial lung involvement
- Chronic interstitial disease / fibrosis
- Lungworm (Aelurostrongylus in cats, Oslerus osleri in dogs)
- Early bacterial pneumonia before alveolar filling
PATTERN 3: BRONCHIAL PATTERN
- Feline Asthma / Allergic Bronchitis — the classic cause in cats → bronchial pattern is THE most characteristic X-ray finding
- Chronic Bronchitis in dogs (especially small breeds)
- Bronchopneumonia
- Lungworm (peribronchial inflammation)
PATTERN 4: VASCULAR PATTERN
| Finding | Meaning |
|---|---|
| Enlarged pulmonary vessels (caudal lobar arteries especially) | Heartworm disease, pulmonary hypertension, left-to-right shunts (PDA, VSD) |
| Small/underfilled pulmonary vessels | Right heart failure, pulmonic stenosis (reduced right heart output) |
| Asymmetric vessel enlargement | Heartworm — classic "knobby", tortuous right caudal lobar artery |
| Caudal lobar artery > lobar vein | Pulmonary hypertension, heartworm |
- Enlarged, tortuous right caudal lobar artery — pathognomonic
- Right heart enlargement
- Perivascular haziness (eosinophilic infiltrate)
- Interstitial pattern
- "Reverse D" right heart silhouette in severe cases
PATTERN 5: MIXED PATTERN
💧 PLEURAL EFFUSION
- Blunting of the costophrenic angles (normally sharp V-shaped corners) — earliest sign
- "Meniscus sign" — curved upper fluid border
- Homogeneous white opacity at lung bases
- Fissure lines (fluid tracking along interlobar fissures)
- With large effusion: mediastinal shift away from effusion (pushed by fluid)
- Lung appears smaller/compressed
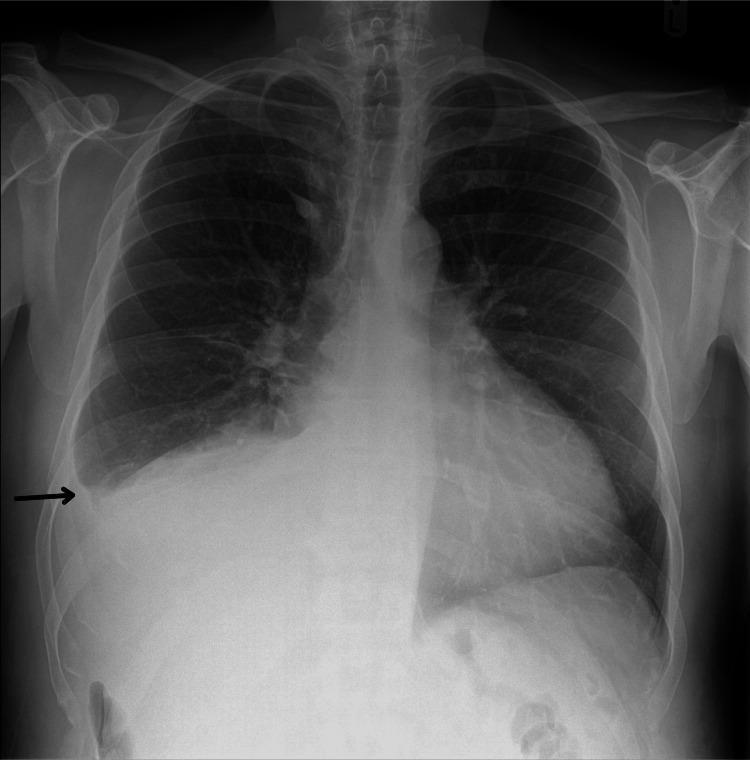
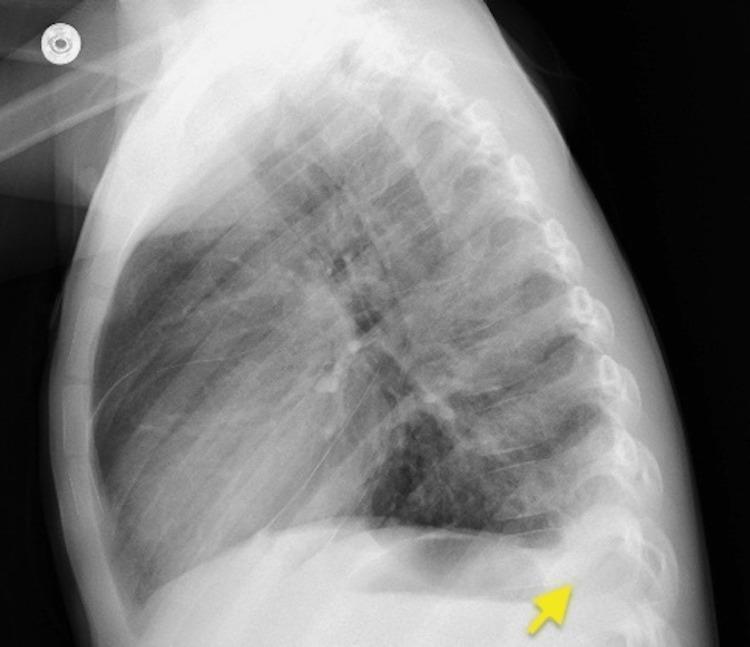
| Cause | Type of Fluid | Clue |
|---|---|---|
| Congestive Heart Failure (CHF) | Transudate | Bilateral, cardiomegaly on X-ray |
| FIP in cats | Exudate (high protein) | Usually bilateral, young cat |
| Chylothorax | Chyle (milky fluid) | Bilateral, cats and dogs, Afghans, Shiba Inus |
| Hemothorax | Blood | Trauma history, acute onset |
| Pyothorax | Pus/exudate | Often unilateral, sick patient, fever |
| Neoplasia | Variable | Older patient, mass on X-ray |
| Hypoproteinemia | Transudate | Bilateral, diffuse edema elsewhere too |
On DV view, cats with CHF often show bilateral effusion + the heart is hidden within the fluid. The heart may look "small" because it's surrounded by white fluid — this is a trap!
💨 PNEUMOTHORAX
- Visceral pleural line — the key sign: a thin white line parallel to the chest wall, with no lung markings peripheral to it (just black air space)
- Lung looks smaller/collapsed (retracted toward hilum)
- If severe: Mediastinal shift TOWARD collapsed lung (lung pulls mediastinum to it)
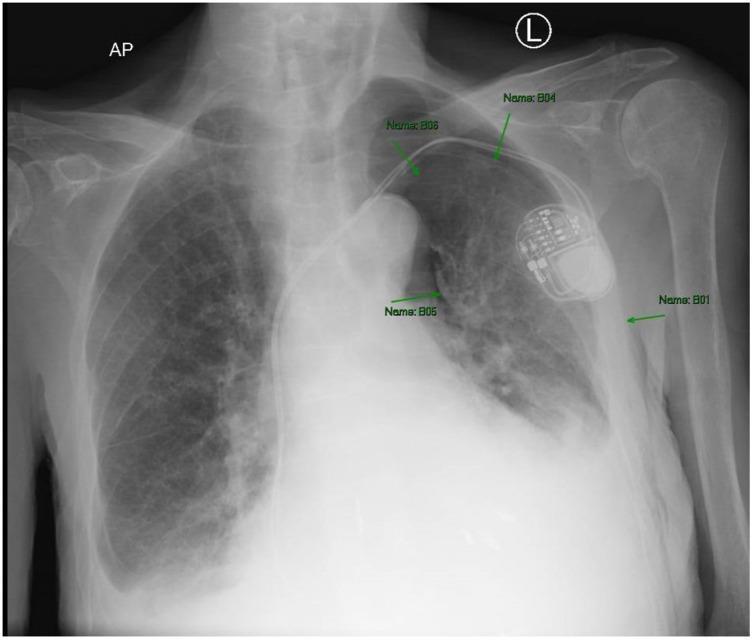
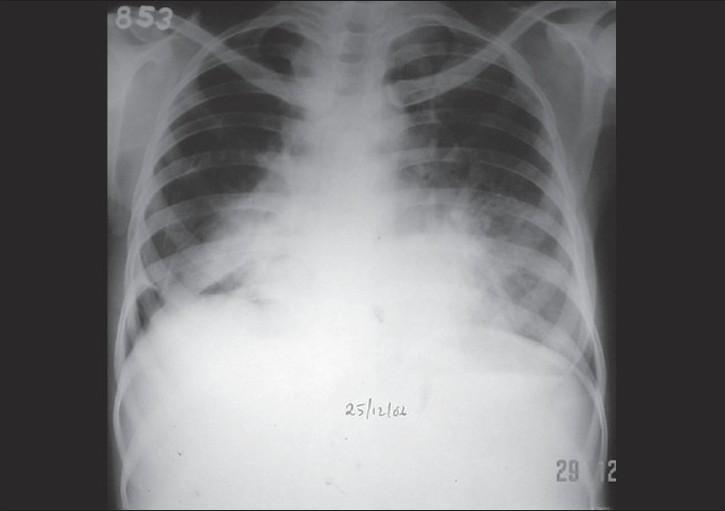
- Trauma (hit by car, bite wounds, rib fractures) — most common
- Spontaneous bullae rupture (dogs with emphysema, giant breeds)
- Pulmonary abscess rupture
- Penetrating wound
- Post-surgical (thoracic surgery complication)
- Rib fracture lacerating lung
- Mediastinal shift AWAY from the pneumothorax side
- Collapsed lung on one side + opposite lung over-expanded
- This is life-threatening — air enters but can't exit → compresses both lungs and heart
- Emergency decompression (needle thoracocentesis) immediately
📊 MEDIASTINAL CHANGES
| Finding | Cause |
|---|---|
| Widened cranial mediastinum | Mediastinal lymphoma (cats!), thymic masses, mediastinal cyst, cranial mediastinal mass |
| Tracheal deviation | Mass pushing trachea, pleural effusion |
| Pneumomediastinum | Free air in mediastinum → air around trachea and esophagus visible — from esophageal rupture, tracheal tear, trauma |
| Mediastinal shift to one side | Large effusion on opposite side OR tension pneumothorax on same side |
| Widened caudal vena cava | Right heart failure, pericardial effusion |
🐘 DIAPHRAGM
| Finding | Cause |
|---|---|
| Elevated diaphragm (one side) | Phrenic nerve damage, liver enlargement, free abdominal fluid (presses up), pain/splinting |
| Flattened diaphragm | Hyperinflation (asthma, air trapping) — diaphragm pushed down by over-expanded lungs |
| Diaphragmatic hernia | Abdominal organs in thorax — intestinal gas seen in chest, no visible diaphragm margin, displaced cardiac silhouette |
| Peritoneopericardial diaphragmatic hernia (PPDH) | Congenital — abdominal organs in pericardial sac — enlarged "rounded" cardiac silhouette |
SECTION 9 — ABDOMINAL RADIOGRAPHY
What X-ray Sees in the Abdomen
- Gas in GI tract (black)
- Fat (slightly darker than soft tissue)
- Mineral/calcification (bright white)
- Organ size and position (subtle gray differences)
Normal Abdominal X-ray Features
| Structure | Appearance |
|---|---|
| Liver | Triangular soft tissue density, cranial right abdomen |
| Spleen | Soft tissue density, left cranial/mid abdomen |
| Kidneys | Bean-shaped, retroperitoneal, visible in fat-rich patients |
| Bladder | Round/oval soft tissue at caudal abdomen |
| Stomach | Variable gas-fluid — depends on food/position |
| Small intestine | Multiple loops, small amount of gas normal, diameter < rib width |
| Large intestine | Larger diameter, peripheral, more gas |
| Spine | White vertebral column |
| Pelvis | White bony structures |
Retroperitoneal fat stripe:
🫁 GASTRIC DILATION-VOLVULUS (GDV) — THE MOST IMPORTANT ABDOMINAL EMERGENCY
- Massively gas-distended stomach
- The stomach is rotated (volvulus) — creates a compartmentalized appearance with a soft tissue band dividing the gas shadow
- The pylorus flips to the LEFT side (normally it's on the right)
- "Popeye arm" or "C-shaped" gas pattern — classic finding
Emergency surgery required within 1–2 hours. X-ray confirms diagnosis → immediate surgical intervention.
