All images are now in hand. Here is the complete, detailed, fully illustrated section on secondary suturing of burst abdomen:
Secondary Suturing of Burst Abdomen - Detailed Account
1. DEFINITION
Burst abdomen (acute abdominal wound dehiscence / abdominal wound disruption) is the postoperative separation of the musculo-aponeurotic layers of a laparotomy wound. It ranges from partial (superficial, skin-only) to complete dehiscence with evisceration - protrusion of abdominal viscera (bowel or omentum) through the disrupted incision.
"Significant wound dehiscence occurs in approximately 1% of all laparotomies. In patients with malignant disease or other serious illness, the incidence may be much greater."
-- Sabiston Textbook of Surgery 21e
2. ANATOMY OF THE ABDOMINAL WALL (Why It Bursts)
Understanding the layers is critical to the repair. A midline laparotomy incision disrupts these layers from outside in:
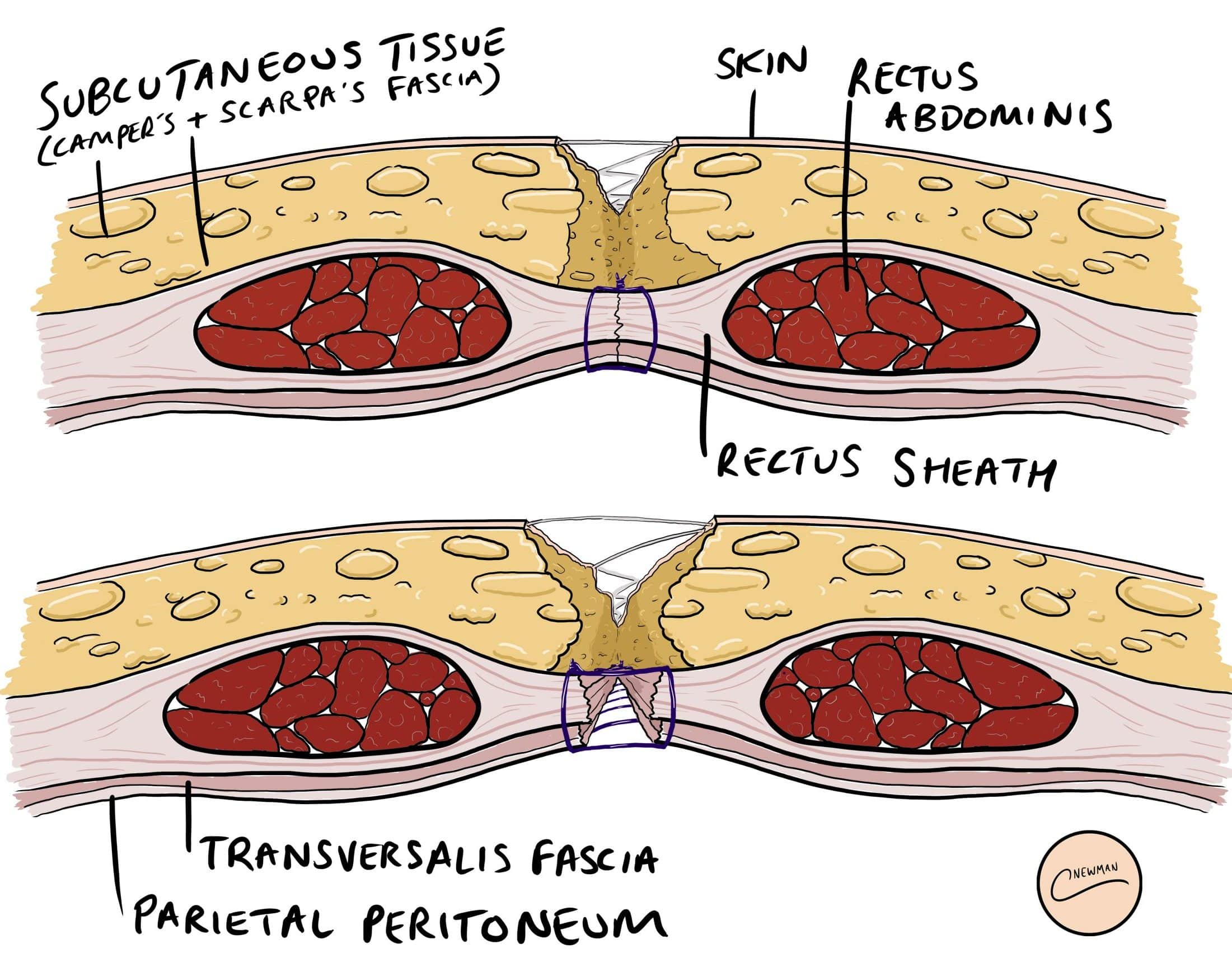
Abdominal wall cross-section: Skin → Subcutaneous tissue (Camper's + Scarpa's fascia) → Anterior rectus sheath → Rectus abdominis → Posterior rectus sheath → Transversalis fascia → Parietal peritoneum
In burst abdomen, it is the fascial layer (rectus sheath / linea alba) that is the critical failure point. When fascia gives way, nothing prevents evisceration.
