Here is the complete illustrated OBG instruments guide for your table viva. Images are embedded where available; Wikipedia/Wikimedia links open directly as clinical reference photos.
OBG Instruments with Clinical Images - Table Viva (MBBS)
1. Cusco's Bivalve Self-Retaining Speculum
Description: Two-bladed, duck-bill shaped, self-retaining (no assistant needed). Patient in dorsal lithotomy position.
Uses:
- Visualize cervix and vaginal fornices (routine P/V exam)
- Pap smear / cervical cytology
- Detect APH local cause (polyp, ectopy, Ca cervix)
- Detect PROM (liquor leaking from os)
- Colposcopy, cervical biopsy, IUCD insertion/removal
Key viva point: Self-retaining = no assistant required. 2 blades open anteroposteriorly.
2. Sim's Double-Bladed Posterior Vaginal Speculum
Description: Two unequal blades (narrow for nulliparous, wide for parous), not self-retaining - held by assistant. Patient in Sim's (left lateral) position.
Uses:
- Retract posterior vaginal wall for surgical procedures
- Inspect cervix/vagina for injury after delivery
- Clean vagina post-delivery
- D&C, D&E, repair of perineal tears
- Exclude local APH cause
Key viva point: NOT self-retaining, needs assistant to hold. Sims' position = left lateral decubitus.
3. Hegar's Cervical Dilators
Description: Set of graduated, curved, metallic, blunt-ended rods. Sizes 1-20 (each number = diameter in mm). Used in pairs (double-ended, each end a consecutive size).
Uses:
- Cervical dilatation before D&C, D&E
- Suction evacuation (MTP)
- Hysteroscopy
- Primary dysmenorrhea (cervical stenosis)
- Fothergill's operation (Manchester repair)
Key viva point: Serial dilatation done - start small, go up gradually. Can cause uterine perforation if force used. Hawkin-Ambler's dilator is better (has a holder, fewer injuries).
4. Teale's Vulsellum Forceps
Description: Long scissors-like forceps with multiple teeth (2 × 3 teeth) at tip. Has a ratchet lock.
Uses:
- Grasp anterior cervical lip for D&C, suction evacuation
- Grasp posterior cervical lip for colpotomy, colpocentesis (access to POD)
- Hold cervix for cervical biopsy, amputation, electrocautery, cryocautery
- Encerclage (though ring forceps preferred)
Key viva point: "2 × 3" teeth = better grip but more trauma. Allis forceps used instead in obstetrics (less traumatic to soft vascular cervix).
5. Simpson's Uterine Sound
Description: Thin, malleable, graduated silver/stainless steel probe with a rounded tip. Markings at 1 cm intervals.
Uses:
- Measure length of uterine cavity (normal 6-8 cm)
- Determine position of uterus (anteverted vs retroverted)
- Check patency of internal os
- Before IUCD insertion to determine cavity size/direction
Key viva point: Normal uterine cavity = 6-8 cm (up to 10 cm in multiparous). Can cause uterine perforation if excess force used.
6. Sponge Holding Forceps (Ring Forceps)
Description: Circular rings at tip (fenestrated ovoid ends), ratchet lock, long handles.
Uses:
- Swabbing with betadine/antiseptic solution pre-op (abdomen, vulva, vagina)
- Apply pressure for hemostasis
- Blunt dissection
- Clean uterine cavity after C-section delivery
- Examine cervix for tears after delivery
- Hold cervix for encerclage
- Remove cervical polyps
Key viva point: Has a ratchet lock. Distinguished from Haywood Smith's ovum forceps by the lock.
7. Haywood Smith's Ovum Forceps
Description: Identical appearance to ring forceps but has NO ratchet lock. Blades are cupped/concave.
Uses:
- Evacuate products of conception (POC) in surgical MTP
- Evacuation of incomplete/missed abortion (RPOC)
- Gentle grasping to avoid crushing tissue
Key viva point: NO lock = key distinguishing feature from sponge holding forceps.