🌀 INTESTINAL OBSTRUCTION
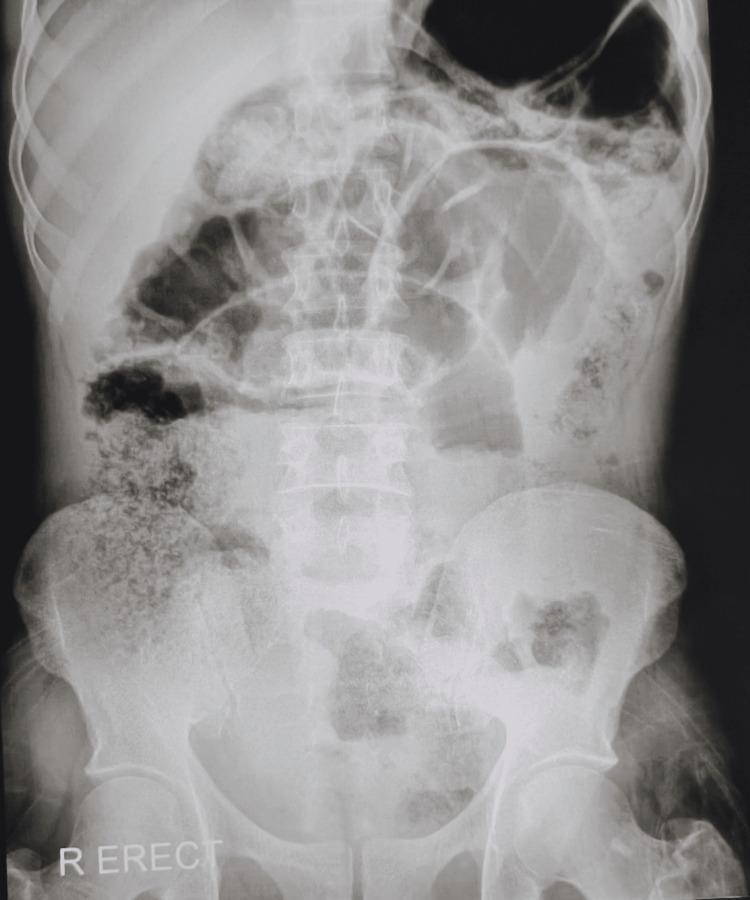

- Normal small intestine diameter in dogs: Should not exceed width of a rib body (roughly 1.5× the rib)
- Loops > 2–3× rib width = significant dilation = obstruction until proven otherwise
- Valvulae conniventes: The "stack of coins" pattern = small intestinal loops (seen as laddered lines across the loop width)
- Haustra: The bubble-like gas segments = large intestine (seen as bubbles separated by soft tissue folds)
- Dilated small intestine + no colon gas → small intestinal obstruction
- Dilated large intestine → colonic obstruction, megacolon
- Foreign body (bones, toys, corn cobs, fabric — dogs)
- Intussusception (telescoping of bowel) — mainly young animals, post-parvoviral enteritis
- Volvulus
- Mass/adhesion
- Mesenteric hernia
🟡 ABDOMINAL CALCIFICATIONS / UROLITHIASIS
| Location | Appearance | Diagnosis |
|---|---|---|
| Bladder | Round/oval mineral density inside bladder outline | Cystic calculi (bladder stones) |
| Kidney | Mineral within kidney outline | Nephrolithiasis |
| Ureter | Linear mineral along ureter course | Ureteral calculi |
| Urethra | Mineral in penile/urethral region (especially male cats/dogs) | Urethral obstruction — EMERGENCY! |
| Liver area | Mineral within liver | Hepatic mineralization, old hematoma, choleliths |
| Adrenal | Small mineral near kidney | Old adrenal lesion, pheochromocytoma |
| Prostate | Mineral in prostate region | Prostatic mineralization (benign or malignant) |
Radiolucent stones (urate, cystine, matrix) are NOT visible on plain X-ray. Need contrast study or ultrasound.
🫁 FREE ABDOMINAL AIR (PNEUMOPERITONEUM)
- On standing lateral or VD with horizontal beam: Air rises to the top (subphrenic = under diaphragm)
- Air seen between liver and diaphragm (normally they're the same gray and touch = no visible interface)
- Air under diaphragm appears as black crescent
- Gastrointestinal perforation (perforated ulcer, intestinal rupture, perforating foreign body) — most serious
- Post-surgical (normal for 2–3 weeks after abdominal surgery)
- Penetrating abdominal wound
- Rectal perforation (e.g., from bite wound, thermometer)
Free air in the abdomen in a non-surgical patient = perforation until proven otherwise → emergency surgery.
📐 ORGAN SIZE CHANGES
| Finding | Possible Causes |
|---|---|
| Hepatomegaly (enlarged liver, caudal to last rib) | Hepatitis, congestion (right heart failure), neoplasia, hyperadrenocorticism |
| Microhepatica (small liver, cranial to last rib) | Cirrhosis, portosystemic shunt (young dogs!), fibrosis |
| Splenomegaly | Sedation (acepromazine!), extramedullary hematopoiesis, splenic mass (hemangiosarcoma), lymphoma |
| Renomegaly | PKD, lymphoma (cats!), acute pyelonephritis, renal tumor |
| Bladder distension | Urethral obstruction, detrusor atony, neurogenic bladder |
| Uterine enlargement | Pyometra, pregnancy, hydrometra |
| Loss of peritoneal detail | Free abdominal fluid (ascites, hemorrhage, peritonitis) — everything looks the same gray = "ground glass" abdomen |
SECTION 10 — MUSCULOSKELETAL (BONE) RADIOGRAPHY
Normal Bone Anatomy on X-ray
Epiphysis ← Bone end (joint surface) — contains growth plate in young animals
|
Growth plate (physis) ← Dark line in growing bones — closes with maturity
|
Metaphysis ← Flared zone between growth plate and diaphysis
|
Diaphysis ← Shaft of bone — dense cortex + hollow medullary canal
|
Cortex ← Outer hard white shell
|
Medullary canal ← Inner darker channel (contains bone marrow)
|
Trabeculae ← Internal spongy bone pattern
|
Periosteum ← Outer membrane (not visible unless reacting)
Reading a Bone X-ray — What to Check:
- Cortex: Intact? Disrupted? Thinned? Thickened?
- Medullary canal: Normal density? Lucent lesion? Sclerotic?
- Periosteal reaction: Any new bone forming on outside?
- Joint space: Normal? Narrowed? Widened? Debris?
- Bone density: Normal white? Too white (sclerotic)? Too dark (osteoporosis)?
- Alignment: Fragments aligned? Displaced? Angulated?
🦴 FRACTURES

Fracture Classification (What to Report on X-ray)
| Feature | Options |
|---|---|
| Completeness | Complete (all the way through cortex) vs. Incomplete (greenstick, fissure) |
| Number of fragments | Simple (2 fragments), Comminuted (3+ fragments), Segmental |
| Displacement | Displaced (fragments shifted) vs. Non-displaced (aligned) |
| Direction of fracture line | Transverse, Oblique, Spiral, Longitudinal |
| Location | Epiphyseal, Physeal (growth plate), Metaphyseal, Diaphyseal |
| Joint involvement | Intra-articular vs. Extra-articular |
| Open vs. Closed | Soft tissue gas near fracture = open fracture |
Physeal (Growth Plate) Fractures in Young Animals
- Very important in puppies/kittens
- Salter-Harris classification:
- Type I: Slip through growth plate (whole epiphysis separates)
- Type II: Through growth plate + into metaphysis (most common)
- Type III: Through growth plate + into epiphysis (joint involved)
- Type IV: Through metaphysis + growth plate + epiphysis
- Type V: Crush of growth plate (worst — causes growth stunting)
Fracture Healing — Radiographic Stages
| Stage | Time | X-ray Appearance |
|---|---|---|
| Acute | 0–5 days | Fracture line visible, sharp edges, soft tissue swelling |
| Inflammatory | 5–14 days | Slight haziness around fracture |
| Soft callus | 14–21 days | Faint white cloud of new bone around fracture |
| Hard callus | 3–8 weeks | Dense white callus bridging the gap |
| Remodeling | Months–years | Callus shrinks, bone shape restored, fracture line disappears |
If no callus is forming at 3–4 weeks = delayed union. If fracture site remains mobile and no union by 4+ months = non-union → surgical intervention needed.