3. INCIDENCE AND TIMING
- Overall incidence: ~1% of all laparotomies (up to 10-15% in high-risk patients)
- Typical timing: Day 5-10 post-surgery (peak Day 7-8)
- At this time wound tensile strength is only 7-60% of native bursting pressure - the wound is at its most vulnerable while still healing
4. PREDISPOSING FACTORS
Patient (Systemic) Factors
| Factor | Mechanism |
|---|
| Malnutrition / Hypoproteinaemia | Impaired collagen synthesis and wound healing |
| Anaemia | Reduced oxygen delivery to healing wound |
| Obesity | Excess intra-abdominal pressure, poor tissue vascularity |
| Diabetes mellitus | Impaired neutrophil function, delayed healing |
| Corticosteroid use | Suppresses fibroplasia and collagen cross-linking |
| Malignancy | Cachexia + immune compromise |
| Jaundice | Impaired collagen synthesis, endotoxaemia |
| Uraemia | Impaired platelet function and healing |
| Immunosuppression | Reduced wound defence |
Local / Technical Factors
| Factor | Mechanism |
|---|
| Wound infection / SSI | Collagenase-mediated collagen breakdown |
| Haematoma / Seroma | Acts as culture medium + prevents apposition |
| Poor technique | Inadequate fascial bites, excessive tension, wrong suture |
| Wrong suture material | Fast-absorbing suture loses strength before fascia heals |
| Dead space | Increases fluid collection and infection risk |
Postoperative Factors
| Factor | Mechanism |
|---|
| Ileus / Abdominal distension | Increases intra-abdominal pressure on suture line |
| Persistent coughing (chronic lung disease) | Repeated stress on wound |
| Vomiting | Sudden spikes in intra-abdominal pressure |
| Inadequate analgesia | Reflex muscle spasm and coughing |
5. PATHOPHYSIOLOGY
During the first 1-2 weeks post-surgery:
- Wound tensile strength is only 7-10% of normal
- At 5 weeks: ~60% of normal
- After 1 month: dehiscence from normal activity becomes unlikely
The critical window is Days 5-10: enough time for infection to set in and degrade collagen, but wound not yet strong enough to resist the forces of postoperative ileus and patient activity.
6. CLINICAL PRESENTATION
Warning Sign (Premonitory Sign)
- Sudden increase in serous, pink or serosanguinous wound drainage - the so-called "salmon-pink fluid"
- This must be treated as deep fascial dehiscence until proven otherwise
- Occurs 24-48 hours before visible dehiscence in ~50% of cases
Grades of Dehiscence
| Grade | Features |
|---|
| Superficial | Skin and subcutaneous tissue open; rectus sheath intact; no evisceration |
| Deep (fascial) | Rectus sheath disrupted; new wound bulging; heavy serosanguinous discharge |
| Complete / Burst abdomen | Full-thickness disruption; omentum or bowel visibly protrudes through wound |
7. IMMEDIATE MANAGEMENT (Pre-Theatre)
This is a surgical emergency. Take these steps immediately on the ward:
1. CALL the surgical team and anaesthesia immediately
2. A-E assessment and resuscitation
3. IV access + IV fluid resuscitation
4. IV broad-spectrum antibiotics (e.g. piperacillin-tazobactam)
5. Adequate IV analgesia (reduces straining)
6. Cover the wound:
- Moist (saline-soaked) gauze over the wound AND any protruding viscera
- NEVER dry gauze directly on exposed bowel — it erodes into bowel lumen, causing fistula
- Petroleum jelly gauze is preferred for exposed bowel
7. Do NOT attempt to reduce eviscerated bowel on the ward
8. Urgent transfer to operating theatre — patient supine, knees slightly bent to relax abdominal wall
9. NBM (nil by mouth)
10. Mark for stoma if likely required
8. OPERATIVE MANAGEMENT - SECONDARY SUTURING (STEP BY STEP)
Setting: Operating theatre, general anaesthesia. Cannot be done adequately under local or spinal.