8. Blake's Sharp Uterine Curette
Description: Thin handle with a spoon-shaped sharp loop at end. Various sizes.
Uses:
- Endometrial curettage (D&C)
- MTP evacuation
- Incomplete abortion (RPOC)
- Endometrial sampling for abnormal uterine bleeding
- Hydatidiform mole evacuation
Key viva point: Sharp curette used in D&C. Flushing curette is BLUNT - used in D&E to flush uterine cavity. Randall's/Pipelle = flexible, outpatient endometrial biopsy without anesthesia.
9. Obstetric Forceps (Anderson's / Long Curved)
Description: Two separate crossing blades. Each blade has: blade (tip, fenestrated body) - shank - lock - handle. Two curves: cephalic curve (fits baby's head) + pelvic curve (fits birth canal).
Types:
| Forceps | Feature | Use |
|---|
| Anderson's (Long curved) | Standard, English lock | Low/outlet forceps delivery |
| Wrigley's | Short blades | Outlet forceps, C-section (impacted head) |
| Kjelland's | Minimal pelvic curve, sliding lock | Rotation (deep transverse arrest, face presentation) |
| Neville-Barnes | Axis traction device | Low/mid forceps with axis traction |
ACOG Classification:
- Outlet: Scalp visible at introitus, rotation ≤45°
- Low: Station +2 or below
- Mid: Engaged but above +2 station
Key viva point: "Never apply forceps to an unengaged head." Complications: maternal lacerations, neonatal facial nerve palsy, cephalhematoma, subgaleal hemorrhage.
10. Ventouse / Vacuum Extractor
Description: Suction cup (metal Malmstrom or silastic/plastic) connected to vacuum pump via tube. Applied to fetal scalp. Suction built to 0.8 kg/cm² (80 kPa) over 2-8 minutes.
Scalp swelling formed = CHIGNON (caput succedaneum-like, disappears within 24-48 hrs)
Advantages over forceps: Less maternal trauma, less anesthesia needed, easier to learn, self-detaches if excessive traction.
Contraindications:
- Preterm (<34 weeks) - fragile fetal skull
- Face presentation
- Fetal bleeding disorders (thrombocytopenia, hemophilia)
- After fetal blood sampling
- Unengaged head
Key viva point: Sequential use (vacuum then forceps) dramatically increases intracranial hemorrhage risk (7.4× vs spontaneous) - avoid.
11. Episiotomy Scissors
Description: Angled/bent scissors. One blunt-tipped blade (placed in vagina), one sharp blade outside.
Types:
- Mediolateral episiotomy - preferred in India (45° angle from midline) - less risk of 3rd/4th degree tear
- Midline/median - easier to repair, heals better, but higher risk of extension to anal sphincter
Key viva point: Timing: cut at crowning, at peak of contraction. Routine episiotomy no longer recommended - only selective.
12. Doyen's Retractor
Description: Curved, wide, flat blade with a handle. Bladder retractor.
Uses:
- Retract abdominal wall and bladder during LSCS (Lower Segment Cesarean Section)
- Essential for exposure of the lower uterine segment
- Protect bladder from injury
Key viva point: Placed after reflecting the bladder flap in LSCS. Two Doyen's used - one for bladder, one for upper flap.
13. Green-Armytage Hemostatic Forceps
Description: Long, straight, hemostatic forceps with transverse serrations.
Uses (specifically for LSCS):
- Applied to the 4 angles and cut edges of uterine incision during C-section
- Prevent blood loss from uterine sinuses
- Hold flaps for suturing
Key viva point: "4 Green-Armytage forceps are used in LSCS" - 2 for cut edges, 1 for each angle.
14. Pinard's Fetoscope
Description: Trumpet/cone-shaped monaural stethoscope. Wooden or metal. Wide end on maternal abdomen, narrow end to examiner's ear.