🦴 BONE LESIONS (Lytic vs. Proliferative)
| Pattern | Appearance | Think |
|---|---|---|
| Lytic lesion | Dark holes in bone — bone being destroyed | Neoplasia (osteosarcoma, metastasis), infection (osteomyelitis), cyst |
| Sclerotic lesion | Extra white bone density | Reactive new bone, osteoma, healed osteomyelitis, blastic metastasis |
| Mixed lytic/proliferative | Both dark holes AND irregular white new bone | Osteosarcoma (classic "sunburst" or "Codman's triangle" pattern) |
| Periosteal reaction | Spiculated (sunburst) or smooth new bone on surface | Osteosarcoma (aggressive irregular) vs. healing (smooth) |
- Typically affects metaphysis of long bones in large/giant breeds
- Distal radius, proximal humerus, distal femur, proximal tibia most common locations
- X-ray: Aggressive bone destruction (lytic) + sunburst periosteal reaction + soft tissue swelling
- May see Codman's triangle (elevation of periosteum at edge of tumor)
- Virtually no normal periosteal reaction = very aggressive = poor prognosis
🐾 JOINT RADIOGRAPHY
| Finding | Meaning |
|---|---|
| Narrowed joint space | Cartilage loss = Osteoarthritis (OA) / Degenerative Joint Disease (DJD) |
| Osteophytes (bone spurs) | New bone at joint margins = chronic OA |
| Joint effusion | Widened joint space (fluid pushing bones apart) + soft tissue swelling |
| Subchondral sclerosis | Dense white bone just under cartilage = OA response |
| Joint mice (mineral fragments in joint) | OA fragments, osteochondrosis dissecans (OCD) |
| Luxation | Joint surfaces not aligned |
| Subluxation | Partial misalignment of joint surfaces |
- OFA (Orthopedic Foundation for Animals) extended hip view
- Evaluated at 2 years of age for certification
- Signs: Shallow acetabulum, femoral head subluxation, DJD, remodeling of femoral head
- PennHIP method: Distraction index (DI) measured — the gold standard for predicting HD development
- Fragmented medial coronoid process (FCP), OCD of humeral condyle, ununited anconeal process (UAP)
- X-ray: Elbow OA (osteophytes at anconeal process area), widened humeroradial joint space, sclerosis
- X-ray findings: Cranial tibial thrust, stifle effusion (loss of fat pad, widened joint space), periarticular osteophytes (chronic)
- X-ray does not show the ligament itself — diagnosis is clinical/arthroscopic
🦷 DENTAL / SKULL RADIOGRAPHY
- Intraoral technique — plates placed inside mouth
- Show tooth roots, periodontal ligament space, alveolar bone
- Essential for: Tooth root abscesses, feline tooth resorption, periodontal disease grading
- DV (dorsoventral) — nasal cavities, frontal sinuses, skull
- Lateral — skull profile, teeth, tympanic bullae
- Rostrocaudal (open mouth) — tympanic bullae (otitis media/interna cases)
- VD oblique — temporomandibular joint
- Chronic otitis externa → otitis media → fluid/thickening in bulla
- X-ray: Increased opacity (white) in bulla = fluid or thickening. Loss of sharp outline = aggressive disease
SECTION 11 — SPINAL RADIOGRAPHY
Views:
- Lateral: Intervertebral disc spaces, vertebral body alignment, osteophytes
- VD: Disc spaces, vertebral width, narrowing
What to Look For:
| Finding | Meaning |
|---|---|
| Narrowed intervertebral disc space | Disc degeneration or herniation |
| Calcified disc material | Chondrodystrophic breeds (Dachshund, CKCS, Pekingese) — mineralized nucleus pulposus → prone to Hansen Type I disc herniation |
| Bridging spondylosis | White bone bridges between vertebrae = chronic disc disease/stress |
| Vertebral fracture/luxation | Trauma — assess alignment |
| Lytic vertebral lesion | Discospondylitis (infection), neoplasia, multiple myeloma |
| Sclerosis of vertebral end-plates | Discospondylitis (infection — classically Brucella, Staphylococcus) |
| "Moth-eaten" vertebrae | Aggressive bone disease — neoplasia |
SECTION 12 — CONTRAST RADIOGRAPHY
Common Contrast Studies in Veterinary Practice
| Study | Contrast Agent | What It Shows | When Used |
|---|---|---|---|
| Upper GI series (UGI) | Barium sulfate PO | Esophagus, stomach, small intestine | Esophageal foreign body, megaesophagus, mass, stricture, delayed gastric emptying |
| Barium enema | Barium per rectum | Large intestine | Colonic mass, intussusception |
| IVP (Intravenous Pyelogram) | IV iodinated contrast | Kidneys, ureters, bladder | Ureteral ectopia, renal function, ureter obstruction |
| Cystourethrogram | Contrast via catheter into bladder | Bladder and urethra | TCC location, urethral stricture, bladder rupture |
| Myelogram | Intrathecal iohexol | Spinal cord, intervertebral discs | Disc herniation, spinal tumor, cord compression |
| Fistulogram | Iodinated contrast in fistula tract | Draining tract course | Bite wound tracts, deep infection |
| Arthrography | Contrast into joint | Joint surfaces, ligaments | OCD defects, joint disease |
- Megaesophagus: Massively dilated esophagus filled with barium
- Esophageal foreign body: Filling defect (where barium can't flow = object is there)
- Hiatal hernia: Stomach herniating through diaphragm
SECTION 13 — AGE-SPECIFIC RADIOGRAPHIC FINDINGS
| Age | Species | Finding | Significance |
|---|---|---|---|
| Neonates | All | Open growth plates (dark lines at epiphyses), unfused bones, incompletely ossified carpal/tarsal bones | Normal — do not over-interpret |
| Puppies/Kittens < 6 months | All | Thymus visible as white triangle in cranial mediastinum | Normal — NOT a mass! |
| < 8 months (dogs) | Dogs | Open physes — don't mistake growth plate as fracture | Normal physeal lines are bilateral and symmetric |
| Chondrodystrophic breeds (any age) | Dachshund, CKCS, Pekingese, Basset | Multiple calcified intervertebral discs | These dogs are HIGH RISK for IVDD — even single episode → full spinal series |
| Middle-aged intact male dogs | Dogs | Prostatic enlargement visible on VD | BPH very common in intact males >5 years |
| Middle-aged to senior (> 7 years) | Dogs | Intervertebral disc calcifications, spondylosis, joint osteophytes | Normal aging changes — compare with clinical signs |
| Senior cats (> 10 years) | Cats | Articular osteophytes in spine (thoracolumbar), muscle atrophy | Feline spondylosis — very common, underdiagnosed |
| Any age — large/giant breeds | Dogs | GDV risk → any acute abdomen = consider GDV | Emergency X-ray protocol |
| Young large breeds (< 2 years) | GSD, Lab, Golden | OCD lesions at shoulder/stifle, HD | Screen before clinical signs worsen |
| Persian cats (any age) | Cats | Renomegaly with smooth surface (PKD cysts too small for X-ray) | Use USG for PKD — X-ray underestimates |
| Any age — Cavalier CKCS | Dogs | Enlarged cardiac silhouette, left atrial enlargement | MMVD screening — VHS useful |
SECTION 14 — RADIOGRAPHIC SIGNS SUMMARY TABLE
Chest X-ray Signs
| Sign | Appearance | Meaning |
|---|---|---|
| Air bronchogram | Dark bronchi within white opacity | Alveolar consolidation (pneumonia, edema) |
| Silhouette sign | Loss of border between two structures | Both structures same density = disease process touching normal structure |
| Kerley B lines | Horizontal lines at lung periphery | Interstitial edema (CHF) |
| Bat-wing/butterfly pattern | Bilateral perihilar white opacity | Pulmonary edema |
| Sail sign | Triangular white thymic shadow in young animal | Normal thymus — NOT a mass |
| Tracheal elevation (dorsal) | Trachea displaced dorsally | Left atrial enlargement (MMVD in dogs) |
| Reverse D heart | Straight left heart border on VD | Right heart enlargement |
| Blunted costophrenic angle | Lost sharp corner at lung base | Pleural effusion |
| Visceral pleural line | White line with no markings peripheral to it | Pneumothorax |
| Meniscus sign | Curved fluid upper border | Free pleural fluid |
Abdominal X-ray Signs
| Sign | Appearance | Meaning |
|---|---|---|
| Ground glass abdomen | Loss of abdominal detail, everything gray | Free abdominal fluid (ascites, hemorrhage, peritonitis) |
| Coffee bean sign | Gas-filled loop shaped like coffee bean with central stripe | Sigmoid or cecal volvulus |
| String of pearls | Small gas bubbles in a row | Air trapped in intestinal mucosal folds = obstruction |
| Free subphrenic air | Air visible under diaphragm | Perforation |
| Double bubble | Two gas compartments | GDV (most common), or duodenal atresia in neonates |
| Displacement of colon | Colon pushed caudally/laterally | Hepatomegaly, large abdominal mass |
| Loss of kidney outline | Kidney not visible/distinct | Retroperitoneal fluid, mass effacement |
| Compartmentalized gas in stomach | Gas divided by soft tissue band | GDV — pylorus rotated |
SECTION 15 — PRACTICE QUESTIONS
Answer: Take right lateral AND VD views immediately (before more deterioration). Expected findings: Massively gas-distended stomach with compartmentalization (soft tissue band dividing the gas = the pyloric/duodenal wall rotated across the gas shadow). On lateral: gas-filled stomach with "double bubble" compartment. On VD: stomach extends across entire cranial abdomen. Small intestinal gas-distension (secondary ileus). Spleen may be displaced. Diagnosis = GDV. Do NOT delay for more views. Emergency surgery within 1 hour after stabilization (IV fluids + decompression). If left untreated → gastric necrosis, shock, death.
Answer: Lateral and VD thoracolumbar spine X-rays. Expected findings: Calcified intervertebral disc material in multiple disc spaces (characteristic of chondrodystrophic breeds — Dachshunds calcify their nucleus pulposus). Look for narrowed disc space at the level correlating with the neurological deficits. May see extruded calcified disc material in the spinal canal (ventral floor of canal appearing white). However, X-ray alone cannot rule out disc herniation — myelogram or CT/MRI is required to confirm and localize. This is Hansen Type I IVDD — emergency decompressive surgery (hemilaminectomy) if deep pain is absent or rapidly deteriorating.
Answer: Congestive Heart Failure (CHF) secondary to Myxomatous Mitral Valve Disease (MMVD). The enlarged cardiac silhouette = cardiomegaly. The 2–3 o'clock bulge on VD = left atrial enlargement (pathognomonic for MMVD in Cavaliers). Perihilar haze = early pulmonary edema (cardiogenic — left heart failure → backup of fluid into pulmonary interstitium). Treatment: Furosemide (diuretic) + pimobendan + ACE inhibitor. Confirm with echocardiography (mitral regurgitation, LA:Ao ratio, FS%). VHS would be >10.5 vertebral lengths.
Answer: Bilateral pleural effusion + cardiomegaly → most likely CHF from HCM (hypertrophic cardiomyopathy) OR chylothorax or FIP in a young cat. First priority: Do NOT stress the cat more — DV view was correct choice (less stressful than VD for dyspneic cats). Immediate treatment: Bilateral thoracocentesis (remove pleural fluid → cat can breathe) BEFORE any further diagnostics. After stabilization: Echocardiogram (assess HCM), fluid analysis (chylothorax vs. transudate vs. FIP exudate). If young cat with bilateral effusion = consider FIP (coronavirus) — check for globulins, A:G ratio.
Answer: Left-sided tension pneumothorax. The pleural line = air in pleural space collapsing the left lung. The rightward mediastinal shift = air under pressure pushing everything to the right = tension pneumothorax (most dangerous form). Immediate emergency needle decompression: Insert 18G butterfly catheter/needle in the dorsal 7th–9th intercostal space (high up — air rises) of the left side. Release the pressure. Follow with chest drain placement. The patient may arrest without immediate decompression. Do NOT delay for more X-rays. After decompression: reassess with follow-up X-ray, look for underlying rib fractures, lung contusions, diaphragmatic hernia.