PRE-OPERATIVE PLANNING
Before operating, assess:
- Is there gross intra-abdominal sepsis or feculent discharge? (Will need full exploration + washout, possibly ostomy)
- Is fascial closure technically feasible? (Is there loss of domain? Is there ischemic/necrotic fascia?)
- What are the patient's risk factors for re-dehiscence? (Guides use of retention sutures)
STEP 1: OPEN THE WOUND AND ASSESS FASCIA
- Open all of the skin incision fully (not just the visibly dehisced segment)
- Carefully inspect the entire fascial closure from one end to the other
- Locate where the previous fascial suture is intact and trace back from the dehisced area
- Debride all necrotic/devitalised tissue at the fascial edges until clean, viable fascia is reached
- This step is essential - closing over dead tissue guarantees re-dehiscence
STEP 2: ABDOMINAL EXPLORATION AND LAVAGE
- Gently examine intra-abdominal contents:
- Clear serous fluid → limited, gentle exploration; avoid iatrogenic bowel injury
- Purulent discharge → search for undrained collections and address
- Feculent/bilious fluid → enterocutaneous fistula suspected → extensive washout + repair/diversion
- Apply gentle downward pressure on bowel for limited visualization
- Lavage the peritoneal cavity with warm saline (1-3 litres)
- If in doubt, do not over-explore - the priority is closure, not comprehensive exploration
STEP 3: PLACE RETENTION SUTURES (BEFORE FASCIAL CLOSURE)
This is the key distinguishing step in secondary suturing of burst abdomen.
Purpose of retention sutures:
- They do NOT prevent fascial dehiscence
- They DO prevent evisceration if the fascial closure fails again
- They distribute tension over a wide area of the abdominal wall, sparing the suture line
Technique:
Line diagram: Retention suture passing full-thickness through skin → subcutaneous fat → anterior rectus sheath → rectus muscle → posterior sheath (extraperitoneal) with rubber catheter bolster on skin surface. Note the interrupted PDS sutures closing the fascia separately.
Placement details:
- Suture material: No. 1 or No. 2 heavy non-absorbable - nylon, polypropylene, or braided (e.g. nylon, PDS No. 1/2)
- Position: 3-4 cm from the fascial edge, on both sides of the wound
- Spacing: 4-6 cm apart from each other along the wound length
- Depth: Full-thickness passing through: skin → subcutaneous fat → anterior rectus sheath → rectus muscle → ideally extraperitoneal (posterior sheath, preperitoneal space) - avoiding intraperitoneal placement to prevent visceral entrapment
- Visualise the needle at all times - place a malleable retractor under the fascia to protect bowel
- Do NOT tie the retention sutures yet - leave them long and marked; they are tied after fascial closure is complete
Types of retention sutures:
Types of retention/through-and-through sutures: (A) Simple interrupted, (B) Horizontal mattress, (C) Figure-of-eight, (D) With external bolster - showing different configurations used in clinical practice
STEP 4: CLOSE THE FASCIA (MASS CLOSURE / INTERRUPTED)
This is the definitive repair.