Use: Auscultate fetal heart sounds. Normal FHR = 110-160 bpm.
Key viva point: Primitive, now replaced by Doppler. Still used in resource-limited settings. Cannot detect FHR variability (only rate). Doppler preferred from 12 weeks, Pinard from 28 weeks.
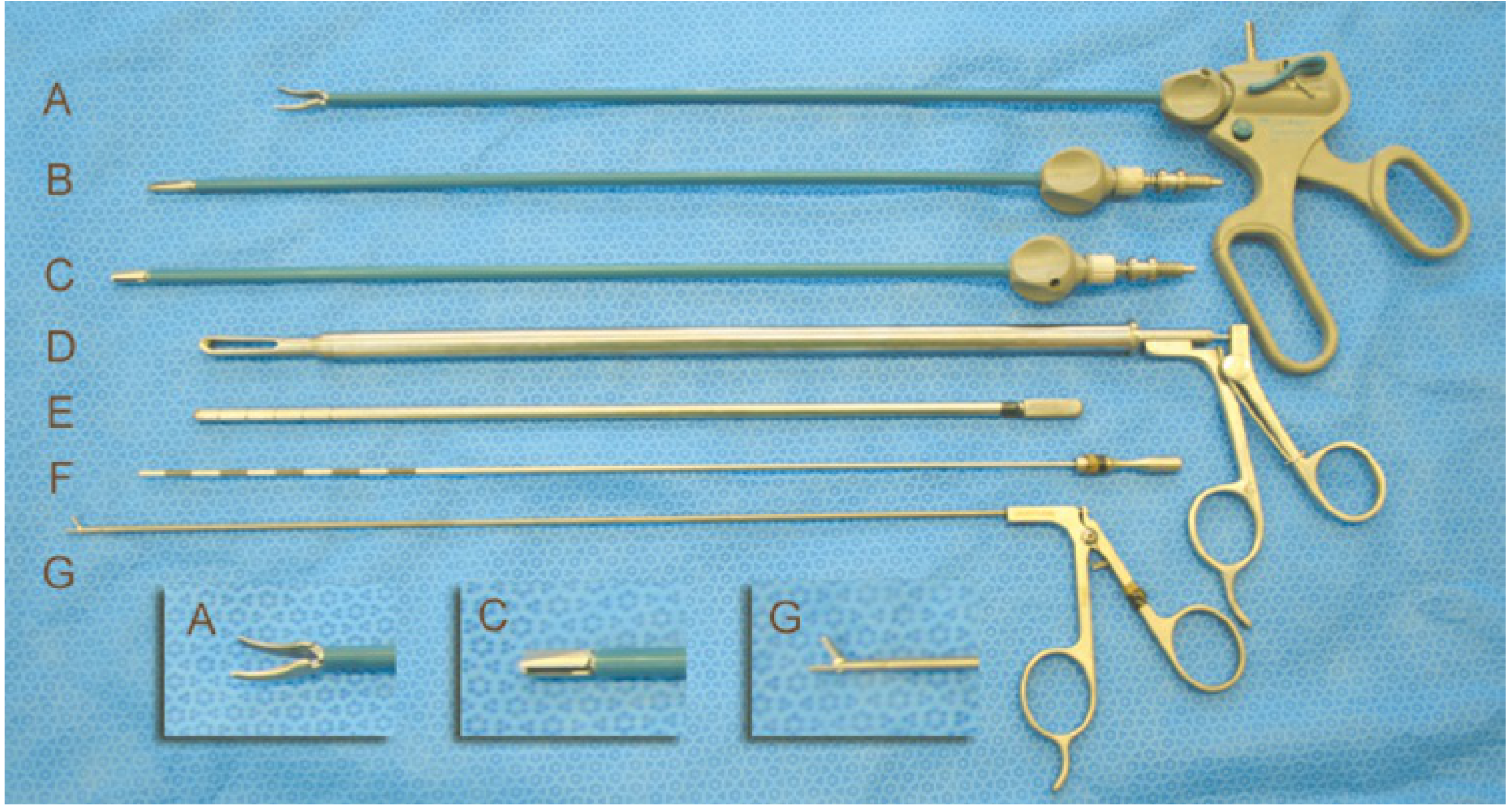
15. Laparoscopic Instruments (from Berek & Novak's Gynecology)
The following images are from the Berek & Novak's Gynecology textbook, showing actual surgical instruments used in gynecologic laparoscopy:
Laparoscopic Grasping Forceps Set (A-G):
Laparoscopic instruments: A = Maryland graspers (5 mm curved tip), B & C = alternate tips for same handle, D = 10 mm claw grasper, E & F = 5 mm and 2 mm manipulating probes, G = 2 mm grasping forceps - Berek & Novak's Gynecology