QUICK REFERENCE CARD — WHAT TO LOOK FOR ON EACH X-RAY
Chest X-ray Checklist
☐ Trachea: midline? deviated? narrowed?
☐ Cardiac silhouette: size (VHS)? shape? borders sharp?
☐ Left atrium: tracheal elevation? 2-3 o'clock bulge?
☐ Pulmonary vessels: normal? enlarged? asymmetric?
☐ Lung fields: any opacity? which pattern? (alveolar/interstitial/bronchial/vascular)
☐ Pleural space: costophrenic angles sharp? any effusion? any pleural line?
☐ Diaphragm: both crura visible? elevated? interrupted (hernia)?
☐ Mediastinum: width normal? any mass? pneumomediastinum?
☐ Bones: rib fractures? vertebral lesions? scapular fracture?
☐ Extra-thoracic: any subcutaneous gas? foreign material?
Abdominal X-ray Checklist
☐ Serosal detail: sharp (normal)? hazy (fluid)? absent (serious)?
☐ Liver size: within costal arch? extended caudally?
☐ Spleen: visible? enlarged?
☐ Kidneys: visible? size? position? calcification?
☐ Bladder: visible? size? any calcification?
☐ Stomach: gas? normal position? compartmentalized (GDV)?
☐ Small intestine: diameter vs. rib? dilated loops? air-fluid levels?
☐ Large intestine: diameter? obstruction? megacolon?
☐ Free air: subphrenic? outlining organs?
☐ Calcifications: location? size? shape?
☐ Bones: spine alignment? vertebral lesions? pelvic fractures?
☐ Uterus: visible? enlarged (pyometra/pregnancy)?
Sources: Grainger & Allison's Diagnostic Radiology (Elsevier); Murray & Nadel's Textbook of Respiratory Medicine (Elsevier); Rosen's Emergency Medicine (Elsevier); Fishman's Pulmonary Diseases and Disorders (McGraw-Hill); Roberts & Hedges' Clinical Procedures in Emergency Medicine (Elsevier); Goldman-Cecil Medicine International Edition; The Harriet Lane Handbook 23e; Applied veterinary species-specific radiographic knowledge.
Left and rft and helth check in pets a to z details everything including without any missing. From vet sources . Explain as much as u can easy English
🧪 LFT + RFT + COMPLETE HEALTH CHECK IN PETS
The Most Detailed Clinical Guide for Veterinary Practice
Sources: Henry's Clinical Diagnosis & Management by Laboratory Methods | Washington Manual of Medical Therapeutics | Robbins & Kumar Basic Pathology | Quick Compendium of Clinical Pathology 5e | Tietz Textbook of Laboratory Medicine 7e | Barash Clinical Anesthesia 9e | Morgan & Mikhail's Clinical Anesthesiology 7e | Brenner & Rector's The Kidney | Applied Veterinary Clinical Knowledge
UNDERSTANDING THE BLOOD BIOCHEMISTRY PANEL
- LFT (Liver Function Tests) — Checks if the liver is healthy
- RFT (Renal Function Tests) — Checks if the kidneys are healthy
═══════════════════════════════════
PART 1 — LFT: LIVER FUNCTION TESTS
═══════════════════════════════════
Why the Liver Matters
- Breaks down fats, carbohydrates, proteins
- Produces bile (for fat digestion)
- Detoxifies drugs, toxins, ammonia
- Makes blood clotting factors (prothrombin, fibrinogen)
- Makes albumin (the main blood protein)
- Stores glycogen (energy reserve)
- Converts bilirubin for excretion
If the liver fails → the whole body fails. LFTs tell you HOW the liver is failing and WHY.
LFT TEST 1: ALT — Alanine Aminotransferase
| Species | Normal ALT (U/L) |
|---|---|
| Dog | 10 – 100 |
| Cat | 10 – 75 |
| Horse | 3 – 23 |
| Cow | 11 – 40 |
Species note: ALT is most useful in dogs and cats. In horses and ruminants (cows, goats, sheep), ALT is not as liver-specific.
| Level of Elevation | What It Means |
|---|---|
| Mild (1–3× normal) | Mild hepatocellular stress — drug side effects, early fatty liver, subclinical disease |
| Moderate (3–10× normal) | Active hepatocellular damage — hepatitis, toxin exposure, infectious disease |
| Severe (>10× normal) | Major liver damage — acute hepatitis, hepatic necrosis, toxin (xylitol, aflatoxin, acetaminophen in cats), leptospirosis |
| Extreme (>50× normal) | Massive liver necrosis — usually a poor sign |
- Hepatitis (bacterial, viral, autoimmune — copper-associated hepatitis in Bedlington Terriers, Labradors)
- Toxins: Xylitol (dogs — found in sugar-free gum, peanut butter!), aflatoxin (contaminated food), mushrooms (Amanita), blue-green algae
- Acetaminophen (Paracetamol): Deadly in cats — causes hepatic necrosis + methemoglobinemia. Never give paracetamol to cats!
- Corticosteroids (dogs only) → steroid hepatopathy → vacuolar change → ALT 3–10× — important to know because many dogs are on steroids
- Diabetes mellitus → hepatic lipidosis secondary to insulin deficiency
- Hyperthyroidism (cats) → liver enzyme elevation common
- Pancreatitis → adjacent inflammation raises ALT
- Hypothyroidism (dogs) → hepatic lipid accumulation
- Cushing's disease (hyperadrenocorticism) → steroid hepatopathy → very high ALT
- Portosystemic shunt (PSS) → liver not getting adequate blood flow → enzyme changes
LFT TEST 2: AST — Aspartate Aminotransferase
| Species | Normal AST (U/L) |
|---|---|
| Dog | 10 – 40 |
| Cat | 10 – 40 |
| Horse | 220 – 600 |
| Cow | 50 – 100 |
- Liver damage (hepatocellular — same as ALT)
- Muscle damage (rhabdomyolysis, trauma, myositis, excessive exercise, IM injections)
- Hemolysis (RBC contain AST → broken RBCs release it)
- Cardiac muscle damage (myocarditis)
- Sample artifact — hemolyzed sample falsely elevates AST
| Pattern | Meaning |
|---|---|
| ALT ↑↑ + AST ↑ (ALT > AST) | Hepatocellular disease → liver is the source |
| AST ↑↑ + ALT normal or slightly ↑ | Muscle damage (rhabdomyolysis, myopathy) → muscle is the source |
| Both very high equally | Liver + muscle both involved, OR severe acute hepatic necrosis |
Practical tip: If AST is high but ALT is normal → check creatine kinase (CK) to confirm muscle damage.
LFT TEST 3: ALP — Alkaline Phosphatase (SAP — Serum Alkaline Phosphatase)
| Species | Normal ALP (U/L) |
|---|---|
| Dog | 20 – 150 |
| Cat | 10 – 90 |
| Horse | 100 – 500 |
| Cow | 30 – 200 |
| Cause | Mechanism | Notes |
|---|---|---|
| Biliary obstruction (extrahepatic) | Bile backed up → ALP leaks | Pancreatitis compressing bile duct, cholelith, bile duct tumor |
| Intrahepatic cholestasis | Bile not flowing within liver | Hepatitis, cholangiohepatitis (cats!), toxic hepatopathy |
| Corticosteroids | Induces liver ALP isoenzyme | DOGS ONLY — major cause of high ALP. Exogenous steroids (treatment) OR endogenous (Cushing's disease). Cat liver does NOT have steroid-induced ALP isoenzyme |
| Cushing's disease | Cortisol excess → steroid-induced ALP | ALP can be 5–50× normal in Cushing's dogs |
| Bone disease | Bone-derived ALP | Growing puppies (normal!), bone tumors (osteosarcoma), bone fractures healing |
| Hyperthyroidism | Cats | Common finding in hyperthyroid cats |
| Diabetes mellitus | Secondary hepatic lipidosis | |
| Hepatic neoplasia | Space-occupying lesions → cholestasis |
- Dog: ALP elevation is very common due to steroid-induced enzyme. Always check if dog is receiving ANY steroid (prednisone, dexamethasone, even topical ear drops!)
- Cat: ALP elevation is MORE concerning in cats because cats DON'T have the steroid-induced isoenzyme. A high ALP in a cat usually means significant liver disease or cholestasis. Even 2× normal in a cat = worth investigating.
LFT TEST 4: GGT — Gamma Glutamyl Transferase (Gamma GT)
| Species | Normal GGT (U/L) |
|---|---|
| Dog | 2 – 10 |
| Cat | 0 – 5 |
| Horse | 5 – 25 |
| Cow | 10 – 50 |
- Biliary obstruction (extra or intrahepatic cholestasis) — THE most sensitive marker
- Cholangiohepatitis in cats — GGT is elevated more often than ALP in cats with hepatic lipidosis
- Corticosteroids in dogs (same as ALP)
- Pancreatic disease
- Bile duct hyperplasia
- In cats: GGT is the better biliary marker than ALP
- In cats with hepatic lipidosis: ALP is usually very high but GGT is often normal or only mildly elevated — this pattern (high ALP + normal/low GGT in a cat) is strongly suggestive of hepatic lipidosis
- If both ALP and GGT are high → true biliary disease or cholangiohepatitis
LFT TEST 5: BILIRUBIN (Total, Direct/Conjugated, Indirect/Unconjugated)
Bilirubin Pathway (Simplified):
Old RBC destroyed
↓
Hemoglobin → Heme → Unconjugated (Indirect) Bilirubin
↓ (travels in blood bound to albumin)
Liver picks it up
↓
Liver adds glucuronide → Conjugated (Direct) Bilirubin
↓
Secreted into bile → goes to intestines → excreted in feces (gives stool its brown color)
→ some converted to urobilinogen → goes to urine (yellow color)
| Species | Normal Total Bilirubin (mg/dL) |
|---|---|
| Dog | 0 – 0.3 |
| Cat | 0 – 0.3 |
| Horse | 0.5 – 3.5 (higher due to fasting) |
| Cow | 0 – 0.5 |
The Three Types of Jaundice — Most Important Clinical Tool:
TYPE 1: PRE-HEPATIC JAUNDICE (Hemolytic)
- Cause: Too many RBCs being destroyed → too much bilirubin produced → overwhelms liver
- Bilirubin pattern: Mainly UNCONJUGATED (indirect) elevated
- Urine: Normal (no bilirubin in urine — unconjugated bilirubin bound to albumin, can't pass through kidney)
- Urobilinogen: Increased (more bilirubin reaching gut)
- Liver enzymes: Normal or mildly elevated (liver is fine)
- RBC: Low — anemia present
- Examples: IMHA (immune-mediated hemolytic anemia), Babesia, Hemobartonella, severe hemolysis
TYPE 2: HEPATIC JAUNDICE (Liver Disease)
- Cause: Liver cannot process bilirubin properly
- Bilirubin pattern: BOTH conjugated AND unconjugated elevated
- Urine bilirubin: Present (conjugated bilirubin can pass through kidney)
- Urobilinogen: Variable
- Liver enzymes: HIGH (ALT, ALP, GGT elevated)
- Examples: Acute hepatitis, cirrhosis, hepatic lipidosis in cats, leptospirosis, hepatic lymphoma
TYPE 3: POST-HEPATIC JAUNDICE (Obstructive)
- Cause: Bile cannot flow out of liver/bile duct → bilirubin backs up
- Bilirubin pattern: Mainly CONJUGATED (direct) elevated
- Urine bilirubin: Present (dark brown "tea-colored" urine)
- Urobilinogen: ABSENT or very low (bile not reaching gut)
- Feces: Pale/acholic (no bilirubin in stool → stool turns pale/white)
- Liver enzymes: ALP and GGT especially elevated
- Examples: Pancreatitis compressing bile duct, gallbladder mucocele (dogs), cholelith, bile duct carcinoma, duodenal mass
Icterus Quick Recognition Chart:
| Finding | Pre-hepatic | Hepatic | Post-hepatic |
|---|---|---|---|
| Mucous membranes | Yellow | Yellow | Deep yellow/orange |
| Urine color | Normal/yellow | Dark yellow | Very dark "tea" color |
| Stool color | Normal/dark | Normal or pale | PALE/acholic |
| ALT/ALP | Normal | High | ALP especially high |
| Anemia | YES (hemolytic) | Possible | No (unless chronic) |
| Conjugated bilirubin | Normal | High | Very High |
| Unconjugated bilirubin | Very High | High | Normal/slightly ↑ |
LFT TEST 6: BILE ACIDS (Fasting and Post-Prandial)
| Species | Fasting Bile Acids (µmol/L) | Post-prandial (2-hour) |
|---|---|---|
| Dog | < 5 | < 25 |
| Cat | < 5 | < 10 |
- Take blood sample after 12-hour fast → Fasting bile acids
- Feed a small meal
- Take blood sample again 2 hours later → Post-prandial bile acids
- Portosystemic Shunt (PSS) — the #1 most common cause in young animals. Blood bypasses the liver → bile acids not cleared → very high levels. This is the BEST diagnostic test for PSS.