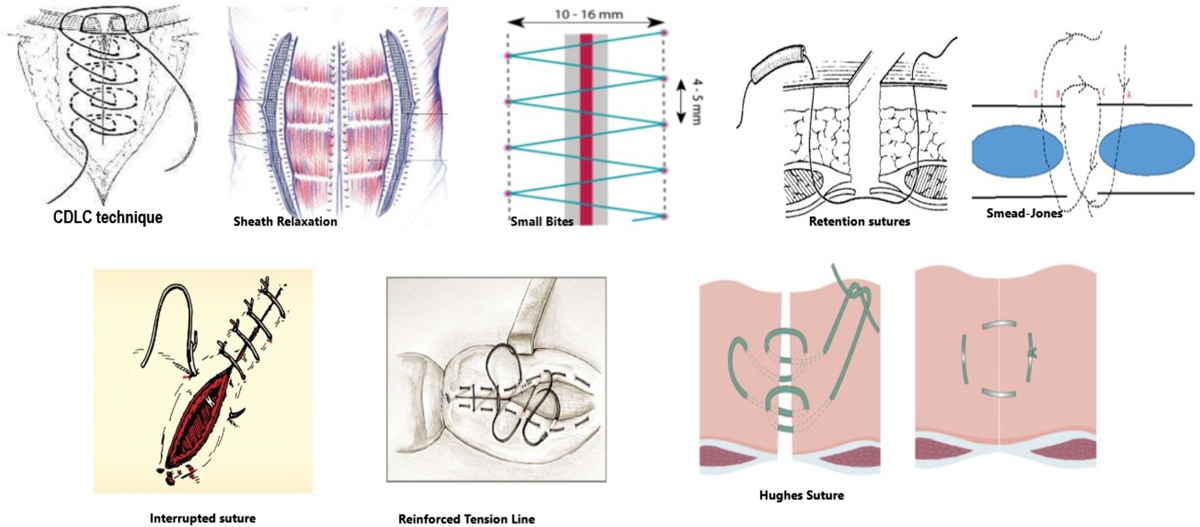
Overview of abdominal closure techniques - from standard interrupted to small-bites technique to retention/Smead-Jones configurations
Preferred technique for secondary closure:
- Interrupted mass closure is preferred over continuous suture for secondary closure
- A meta-analysis (Gupta et al., 23 studies, N=10,900) showed interrupted closure was associated with significantly less dehiscence than continuous closure
- A 2019 RCT (Bansiwal et al., 300 patients) showed burst abdomen rate of 20.1% with continuous vs. 5.4% with interrupted (p<0.05) in emergency laparotomy
- With continuous closure, a single stitch failure or area of fascial necrosis opens the entire wound; with interrupted, only that segment fails
Suture material of choice:
- Polydioxanone (PDS) No. 1 - preferred (monofilament, resists infection, retains tensile strength for 40-90 days - matches fascial healing timeline)
- Alternatively: Polyglyconate (Maxon), polypropylene, or nylon
- Avoid fast-absorbing sutures (polyglactin alone) - insufficient tensile strength duration for fascial healing (half-life only 3 weeks); associated with higher dehiscence rates (52% vs. 16% with PDS in one study)
- Barbed sutures (if available): provide even tension distribution without knots
Technical principles:
- Start with sutures at each end of the wound then meet in the middle (distributes tension)
- Take adequate fascial bites - not too shallow (won't hold) and not excessively deep (excess tension + ischaemia)
- Elective recommendation: small bites (5mm tissue, 5mm apart) - associated with lower incisional hernia rates
- Emergency/re-closure: larger bites acceptable to secure repair
- Maintain direct visualization throughout - malleable retractor protecting bowel under fascia
- Do NOT close the peritoneum separately - no benefit and adds operating time
STEP 5: TIE RETENTION SUTURES OVER BOLSTERS
Now tie the retention sutures that were placed in Step 3, but only after fascial closure is complete.