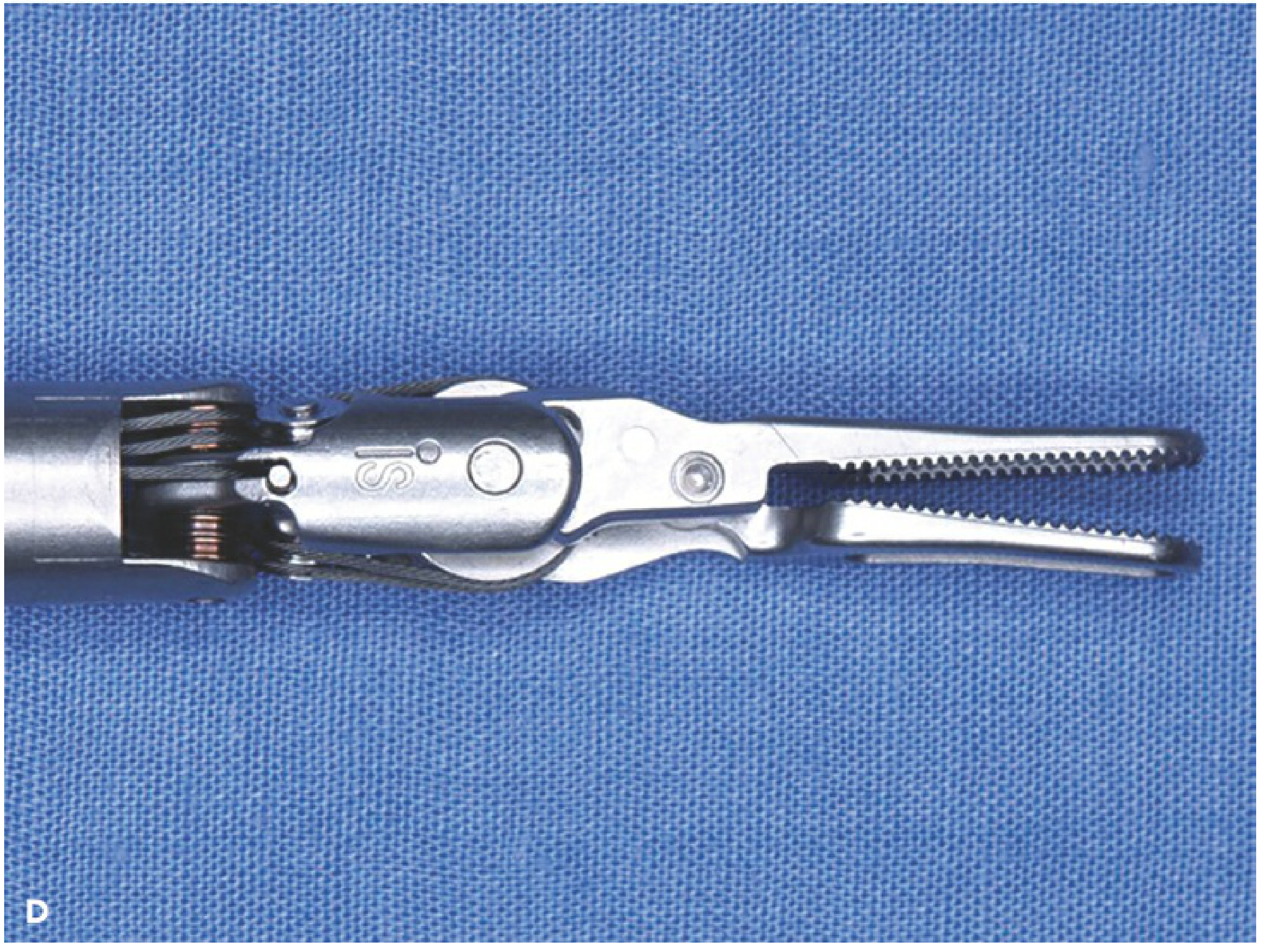
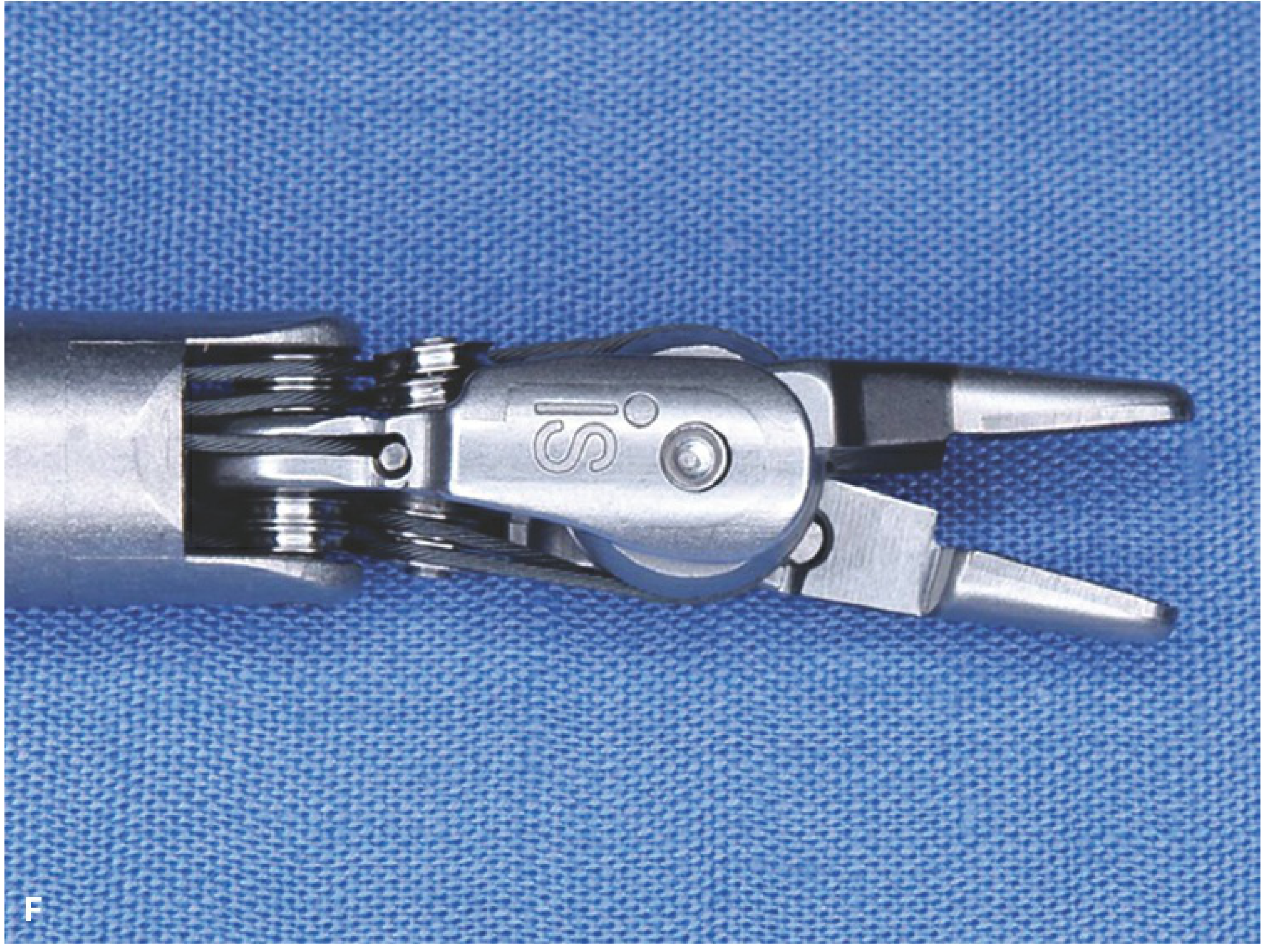
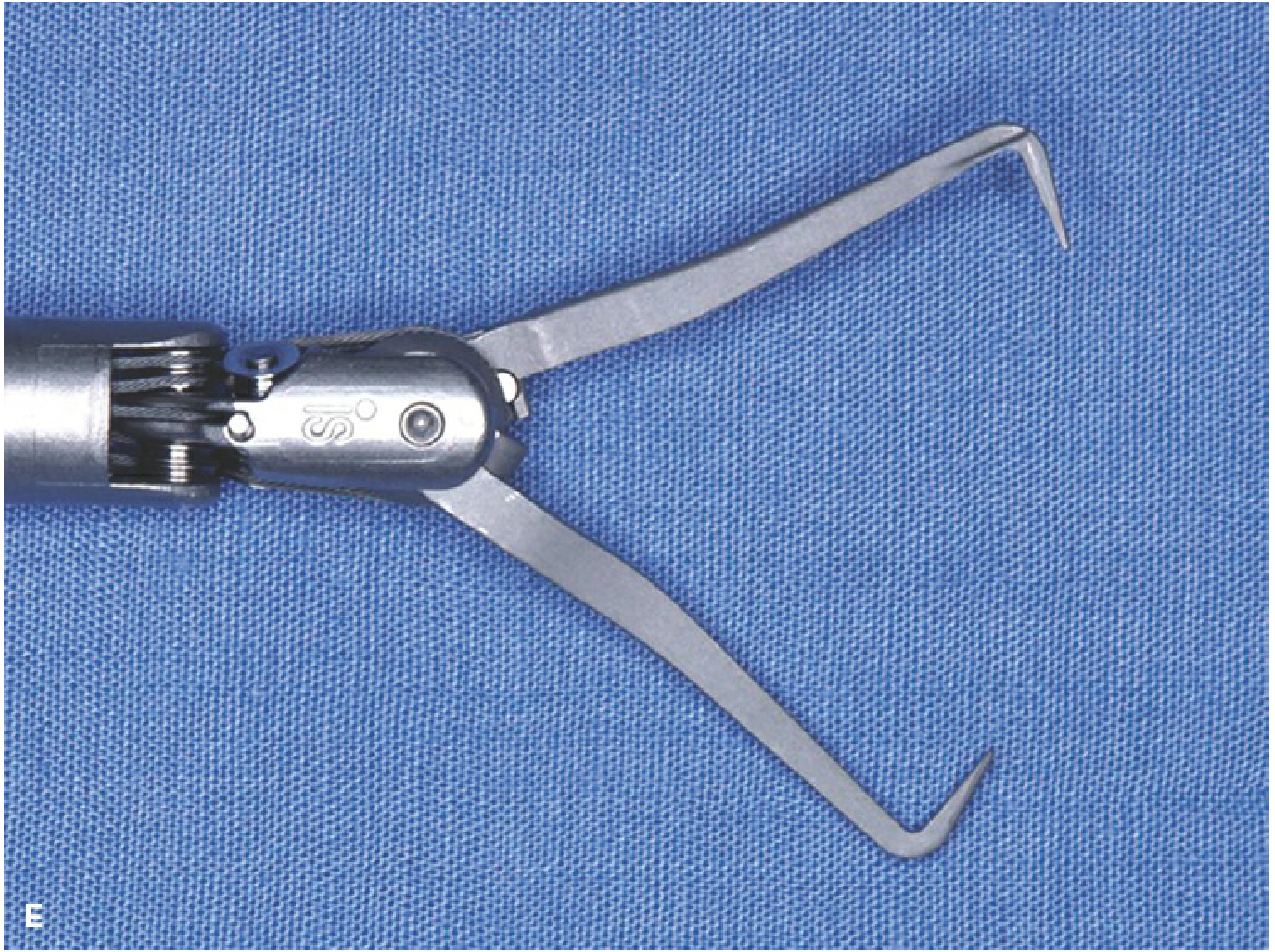
Robotic EndoWrist Instruments (used in Robotic/Da Vinci gynecologic surgery):
Robotic articulated scissors (curved tip, 7 degrees of freedom) - Berek & Novak's Gynecology
Robotic needle driver with serrated jaws - used for suturing in robotic hysterectomy/myomectomy - Berek & Novak's Gynecology
Robotic bipolar grasping forceps - tissue manipulation and hemostasis - Berek & Novak's Gynecology
Robotic curved/hooked grasper - used for uterine retraction in laparoscopic procedures - Berek & Novak's Gynecology