- Chronic liver disease (cirrhosis, hepatitis)
- Hepatic lipidosis (cats)
- Any cause of reduced hepatic function
LFT TEST 7: ALBUMIN
| Species | Normal Albumin (g/dL) |
|---|---|
| Dog | 2.5 – 4.0 |
| Cat | 2.1 – 3.3 |
| Horse | 2.5 – 4.0 |
| Cow | 2.5 – 3.5 |
| Cause | Mechanism | Other Clues |
|---|---|---|
| Liver failure | Liver not making enough albumin | High bilirubin, high bile acids, high enzymes |
| Protein-losing enteropathy (PLE) | Protein leaking out through diseased gut | Low globulins too, diarrhea, weight loss |
| Protein-losing nephropathy (PLN) | Protein leaking through damaged glomeruli | Proteinuria on urinalysis, normal globulins |
| Malnutrition / Starvation | Not enough protein in diet | Thin patient, low BCS |
| Chronic blood loss | Protein lost with blood | Anemia, low PCV |
| Third-space losses | Fluid leaking into body cavities | Ascites, pleural effusion, edema |
| Burns | Protein lost through skin | History of severe burns |
- Peripheral edema (fluid accumulates under skin — especially limbs, face, ventral body)
- Ascites (fluid in abdomen)
- Pleural effusion (fluid in chest)
- Caveat: Signs usually appear when albumin < 1.5–2.0 g/dL
LFT TEST 8: TOTAL PROTEIN and GLOBULINS
| Species | Normal Total Protein (g/dL) |
|---|---|
| Dog | 5.4 – 7.8 |
| Cat | 6.0 – 8.4 |
| Horse | 5.5 – 8.0 |
- Chronic infection/inflammation — body producing lots of antibodies
- FIP in cats — very high globulins (often >5 g/dL), low albumin → A:G ratio < 0.8 = very suspicious for FIP
- Multiple myeloma (plasma cell cancer) — monoclonal spike on protein electrophoresis
- Ehrlichiosis — tick-borne disease, chronic → very high globulins
- Leishmaniasis — endemic in Mediterranean regions, dogs
- Brucellosis — chronic infection
- Immunodeficiency
- Neonatal animals who haven't received colostrum (failure of passive transfer)
- Protein-losing enteropathy (all proteins lost equally)
- Normal: 0.8 – 2.0
- A:G < 0.5 in a cat with ascites/effusion = FIP until proven otherwise (the most important use of this ratio)
LFT TEST 9: PROTHROMBIN TIME (PT) and aPTT
- PT (Prothrombin Time): Tests extrinsic clotting pathway (factors I, II, V, VII, X)
- aPTT: Tests intrinsic pathway (factors I, II, V, VIII, IX, X, XI, XII)
- Severe liver failure — liver not making clotting factors → spontaneous bleeding
- Rodenticide toxicity (anticoagulant rat poison) — warfarin/brodifacoum → inhibits Vitamin K-dependent clotting factors (II, VII, IX, X) → PT prolonged first (VII has shortest half-life)
- DIC (Disseminated Intravascular Coagulation) — both PT and aPTT prolonged + thrombocytopenia
- Vitamin K deficiency — fat malabsorption (obstructive jaundice)
- Inherited coagulopathy (von Willebrand disease, hemophilia A/B)
LFT TEST 10: AMMONIA
- Seizures, disorientation, circling, head pressing, ptyalism (drooling), stupor, coma
- Classic in dogs with portosystemic shunts (PSS) — especially after a protein meal
- In cats: hyperactivity, aggression, then depression
- Also elevated in severe acute liver failure
LFT TEST 11: CHOLESTEROL
| ↑ High Cholesterol | ↓ Low Cholesterol |
|---|---|
| Hypothyroidism (dogs) — most common! | Severe liver disease (liver can't make it) |
| Cushing's disease | Portosystemic shunt |
| Diabetes mellitus | Malabsorption, PLE |
| Nephrotic syndrome (protein-losing nephropathy) | Hypoadrenocorticism (Addison's) |
| Post-prandial (normal after eating) | |
| Pancreatitis | |
| Primary hyperlipidemia (Miniature Schnauzers) |
LFT TEST 12: GLUCOSE
- Diabetes mellitus — most common cause
- Stress (cats especially — can be 300+ mg/dL from stress alone)
- Pancreatitis (destroys insulin-producing cells)
- Glucocorticoids (steroid treatment or Cushing's)
- Glucagonoma (rare)
- Insulinoma — insulin-producing pancreatic tumor (Boxers, Labrador Retrievers, Irish Setters)
- Neonatal/juvenile hypoglycemia — toy breeds, puppies not eating
- Addison's disease (hypoadrenocorticism)
- Septic shock (bacteria consuming glucose)
- Hepatic failure (liver can't maintain glucose stores)
- Hunting dog hypoglycemia — extreme exercise in poorly fed dog
- Xylitol toxicity (dogs) — xylitol triggers massive insulin release → severe hypoglycemia
COMPLETE LFT SUMMARY TABLE
| Test | Measures | ↑ High Means | ↓ Low Means |
|---|---|---|---|
| ALT | Hepatocyte damage | Active liver cell injury | Rarely significant (end-stage) |
| AST | Hepatocyte/muscle damage | Liver OR muscle injury | Not significant |
| ALP | Cholestasis / bone | Biliary obstruction, steroids (dogs), Cushing's, bone | Not significant |
| GGT | Biliary epithelium | Cholestasis, biliary disease | Not significant |
| Total Bilirubin | Bile metabolism | Hemolysis/liver disease/obstruction | Not significant |
| Direct Bilirubin | Conjugated fraction | Hepatic/post-hepatic jaundice | Normal state |
| Indirect Bilirubin | Unconjugated fraction | Hemolytic/pre-hepatic jaundice | Normal state |
| Bile Acids | Liver function (enterohepatic) | PSS, liver failure, hepatitis | Not significant |
| Albumin | Liver synthesis | (Dehydration — hemoconcentration) | Liver failure, PLE, PLN, malnutrition |
| Total Protein | All proteins | Inflammation, FIP, myeloma | Liver failure, malnutrition, losses |
| Globulins | Immune proteins | Chronic infection, FIP, ehrlichiosis | Neonatal, immunodeficiency |
| PT/aPTT | Clotting | Rodenticide, DIC, liver failure | Not significant |
| Ammonia | Liver detoxification | PSS, liver failure → encephalopathy | Not significant |
| Cholesterol | Lipid metabolism | Hypothyroidism, Cushing's, DM | Liver failure, PSS, malabsorption |
| Glucose | Energy metabolism | DM, stress, steroids | Insulinoma, Addison's, neonatal |
═══════════════════════════════════
PART 2 — RFT: RENAL FUNCTION TESTS
═══════════════════════════════════
Why Kidneys Matter
- Filter blood 60× per day → remove waste products (urea, creatinine, toxins)
- Regulate water balance (concentrated or dilute urine)
- Control blood pressure (renin-angiotensin system)
- Maintain electrolyte balance (Na, K, Ca, Phosphorus)
- Produce erythropoietin (stimulates RBC production)
- Activate Vitamin D
Kidneys have HUGE reserve capacity — by the time BUN and creatinine become abnormal, 75% of kidney function is already lost. This is why early detection tests like SDMA are so important.
RFT TEST 1: BUN — Blood Urea Nitrogen
| Species | Normal BUN (mg/dL) |
|---|---|
| Dog | 7 – 27 |
| Cat | 15 – 35 |
| Horse | 10 – 25 |
| Cow | 10 – 25 |
| BUN:Creatinine Ratio | Interpretation |
|---|---|
| Normal: 10:1 to 20:1 | Normal kidney function |
| > 20:1 (BUN disproportionately high) | Pre-renal azotemia — dehydration, reduced blood flow to kidneys, protein-rich diet, GI bleeding (blood digested → protein → urea) |
| 10:1 to 20:1 with both elevated | Renal azotemia — true kidney disease |
| < 10:1 (creatinine high, BUN relatively low) | Liver disease (liver not making urea from protein), low protein diet, polyuria/polydipsia |
- Dehydration (most common!) — concentrated blood → high BUN → called "prerenal azotemia"
- Acute or Chronic Kidney Disease (AKD/CKD)
- Urinary obstruction (cat urethral blockage, urolithiasis)
- High protein diet
- GI hemorrhage — blood in gut = protein source → elevated BUN (without proportional creatinine rise)
- Fever, hypercatabolism
- Corticosteroids (protein catabolism)
- Severe liver failure (liver can't convert ammonia to urea)
- Portosystemic shunt (blood bypasses liver)
- Low protein diet or malnutrition
- Overhydration/polyuria (urea diluted)
RFT TEST 2: CREATININE
| Species | Normal Creatinine (mg/dL) |
|---|---|
| Dog | 0.5 – 1.5 |
| Cat | 0.8 – 1.8 |
| Horse | 1.2 – 2.0 |
| Cow | 1.0 – 2.0 |
- A very muscular (large, fit) dog may have creatinine at upper normal = normal for them
- A very thin, cachexic, or muscle-wasting cat may have LOW normal creatinine even with significant kidney disease — this makes creatinine UNDERESTIMATE kidney disease in emaciated patients
- Acute Kidney Injury (AKI) — sudden kidney damage (toxins, hypotension, leptospirosis, NSAID overdose, lily toxicity in cats)
- Chronic Kidney Disease (CKD) — progressive loss of nephrons
- Urinary obstruction (post-renal)
- Dehydration (less common for creatinine to rise as much as BUN)
| IRIS Stage | Creatinine Dog (mg/dL) | Creatinine Cat (mg/dL) | Description |
|---|---|---|---|
| Stage 1 | < 1.4 | < 1.6 | Non-azotemic — early disease. Diagnosis by SDMA, USG, proteinuria |
| Stage 2 | 1.4 – 2.0 | 1.6 – 2.8 | Mild azotemia. Some signs possible |
| Stage 3 | 2.1 – 5.0 | 2.9 – 5.0 | Moderate azotemia. Clinical signs present |
| Stage 4 | > 5.0 | > 5.0 | Severe azotemia. Uremic crisis |
This staging system is critical in veterinary nephrology. Once you stage the patient, you also sub-stage by proteinuria (UPC ratio) and blood pressure.