- Thread each retention suture through a bolster before tying:
- Options: Red rubber catheter segments (most commonly used, as shown in textbook image), sterile IV tubing strips, plastic bridges, or commercial retention bridges
- Bolsters distribute the tension over a wider skin area, preventing the heavy suture from cutting through the skin (cheese-wiring effect)
- Tie without excessive tension - the aim is to reduce wound strain, not strangulate tissue
- Avoid pulling too tightly - sutures will dimple the skin and cause pressure necrosis
STEP 6: SKIN CLOSURE
- Close skin loosely - do not aim for tight skin apposition
- Options:
- Loose interrupted skin sutures or staples - allow drainage
- Delayed primary closure (Day 4-5) if contaminated - leave skin open initially, pack with wet dressings, close when wound is clean and granulating
- Leave skin open in gross contamination or infection - heal by secondary intention or vacuum-assisted closure (VAC therapy)
9. THE FOUR-STEP PROCESS - ILLUSTRATED SUMMARY
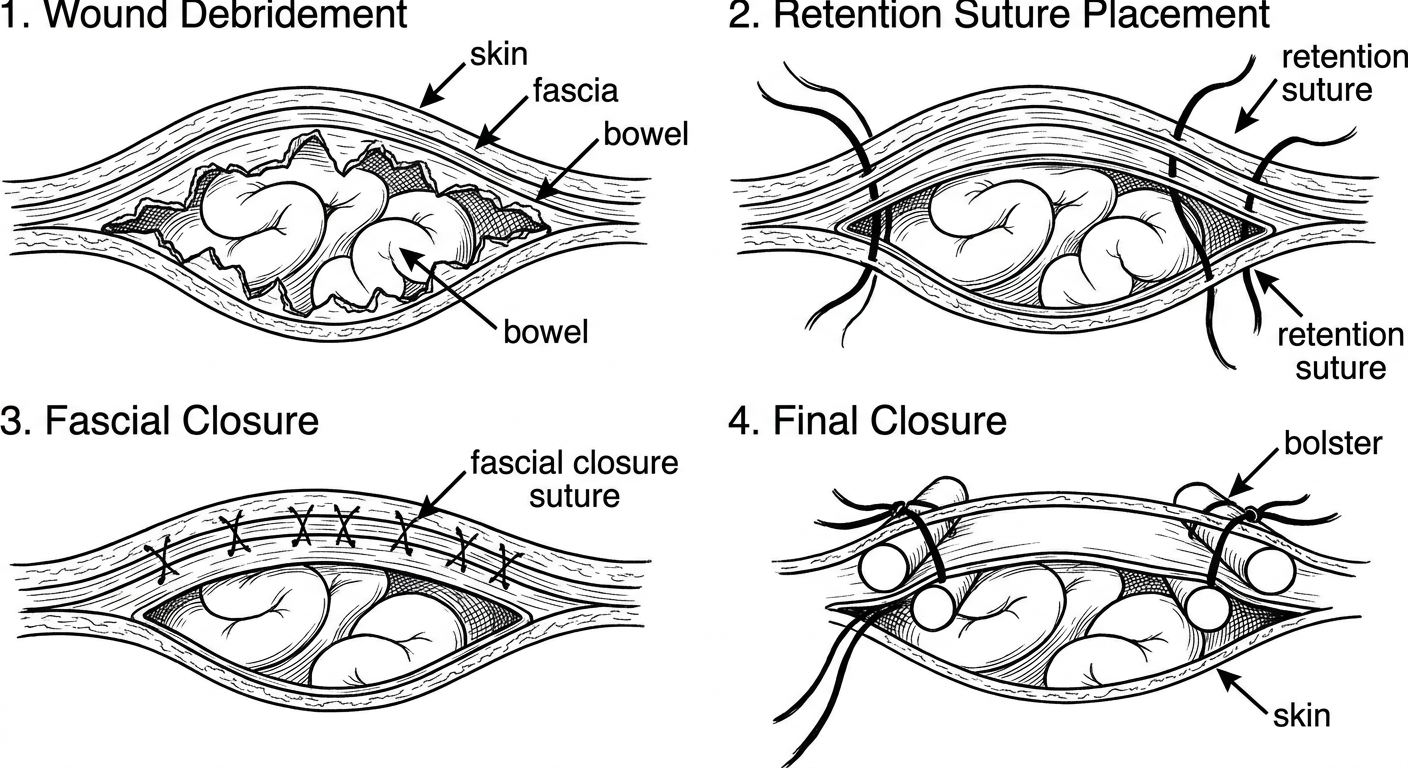
Step-by-step line diagram of secondary suturing of burst abdomen:
1. Wound debridement - fascial edges cleared, bowel visible
2. Retention sutures placed full-thickness through all layers, NOT yet tied
3. Fascial closure with interrupted PDS/mass closure sutures
4. Retention sutures tied over bolsters, skin loosely approximated
10. CLINICAL PHOTOGRAPH - INTRAOPERATIVE
Left: Intraoperative view - fascial closure in progress with long heavy retention sutures passed through all layers lateral to the wound, awaiting tying. Right: Postoperative view - retention sutures tied down over red rubber catheter bolsters, distributing pressure over the skin surface.