16. Hodge Pessary
Description: Hard rubber, elongated oval shape with notches. Placed in vagina.
Uses:
- Correct retroverted uterus (retroversion)
- Manage uterovaginal prolapse (temporary)
- Stress urinary incontinence
Key viva point: Ring pessary preferred for prolapse in elderly unfit patients. Pessaries need regular removal and cleaning (every 3-6 months).
17. IUCD - Copper-T 380A
Description: T-shaped device with copper wire wound around vertical arm and copper sleeves on horizontal arms.
How it works: Copper ions are spermicidal + alter endometrial environment. Also inhibits fertilization.
Effectiveness: >99%, lasts 10 years (Cu-T 380A). Can also be used as emergency contraception within 5 days.
Contraindications: Wilson's disease, heavy/irregular bleeding, copper allergy, pelvic infection (PID), distorted uterine cavity, unexplained vaginal bleeding.
Key viva point: Insertion timing: during menstruation OR first 48 hrs postpartum OR 4-6 weeks postpartum (interval). String should be felt on vaginal examination.
Quick Reference: "Instrument → Procedure" Table
| Procedure | Key Instruments |
|---|
| D&C | Sim's speculum + Vulsellum + Uterine sound + Hegar's dilators + Sharp curette |
| Surgical MTP / Incomplete abortion | Above + Haywood Smith's ovum forceps + Karman's cannula |
| Pap smear / Cervical exam | Cusco's speculum + Ayre's spatula/cytobrush |
| IUCD insertion | Cusco's speculum + Uterine sound + IUCD inserter |
| LSCS | Doyen's retractor + Green-Armytage forceps + Bonney clamps |
| Forceps delivery | Anderson's / Wrigley's forceps |
| Vacuum delivery | Ventouse cup + vacuum pump |
| Episiotomy | Episiotomy scissors |
| Laparoscopy | Veress needle + Trocar + Cannula + Telescope/laparoscope |
| Fetal monitoring | CTG machine, Pinard's fetoscope |
Note: Some Wikipedia instrument image URLs may not render if Wikimedia restricts direct embedding. In that case, right-click the links above and open in a new tab to view the clinical photos. The textbook CDN images (cdn.orris.care) are fully rendered above.