RFT TEST 3: SDMA — Symmetric Dimethylarginine
| Species | Normal SDMA (µg/dL) |
|---|---|
| Dog | < 14 |
| Cat | < 14 |
- Not affected by muscle mass (creatinine is!) → more accurate in thin, cachexic, or elderly patients
- Rises earlier than creatinine
- Correlates better with GFR than BUN
- SDMA 14–17 µg/dL + creatinine normal → Stage 1 CKD (diagnose early!)
- SDMA ≥18 µg/dL → Stage 2+ CKD
For senior wellness screening, always run SDMA. This is the game-changer for early CKD detection, especially in cats.
RFT TEST 4: PHOSPHORUS
- CKD — most common cause in cats and dogs. Phosphorus cannot be excreted → accumulates
- Young animals post-meal (physiologic)
- Hypoparathyroidism
- Vitamin D toxicosis
- Urinary obstruction
- Calcium × Phosphorus product → if too high → calcium phosphate precipitates in soft tissues (kidneys, blood vessels, lungs)
- Promotes further kidney damage
- Causes parathyroid hyperplasia → renal secondary hyperparathyroidism → bone demineralization → "rubber jaw" in dogs
RFT TEST 5: CALCIUM
| ↑ Hypercalcemia | ↓ Hypocalcemia |
|---|---|
| Hypercalcemia of malignancy (lymphoma, anal sac carcinoma, multiple myeloma) — most common in dogs | Eclampsia (puerperal tetany) — lactating females! |
| Hyperparathyroidism (parathyroid adenoma) | Hypoparathyroidism |
| Hypervitaminosis D (rodenticide, plants like day-blooming jasmine, calcipotriol) | CKD (in some stages) |
| Granulomatous disease (fungal) | Pancreatitis (calcium binds to saponified fat) |
| Addison's disease | Hypoalbuminemia (calcium bound to albumin — pseudohypocalcemia) |
| Idiopathic hypercalcemia (cats — common, unknown cause) | Ethylene glycol toxicity (oxalate binds calcium) |
Corrected Ca (mg/dL) = Measured Ca - Albumin (g/dL) + 3.5
RFT TEST 6: ELECTROLYTES
Sodium (Na)
| ↑ Hypernatremia | ↓ Hyponatremia |
|---|---|
| Dehydration (water loss > sodium loss) | Addison's disease (hypoadrenocorticism) — the classic cause! Aldosterone deficiency → Na wasted in urine |
| Diabetes insipidus | Vomiting/diarrhea (sodium lost) |
| Inadequate water intake | Diuretics |
| Hyperaldosteronism | Congestive heart failure |
| Salt poisoning | Liver failure (ascites) |
Potassium (K)
| ↑ Hyperkalemia — DANGEROUS! | ↓ Hypokalemia |
|---|---|
| Addison's disease — most common endocrine cause (aldosterone deficiency → K retained) | Vomiting, diarrhea |
| Urinary obstruction (cat urethral blockage) — K cannot be excreted → builds up | Diuretic use (furosemide) |
| Oliguric/anuric renal failure | Anorexia, poor intake |
| Crush injury, rhabdomyolysis | Insulin treatment (drives K into cells) |
| Acidosis (K shifts out of cells) | CKD cats (hypokalemic nephropathy — important in cats!) |
| Spurious (hemolyzed sample — RBCs contain K) | Diabetic ketoacidosis (DKA) treatment |
- Cardiac effects: Bradycardia, tall T waves, wide QRS, sine wave pattern on ECG → ventricular fibrillation → cardiac arrest
- Emergency treatment: Calcium gluconate (stabilize heart), insulin + glucose (drive K into cells), sodium bicarbonate (acidosis correction), IVF, relieve obstruction
Chloride (Cl)
- Detecting metabolic acidosis/alkalosis
- Evaluating vomiting (hypochloremic metabolic alkalosis from vomiting gastric HCl)
- Addison's disease (↓ Cl follows ↓ Na)
Bicarbonate (HCO₃) / Total CO₂
- ↓ Low (Metabolic Acidosis): CKD, DKA, severe diarrhea, ethylene glycol toxicity, lactic acidosis (shock)
- ↑ High (Metabolic Alkalosis): Vomiting of gastric contents, diuretics, hyperaldosteronism
RFT TEST 7: URINALYSIS (UA) — The MOST Underused but Most Important Renal Test
How to Collect Urine (Properly!)
| Method | How | When to Use |
|---|---|---|
| Cystocentesis (gold standard) | Needle directly into bladder under USG guidance | Any time you want sterile urine for culture, cytology, sediment |
| Catheterization | Urinary catheter passed into bladder | When cystocentesis not possible, urethral obstruction |
| Free-catch (midstream) | Owner collects midstream void | Rough screening only — contaminated with external cells/bacteria |
| Table catch | Catch from patient voiding on table | Routine screening if cystocentesis not possible |
Urinalysis — Component by Component:
A. COLOR
| Color | Possible Cause |
|---|---|
| Pale yellow (normal) | Dilute urine, well-hydrated |
| Dark yellow/amber | Concentrated urine (dehydration) |
| Orange | Very concentrated, bilirubin present, some drugs |
| Red/pink | Hematuria (blood), hemoglobinuria, myoglobinuria |
| Brown/"tea-colored" | Hemoglobinuria (severe hemolysis), myoglobinuria, bilirubinuria |
| Green | Biliverdin, Pseudomonas infection |
| Milky/white | Pyuria (white cells = infection), chyluria (lymph) |
B. CLARITY / TURBIDITY
- Clear: Normal
- Cloudy: Cells (WBCs, RBCs), bacteria, crystals, lipid droplets (normal in cats)
- Flocculent: Casts, mucus, debris
C. SPECIFIC GRAVITY (USG) — The MOST Important Single Urine Test
| USG Value | Interpretation |
|---|---|
| 1.001 – 1.007 | Hyposthenuric — very dilute. Kidney diluting urine below plasma. Seen in DI, psychogenic polydipsia, post-diuretic |
| 1.008 – 1.012 | Isosthenuric — kidney NOT concentrating OR diluting. Urine same osmolality as plasma. This is CLASSIC CKD finding — kidney lost concentrating ability |
| 1.013 – 1.029 | Minimally concentrated — some concentrating ability present |
| 1.030+ (Dog) | Adequately concentrated — kidney working! |
| 1.035+ (Cat) | Adequately concentrated — kidney working! |
| > 1.040 | Very concentrated — dehydrated, or ADH working well |
Key rule: A dehydrated animal MUST have concentrated urine (USG > 1.030 dog, > 1.035 cat) to prove kidneys are working. If a dehydrated animal has USG 1.010 → kidneys are NOT responding to dehydration → renal failure.
D. pH (Urine Acidity/Alkalinity)
| pH | Meaning |
|---|---|
| Acidic (< 6.5) | Normal carnivores, fever, acidosis, protein-rich diet, starvation |
| Alkaline (> 7.5) | Urease-producing infection (Proteus, Staphylococcus → Struvite stone formation!), vegetarian diet, metabolic alkalosis, post-meal |
| Alkaline with acidosis | Renal tubular acidosis — kidneys cannot acidify urine |
E. PROTEIN (Proteinuria)
The Urine Protein:Creatinine Ratio (UPC) is the most accurate test for proteinuria.
| UPC Ratio | Interpretation |
|---|---|
| < 0.2 (dog) | Normal |
| < 0.2 (cat) | Normal |
| 0.2 – 0.5 | Borderline — recheck, investigate |
| > 0.5 | Significant proteinuria — kidney disease |
| > 1.0 | Marked proteinuria — glomerular disease, amyloidosis, glomerulonephritis |
| > 2.0 | Severe glomerular disease |
- Pre-renal: Overflow proteinuria — Bence Jones proteins (myeloma), hemoglobin (hemolysis), myoglobin (muscle damage)
- Renal:
- Glomerular proteinuria → protein leaking through damaged filter (glomerulonephritis, amyloidosis, diabetic nephropathy)
- Tubular proteinuria → tubules can't reabsorb small proteins
- Post-renal: Lower urinary tract inflammation/bleeding (UTI, cystitis, prostatitis) — protein from WBCs, RBCs
F. GLUCOSE (Glucosuria)
| Glucosuria Pattern | Cause |
|---|---|
| Glucose in urine + HIGH blood glucose | Diabetes mellitus — blood glucose exceeds renal threshold (180 mg/dL dog, 280 mg/dL cat) |
| Glucose in urine + NORMAL blood glucose | Renal glucosuria — tubular defect (Fanconi syndrome — Basenjis, other breeds!) → tubules can't reabsorb glucose despite normal blood levels |
G. KETONES
- Diabetic Ketoacidosis (DKA) — life-threatening. Insulin-deficient diabetic → fat breakdown → ketone bodies → urine
- Starvation/prolonged anorexia
- Low carbohydrate diet
- Nursing kittens/puppies
Ketonuria in a known diabetic = DKA emergency. Requires hospitalization, IV fluids, insulin, electrolyte monitoring.