(Source: Current Surgical Therapy 14e, Fig. 8)
11. COMPLETE FASCIAL DEHISCENCE - APPEARANCE
Complete fascial dehiscence after partial failure of a continuous running primary abdominal closure - exactly the scenario that requires secondary suturing. Note the exposed bowel and completely disrupted fascia.
(Source: Current Surgical Therapy 14e, Fig. 7)
12. SPECIAL SCENARIOS AND MODIFICATIONS
When Primary Re-closure is NOT Possible
| Situation | Management |
|---|
| Gross abdominal sepsis / necrotizing fasciitis of abdominal wall | Open abdomen management - negative pressure wound therapy (wound VAC/Barker pack) |
| Loss of domain (fascial edges cannot be approximated without tension) | Bridging mesh repair (biological or synthetic) + possible component separation |
| Bowel edema preventing closure | Bogota bag (sterile IV fluid bag used as temporary silo) or wound VAC |
| Enterocutaneous fistula | Resuscitate → CT scan → operative washout → repair/diversion (ileostomy or colostomy) |
| Colostomy adjacent to wound | Place retention sutures closer to midline; preserve 3 cm of flat skin around stoma; avoid pulling sutures tight near stoma |
| Superficial dehiscence only (fascia intact) | Abdominal binder + wound packing; OR secondary closure after 4-5 days granulation |
13. POSTOPERATIVE CARE
| Measure | Detail |
|---|
| Nutrition | High-protein diet + multivitamins immediately postoperatively; albumin infusion if severely hypoalbuminaemic |
| Retention suture duration | Leave in for 6-8 weeks minimum; remove only after skin wound is well healed for 3-4 weeks |
| Patient counselling | Warn about discomfort from retention sutures - common complaint |
| Abdominal binder | Continued support during recovery |
| Antibiotics | Complete course for wound infection if present |
| Monitor for complications | Re-dehiscence, seroma, wound infection, pressure necrosis under bolsters |
14. COMPLICATIONS OF RETENTION SUTURES
| Complication | Mechanism | Prevention |
|---|
| Skin pressure necrosis | Heavy suture cutting through skin | Bolsters (rubber catheter/IV tubing) |
| Pain / discomfort | Constant tension on skin | Adequate analgesia; avoid over-tightening |
| Wound complications | Suture-skin interface inflammation | Wound hygiene; timely removal |
| Bowel trapping (if intraperitoneal) | Suture loops around viscera | Keep sutures extraperitoneal (preperitoneal space) |
| Difficulty with stoma appliance | Sutures near stoma site | Place sutures 3 cm from stoma edge |
15. PREVENTION OF BURST ABDOMEN (PRIMARY)
Preventing the condition is better than treating it.
- Use slow-absorbing monofilament suture for fascial closure (PDS No. 1 preferred over polyglactin in high-risk patients)
- Mass closure technique for fascial repair; interrupted preferred in emergency settings
- Small-bites technique (5 mm bites, 5 mm apart) in elective cases - reduces hernia rate
- Barbed sutures - even tension distribution, no knot as nidus for infection
- Optimise nutrition preoperatively
- Control blood glucose perioperatively
- Correct anaemia
- Use prophylactic retention sutures in selected very high-risk patients (though not routinely advocated due to complications)
16. OUTCOME DATA
| Management | Mean Healing Time |
|---|
| Secondary intention (conservative dressings only) | 61.2 ± 35.8 days |
| Secondary re-closure (after 4 days granulation) | 17.6 ± 7.2 days |
| Debridement + immediate re-closure | ~20 days (median) |
(Dodson et al., prospective study, p<0.001)
Secondary re-closure is consistently superior to conservative management in terms of healing time, outpatient visits, duration of disability, and cost.
(Sources: Sabiston Textbook of Surgery 21e, p. 718; Current Surgical Therapy 14e, p. 1422-1423; VUMC Global Surgical Atlas - Closure of Laparotomy Wound Dehiscence; StatPearls - Wound Dehiscence; TeachMeSurgery; Gupta meta-analysis 2008; Bansiwal et al. 2019)