Acl basics. Give biomechanics of normal knee vs acl deficient knee
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive content. Let me now compose the full answer.
ACL Basics: Biomechanics of the Normal vs. ACL-Deficient Knee
1. Anatomy of the ACL
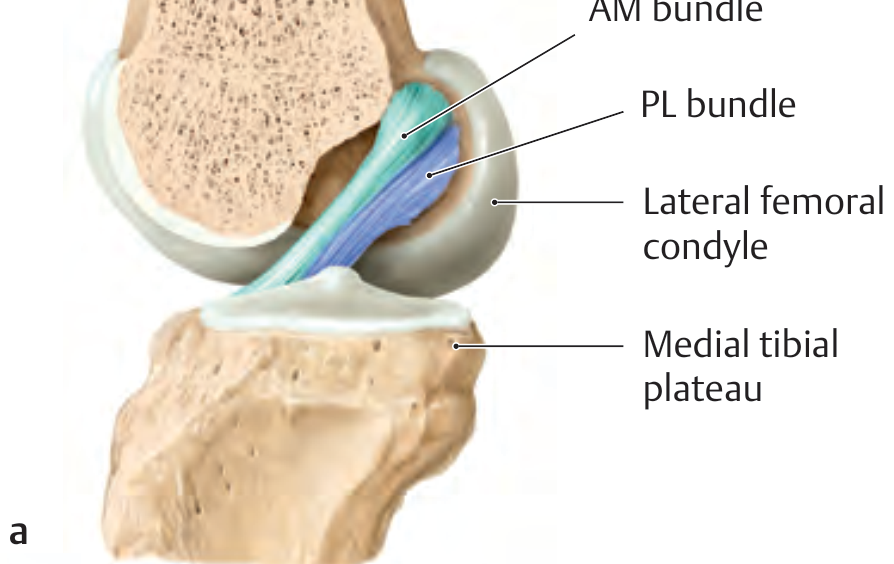
The ACL runs from the posterior lateral wall of the intercondylar fossa of the femur to the anterior tibial plateau, between the tibial spine attachments of the menisci. It is composed of two functional bundles named by their tibial insertions:
| Bundle | Length | Primary function |
|---|---|---|
| Anteromedial (AM) | ~38 mm | Anterior tibial restraint in flexion (>45°) |
| Posterolateral (PL) | ~20 mm | Anterior tibial restraint in extension; rotatory stability |
The femoral origins of both bundles sit in the posterior lateral intercondylar fossa: the AM bundle borders superiorly on the intercondylar line, and the PL bundle courses along the bone-cartilage border. As they pass through the notch, the two bundles lie behind each other, giving the ACL an oval cross-section.
— THIEME Atlas of General Anatomy and Musculoskeletal System
2. Biomechanics of the Normal Knee
Primary restraint: anterior tibial translation
The ACL is the primary restraint to anterior tibial translation — this is its most important biomechanical role. The in-situ force in the ACL is highest at ~30° of flexion in response to an anterior tibial load.
Reciprocal bundle tension through range of motion
The two bundles show reciprocal tension across the arc of flexion — a critical design feature:
- Extension (0°): PL bundle is taut; AM bundle is relatively lax → PL bundle primarily resists anterior translation and provides rotatory stability
- Flexion (>45°): AM bundle tightens as the ACL becomes more horizontal; PL bundle loosens → AM bundle carries the dominant force
This reciprocal tensioning ensures ACL stability across the full arc of knee motion.
— Rockwood & Green's Fractures in Adults, 10th ed.; THIEME Atlas
Screw-home mechanism
The ACL also guides tibial rotation during the screw-home mechanism — the obligatory external tibial rotation that occurs as the knee moves into terminal extension. This is coupled with the asymmetric femoral condyle geometry, and the ACL acts as a rotational guide rope.
Restraint to internal tibial rotation
Internal rotation places strain on the ACL. The PL bundle plays the most significant role in resisting internal rotation (rotatory laxity).
3. The ACL-Deficient Knee: Altered Biomechanics
Loss of anterior tibial translation control
Without the ACL, the tibia translates anteriorly on the femur — this is detected clinically by:
- Lachman test (most sensitive, at 30° flexion) — tests AM bundle
- Anterior drawer test (90° flexion) — tests AM bundle
- KT-1000/2000 arthrometer — quantifies laxity
Pivot shift: the rotatory instability signature
The ACL-deficient knee has increased internal tibial rotation compared with the intact knee. This manifests clinically as the pivot shift — subluxation of the lateral tibial plateau anteriorly in extension, with spontaneous reduction as the knee flexes past ~30–40° (pulled back by the iliotibial band). The pivot shift is the hallmark of rotatory instability and is the examination finding most closely correlated with functional outcome after reconstruction.
"The ACL-deficient knee has increased internal tibial rotation compared with the ACL-intact knee (i.e., positive pivot shift); it is likely that the PL bundle plays the most significant role in this respect." — Rockwood & Green's Fractures in Adults, 10th ed.
Altered joint kinematics and secondary stabilizers
When the ACL is absent, the secondary stabilizers are recruited excessively:
- Posterior horn of the lateral meniscus acts as a secondary restraint to anterior tibial translation → explaining why acute lateral meniscal tears are more common at the time of ACL injury
- Medial meniscus becomes the dominant secondary restraint with chronic ACL deficiency → explaining why medial meniscal tears increase with chronicity
- MCL is injured concurrently in ~25% of cases (takes over rotatory load-sharing)
- PLC (posterolateral corner) injured in ~10%; unrecognized PLC injury is a leading cause of ACL reconstruction failure
Neuromuscular and proprioceptive loss
The ACL contains mechanoreceptors (Ruffini endings, Pacinian corpuscles) that contribute to proprioception and reflex hamstring activation. ACL rupture disrupts this feedback loop, leading to:
- Reduced quadriceps inhibition signaling
- Impaired hamstring co-contraction (the hamstrings normally act as ACL agonists by producing posterior tibial force)
- Altered landing patterns and increased re-injury risk
Long-term: progressive joint deterioration
- Chronic ACL deficiency → increased complex meniscal tears not amenable to repair, and chondral injury
- Chondral and meniscal injuries at the time of initial ACL rupture are the main predictors of arthritic change (not ACL absence per se)
- There is currently no high-level evidence that ACL reconstruction alone reduces the risk of developing arthritis
— Miller's Review of Orthopaedics, 9th ed.
Summary Table: Normal vs. ACL-Deficient Knee
| Parameter | Normal Knee | ACL-Deficient Knee |
|---|---|---|
| Anterior tibial translation | Controlled (ACL primary restraint) | Increased (positive Lachman/drawer) |
| Internal tibial rotation | Controlled (PL bundle) | Increased (positive pivot shift) |
| Screw-home mechanism | ACL-guided | Disrupted |
| Bundle tension at 30° | PL taut, AM relatively lax | Neither functioning |
| Rotatory stability | PL bundle + secondary stabilizers | Lost; secondary restraints overloaded |
| Meniscal load-sharing | Normal | Lateral meniscus acutely, medial chronically overloaded |
| Proprioception | Intact (mechanoreceptors) | Impaired |
| Long-term joint health | Preserved | Progressive meniscal/chondral degeneration risk |
Key clinical takeaway: ACL rupture is not merely a loss of a static restraint — it fundamentally alters knee kinematics (anterior translation + rotatory instability), shifts load onto secondary stabilizers (menisci, MCL, PLC), and disrupts neuromuscular proprioception, collectively explaining the instability, associated injuries, and long-term articular consequences of the ACL-deficient knee.
This is a shared conversation. Sign in to Orris to start your own chat.