H. BILIRUBIN in Urine
- ↑ Bilirubinuria in cats → always significant → liver disease or hemolysis
- ↑ Bilirubinuria in dogs (beyond trace) → hepatic or post-hepatic disease
I. UROBILINOGEN
- Present in normal urine (from bile degradation in gut → reabsorbed → excreted in urine)
- Absent → biliary obstruction (bile not reaching gut)
- Elevated → hemolysis or hepatocellular disease
J. NITRITE
- Indicates bacterial infection (gram-negative bacteria convert nitrate to nitrite)
- Used as screening test for UTI
- False negative: Gram-positive organisms (Staph, Enterococcus) don't produce nitrite
K. LEUKOCYTE ESTERASE
- Indicates white blood cells in urine = pyuria = inflammation/infection
- Must confirm with sediment examination
Urine Sediment Examination — Microscopic
RED BLOOD CELLS (RBCs) in Urine
- > 5 RBC/HPF = Hematuria
- Causes: Cystitis, urolithiasis, trauma, TCC, coagulopathy, renal disease, prostatitis
- Dysmorphic RBCs (misshapen, acanthocytic) = glomerular hematuria (squeezed through glomerular membrane)
- Normal round RBCs = lower urinary tract source
WHITE BLOOD CELLS (WBCs) in Urine
- > 5 WBC/HPF = Pyuria
- Causes: UTI, cystitis, pyelonephritis, urethritis, prostatitis
- Pyuria + bacteriuria + clinical signs = active UTI → culture + sensitivity + antibiotic treatment
CASTS — Very Important for CKD Diagnosis
| Cast Type | Appearance | Meaning |
|---|---|---|
| Hyaline casts | Pale, transparent | Mild proteinuria, fever, exercise, early renal disease |
| Granular casts | Dark, granular contents | Tubular cell degeneration — renal parenchymal disease |
| Cellular casts (RBC, WBC, epithelial) | Cells visible inside cast | Active renal inflammation — tubular necrosis, pyelonephritis |
| Waxy casts | Smooth, "waxy" appearance | Advanced chronic renal disease — very sluggish tubular flow |
| Fatty casts | Lipid droplets in cast | Diabetes, hypothyroidism, hepatic lipidosis, tubular degeneration |
| Broad casts | Wider than normal | Collecting duct = advanced CKD (dilated tubules) |
Any cellular casts = ACTIVE renal disease happening right now. Waxy/broad casts = chronic advanced disease.
BACTERIA
- Normal urine (cystocentesis sample) = STERILE = no bacteria
- Bacteria in cystocentesis sample = urinary tract infection → culture + sensitivity
- Rods usually = gram-negative (E. coli, Proteus, Pseudomonas)
- Cocci usually = gram-positive (Staphylococcus, Streptococcus, Enterococcus)
CRYSTALS
| Crystal Type | Appearance | Significance |
|---|---|---|
| Struvite (MgNH₄PO₄) | "Coffin-lid" rectangular | Alkaline urine + urease-producing bacteria → struvite stones. Very common in dogs (Cocker Spaniels, Schnauzers) and cats |
| Calcium Oxalate Dihydrate | "Envelope/Maltese cross" | Common, associated with hypercalciuria, acidic urine |
| Calcium Oxalate Monohydrate | "Hemp seed" or picket-fence | Also calcium oxalate, sometimes from oxalate toxicity (oxalic acid plants, Ethylene Glycol!) |
| Urate | Round, yellow, "thorny apple" | Dalmatians (genetic — can't process urate), portosystemic shunt (urate not metabolized), acidic urine |
| Cystine | Hexagonal, flat | Cystinuria — genetic tubular defect (Newfoundlands, Mastiffs, Dachshunds) → cystine stones |
| Calcium Phosphate (Apatite) | Amorphous/needle-like | Alkaline urine, hypercalcemia, hyperparathyroidism |
| Xanthine | Yellow-brown amorphous | Rare — allopurinol treatment side effect |
| Bilirubin crystals | Yellow needles | Bilirubinuria, hepatic disease |
| Tyrosine | Yellow needles | Severe liver disease (tyrosine not metabolized) |
RFT TEST 8: UPC RATIO — Urine Protein:Creatinine Ratio
| UPC | Status |
|---|---|
| < 0.2 | Non-proteinuric — normal |
| 0.2 – 0.5 | Borderline |
| > 0.5 | Proteinuric — CKD risk |
| > 2.0 | Severe glomerular disease |
- Non-proteinuric: UPC < 0.2
- Borderline: 0.2–0.5
- Proteinuric: > 0.5 (worse prognosis, start RAAS inhibitor — enalapril or benazepril)
RFT TEST 9: BLOOD PRESSURE
- Dog: Systolic 100–160 mmHg
- Cat: Systolic 100–150 mmHg
| Systolic BP | Risk Category | Action |
|---|---|---|
| < 140 mmHg | Minimal risk | Monitor |
| 140–159 mmHg | Low risk | Lifestyle changes |
| 160–179 mmHg | Moderate risk | Treat if persistent |
| ≥ 180 mmHg | High risk — EMERGENCY | Immediate treatment |
- CKD (most common cause in cats)
- Hyperthyroidism (cats)
- Hyperadrenocorticism (dogs)
- Pheochromocytoma (adrenal tumor)
- Diabetes mellitus
- Primary (idiopathic) hypertension
COMPLETE RFT SUMMARY TABLE
| Test | Measures | ↑ High Means | ↓ Low Means |
|---|---|---|---|
| BUN | Urea nitrogen | Dehydration, renal failure, high protein, GI bleed | Liver failure, PSS, low protein |
| Creatinine | GFR (kidney filter rate) | Renal disease (AKI/CKD), obstruction, dehydration | Muscle wasting (misleading normal!) |
| SDMA | Early GFR decline | CKD (40% loss), better than creatinine | Not significant |
| Phosphorus | Kidney excretion | CKD, obstruction, hypoparathyroidism | Malnutrition, malabsorption |
| Calcium | Parathyroid/Vitamin D/Kidneys | Malignancy, hyperparathyroidism, Vit D toxicity | Eclampsia, hypoparathyroidism, pancreatitis |
| Sodium | Fluid balance | Dehydration, DI | Addison's, vomiting, CHF |
| Potassium | Aldosterone/kidneys | Addison's, urethral obstruction, oliguric ARF | Vomiting, diarrhea, diuretics, CKD cats |
| Chloride | Acid-base | Follows Na usually | Vomiting (HCl loss) |
| Bicarbonate | Acid-base | Metabolic alkalosis (vomiting) | CKD, DKA, diarrhea, ethylene glycol |
| USG | Tubular concentrating ability | Dehydration (appropriate) | CKD, DI, Cushing's |
| Urine Protein (UPC) | Glomerular integrity | Glomerulonephritis, amyloidosis, PLN | — |
| Urine Glucose | Renal threshold/tubules | DM, Fanconi syndrome | — |
| Urine Casts | Tubular health | AKI, pyelonephritis, CKD | — |
| Blood Pressure | Cardiovascular/renal | CKD, hyperthyroidism, Cushing's | Shock, Addison's |
═══════════════════════════════════════════════
PART 3 — COMPLETE HEALTH CHECK (WELLNESS PANEL)
═══════════════════════════════════════════════
WELLNESS CHECK — COMPLETE PANEL
1. PHYSICAL EXAMINATION PARAMETERS
| Parameter | Dog Normal | Cat Normal | What to Check |
|---|---|---|---|
| Temperature | 38–39.2°C (100.5–102.5°F) | 38–39.2°C | Fever (infection, inflammation), hypothermia (shock, toxin) |
| Heart Rate | 60–180 bpm (small = faster) | 140–220 bpm | Bradycardia, tachycardia, arrhythmia |
| Respiratory Rate | 15–30 breaths/min | 20–30 breaths/min | Dyspnea, tachypnea |
| Weight / BCS | Ideal BCS = 4–5/9 | Ideal BCS = 4–5/9 | Obesity, cachexia, weight loss trend |
| Mucous Membrane Color | Pink, moist | Pink, moist | Pale (anemia), white (shock), yellow (jaundice), blue (cyanosis), brick-red (sepsis/CO) |
| CRT (Capillary Refill Time) | < 2 seconds | < 2 seconds | > 2 sec = poor perfusion/shock |
| Hydration Status | Moist mucous membranes, elastic skin | Same | Skin tent, sunken eyes, dry gums = dehydration |
| Lymph Nodes | Not palpable or small | Same | Enlarged = infection, inflammation, or neoplasia |
| Pulse Quality | Strong, regular | Strong, regular | Weak/thready = low cardiac output; bounding = fever, hyperthyroidism |
2. CBC (Complete Blood Count) — Already Covered in Full Previously
| Component | What It Tells You |
|---|---|
| WBC + Differential | Infection type (bacterial/viral/parasitic), stress |
| RBC, PCV, Hgb | Anemia or polycythemia |
| MCV, MCH, MCHC | Type of anemia (iron deficiency, regenerative, etc.) |
| Reticulocytes | Bone marrow response |
| Platelets | Bleeding risk (thrombocytopenia) |
| Blood smear | Morphology, parasites, toxic changes |
3. COMPLETE BIOCHEMISTRY PANEL (LFT + RFT + More)
THYROID HORMONE — T4 (Thyroxine)
| Species | Normal Total T4 |
|---|---|
| Dog | 1.0 – 4.0 µg/dL |
| Cat | 0.8 – 4.7 µg/dL |
- Most common endocrine disease in cats > 8 years old
- Signs: Weight loss despite good appetite, vomiting, hyperactivity, unkempt coat, PU/PD, tachycardia, heart murmur
- Often causes: High ALT, ALP, elevated BP, left ventricular hypertrophy on echo
- Treatment: Methimazole, radioactive iodine, thyroidectomy, iodine-restricted diet (Hill's Y/D)
- Most common endocrine disease in middle-aged dogs (Golden Retrievers, Labrador Retrievers, Dobermans, Boxers)
- Signs: Weight gain, lethargy, cold intolerance, bilateral symmetrical hair loss (truncal alopecia), thickening of skin (myxedema), bradycardia, high cholesterol, high triglycerides
- False low T4: Sick euthyroid syndrome (any non-thyroid illness lowers T4 → misdiagnosis)
- Better test: Free T4 by equilibrium dialysis + cTSH (canine TSH)
Important: Hypothyroid dogs have: HIGH cholesterol + HIGH triglycerides + LOW T4 + HIGH cTSH (elevated because pituitary releasing more TSH to stimulate an underperforming thyroid)
CORTISOL — Adrenal Function Tests
- Administer dexamethasone → measure cortisol at 4 and 8 hours
- Normal: Cortisol suppressed to < 1.0 µg/dL
- Cushing's: Fails to suppress → cortisol remains high
- Inject synthetic ACTH → measure cortisol at 0 and 1 hour
- Addison's: Basal low + fails to stimulate (cortisol < 2 µg/dL at both times)
- Cushing's: Exaggerated response (> 22 µg/dL post-ACTH)
- Iatrogenic Cushing's: Basal and post-ACTH both LOW (exogenous steroids suppress adrenal)
PANCREATIC TESTS
- Gold standard blood test for pancreatitis in dogs and cats
- Normal Spec cPL: < 200 µg/L (dog)
- Normal Spec fPL: < 3.5 µg/L (cat)
- Elevated in pancreatitis, pancreatic neoplasia
- Less specific than lipase (also made by intestine, salivary glands)
- Still used as supporting test: elevated in pancreatitis, intestinal disease, renal failure (reduced clearance)
- Normal dog: 200–2000 U/L
- The gold standard test for Exocrine Pancreatic Insufficiency (EPI)
- Normal dog: 5–35 µg/L
- EPI: TLI < 2.5 µg/L — pancreas not making digestive enzymes → maldigestion, voluminous pale greasy feces, weight loss despite ravenous appetite
- Common in German Shepherds (genetic), also young Rough Collies
COBALAMIN (Vitamin B12) and FOLATE
| Parameter | Normal (Dog) | Normal (Cat) | Significance |
|---|---|---|---|
| Cobalamin (B12) | 200–900 ng/L | 200–1400 ng/L | Low = ileal malabsorption, EPI, intestinal disease, dysbiosis |
| Folate | 7–25 µg/L | 7–24 µg/L | Low = proximal intestinal disease (duodenum/jejunum), IBD; High = small intestinal bacterial overgrowth (SIBO), EPI |
- Low B12 + High Folate = bacterial overgrowth (bacteria consume B12, produce excess folate)
- Low B12 + Low Folate = diffuse intestinal disease, severe IBD, lymphoma
- Low B12 alone = ileal disease, EPI (ileum absorbs B12)
- Low Folate alone = proximal small intestinal disease (IBD, lymphoma in duodenum/jejunum)
URINE CULTURE AND SENSITIVITY (C&S)
- Bacterial colony counts
- Organism identification
- MIC (Minimum Inhibitory Concentration) for multiple antibiotics
FECAL EXAMINATION
| Test | What It Detects |
|---|---|
| Fecal flotation (zinc sulfate, sodium nitrate) | Eggs: Roundworm (Toxocara), Hookworm (Ancylostoma), Whipworm (Trichuris), Tapeworm (Dipylidium, Taenia), Coccidia (Isospora), Giardia |
| Fecal direct smear | Motile Giardia trophozoites, Tritrichomonas in cats, fresh eggs |
| Fecal Baermann | Lungworm larvae (Aelurostrongylus in cats, Angiostrongylus in dogs) |
| Giardia ELISA / SNAP test | Giardia antigen — more sensitive than flotation |
| Fecal PCR panel | Campylobacter, Salmonella, Clostridium, Cryptosporidium, Giardia, parvovirus, coronavirus |
| Fecal occult blood | Blood in feces (GI hemorrhage) — detects non-visible blood |
4. HEARTWORM TEST
| Species | Test | When |
|---|---|---|
| Dog | Heartworm antigen test (detects female worm antigen) | Annually or before starting prevention |
| Cat | Heartworm antigen + antibody test (combined) | Antibody = exposure, antigen = active infection |
5. BLOOD PRESSURE MEASUREMENT
- Every visit for cats > 7 years old
- Every visit for dogs with CKD, Cushing's, diabetes, cardiac disease
- Annual check for all dogs > 7 years
6. SENIOR WELLNESS PANEL — AGE-BY-AGE GUIDE
| Age | Species | Recommended Tests |
|---|---|---|
| 6 weeks | Dog/Cat | Physical exam, fecal, deworming, first vaccination |
| 8–16 weeks | Dog/Cat | Vaccination series, fecal, parvovirus screening |
| 6 months | Dog/Cat | Pre-neuter/spay bloodwork (CBC + basic chemistry) |
| 1 year | Dog/Cat | Annual exam, vaccines, heartworm test (dog), fecal |
| 3–6 years | Dog/Cat | Annual exam, CBC + biochemistry + urinalysis baseline |
| 7 years (SENIOR) | Dog | Full panel: CBC + chemistry + UA + T4 + BP + fecal + heartworm every 6–12 months |
| 7 years (SENIOR) | Cat | Full panel: CBC + chemistry + T4 + UA + BP + SDMA every 6 months |
| 10+ years (GERIATRIC) | Dog | All senior tests + Echo (if murmur) + Chest X-ray + BP every 6 months |
| 10+ years (GERIATRIC) | Cat | All senior + T4 + SDMA + UPC + BP every 6 months. Free T4 if borderline T4 |
7. VACCINATION STATUS CHECK
| Vaccine | Core or Non-core | Species | Schedule |
|---|---|---|---|
| Parvovirus | Core | Dog | Puppy series → 1 year → every 3 years |
| Distemper | Core | Dog | Same as parvovirus (usually combined = DHPP) |
| Adenovirus (Hepatitis) | Core | Dog | Part of DHPP |
| Parainfluenza | Core/Non-core | Dog | Part of DHPP |
| Rabies | Core (legally required) | Dog + Cat | 1 year, then every 1–3 years per local law |
| Feline Herpesvirus (FHV-1) | Core | Cat | Kitten series → boosters (FVRCP) |
| Feline Calicivirus (FCV) | Core | Cat | Part of FVRCP |
| Feline Panleukopenia (FPL) | Core | Cat | Part of FVRCP |
| FeLV | Non-core (core for outdoor cats) | Cat | Kitten + booster, then annually for outdoor cats |
| Bordetella | Non-core | Dog | Before boarding/kenneling, yearly or semi-annual |
| Leptospirosis | Non-core (core in endemic areas) | Dog | Annual in flood-prone areas, farms, rural dogs |
| Lyme (Borrelia) | Non-core | Dog | Endemic areas, tick-exposed dogs |
| Canine Influenza | Non-core | Dog | Boarding/show dogs |
8. DEWORMING AND PARASITE CONTROL
| Parasite | Treatment | Schedule |
|---|---|---|
| Roundworm | Pyrantel, fenbendazole, milbemycin | Puppies/kittens: every 2 weeks until 12 weeks, then monthly until 6 months. Adults: every 3 months or annual fecal |
| Hookworm | Pyrantel, fenbendazole, milbemycin | Same as roundworm |
| Whipworm | Fenbendazole (5-day course), milbemycin | Dogs only. Treat, then recheck fecal in 3–4 months |
| Tapeworm | Praziquantel, epsiprantel | After fecal confirmation or flea infestation |
| Giardia | Metronidazole, fenbendazole | Treat + environmental decontamination |
| Coccidia | Ponazuril, sulfadimethoxine | Young animals especially |
| Heartworm prevention | Monthly: milbemycin oxime, ivermectin, selamectin | Year-round in tropical/subtropical climates |
| Flea/Tick prevention | Isoxazolines (fluralaner, sarolaner), spinosad, selamectin | Monthly or quarterly depending on product |
| Ear mites | Selamectin, ivermectin, milbemycin | Treat all contact animals simultaneously |
9. NUTRITIONAL ASSESSMENT
| Parameter | Checked By | Significance |
|---|---|---|
| Body Condition Score (BCS) | Physical exam (1–9 scale) | 4–5 = ideal. < 3 = underweight. > 7 = obese |
| Muscle Condition Score (MCS) | Palpation over spine, scapulae, skull | Normal, mild/moderate/severe muscle wasting. Muscle loss happens in CKD, cancer, EPI |
| Diet history | Owner interview | Treats, human food, supplements — often reveals cause of obesity, renal phosphorus excess, pancreatitis triggers |
| Water intake | Owner report | Polydipsia (> 90 mL/kg/day dog, > 45 mL/kg/day cat) = investigate DM, Cushing's, DI, CKD, hyperthyroidism |
COMPLETE HEALTH CHECK — SUMMARY SHEET
FULL HEALTH CHECK = ALL OF THE FOLLOWING:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
PHYSICAL EXAM:
☐ Temperature, HR, RR, weight, BCS, MCS
☐ MM color, CRT, hydration
☐ Lymph node palpation
☐ Auscultation (heart murmur? arrhythmia? lung sounds?)
☐ Abdominal palpation (organ size? masses? pain?)
☐ Ophthalmic + ear + skin + oral exam
☐ Orthopedic assessment (joint pain? gait abnormalities?)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
BLOODWORK:
CBC: WBC differential, RBC, PCV, Hgb, MCV, MCH, MCHC, Platelets, Reticulocytes
LFT: ALT, AST, ALP, GGT, Total Bilirubin (Direct + Indirect), Bile Acids (fast + post-prandial), Albumin, Total Protein, Globulins, Cholesterol, Glucose, PT/aPTT (if needed), Ammonia (if encephalopathy suspected)
RFT: BUN, Creatinine, SDMA, Phosphorus, Calcium, Sodium, Potassium, Chloride, Bicarbonate
ADDITIONAL: T4, Spec cPL/fPL (if GI signs), TLI (if EPI suspected), Cortisol/LDDS/ACTH (if endocrine disease suspected), Cobalamin + Folate (if chronic GI disease)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
URINALYSIS:
☐ Color, Clarity
☐ USG, pH, Protein (+ UPC if proteinuric), Glucose, Ketones, Bilirubin, Urobilinogen, Nitrite, Leukocyte Esterase
☐ Sediment: RBCs, WBCs, Casts, Bacteria, Crystals, Epithelial cells
☐ Culture + Sensitivity if pyuria/bacteriuria present
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
FECAL:
☐ Flotation, direct smear, Giardia ELISA (routine)
☐ Baermann (if lungworm suspected)
☐ PCR panel (if diarrhea or systemic illness)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
IMAGING (AS INDICATED):
☐ Thoracic radiographs (cardiac disease, respiratory signs)
☐ Abdominal USG (liver, spleen, kidneys, adrenals, bladder, GIT)
☐ Echocardiography (heart murmur, cardiomegaly on X-ray)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
PREVENTIVE:
☐ Vaccination status review + update
☐ Heartworm test + prevention status
☐ Flea/tick prevention status
☐ Deworming schedule
☐ Blood pressure (all cats > 7y, senior dogs, CKD/hypertension patients)
☐ Dental assessment (periodontal disease grading)
☐ Nutritional counseling (BCS, diet review)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
QUICK CLINICAL DECISION GUIDE
When you see HIGH ALT in a dog:
When you see HIGH ALP in a cat:
When you see HIGH BUN but NORMAL Creatinine:
When you see HIGH BUN AND HIGH Creatinine together:
When USG is fixed at 1.010 in a sick pet:
Cat with weight loss + polyphagia + tachycardia:
Dog with PU/PD + pot belly + thin skin + muscle wasting + hair loss:
Dog with PU/PD + low Na + high K + Na:K < 27:1 + Low BCS:
Sources: Henry's Clinical Diagnosis & Management by Laboratory Methods | Washington Manual of Medical Therapeutics | Robbins & Kumar Basic Pathology | Quick Compendium of Clinical Pathology 5e | Tietz Textbook of Laboratory Medicine 7e | Barash Clinical Anesthesia 9e | Morgan & Mikhail's Clinical Anesthesiology 7e | Brenner & Rector's The Kidney | Applied Veterinary Clinical Knowledge (species-specific reference ranges and interpretations)
Ab mujay feline herpes virud ka bara ma tamam tar details jitni b hai vet sources reserch articles or apni knowledge use karka tamam tar information baj do ak b point miss na ho or 100 accurate ho . English ma details batayen