Give a brief summary on topic vt and lbbb
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a brief but thorough summary of both topics, sourced from multiple authoritative textbooks.
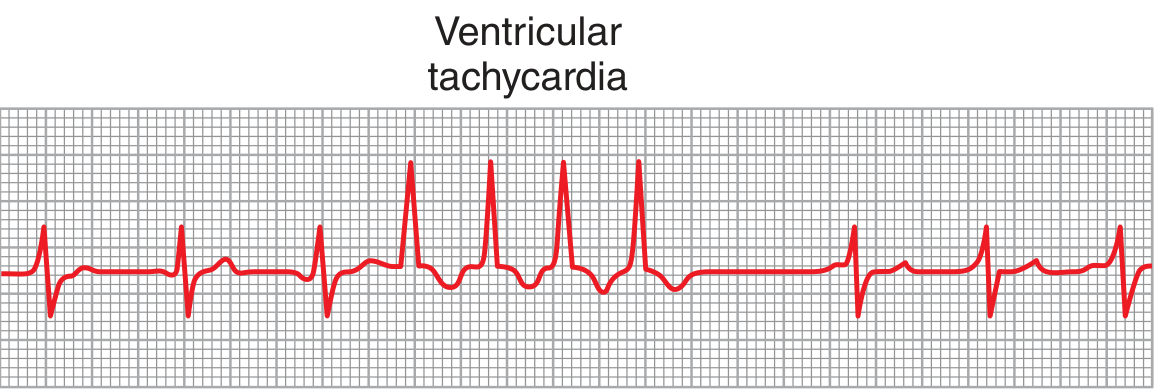
Ventricular Tachycardia (VT)
Definition & Mechanism
VT is a tachyarrhythmia that originates within or below the His bundle. It is defined as three or more consecutive ventricular beats. The most common mechanism is re-entry through scarred myocardium, though automatic and triggered mechanisms also occur.
- Nonsustained VT: lasts <30 seconds and terminates spontaneously
- Sustained VT: lasts ≥30 seconds or requires termination
Types
| Type | Description |
|---|---|
| Monomorphic VT | Uniform QRS morphology; rate 150-200 bpm; most common form |
| Polymorphic VT | Varying QRS morphology; suggests more severe underlying disease |
| Torsades de Pointes | Polymorphic VT with undulating QRS axis; occurs with prolonged QT; rate >200 bpm |
ECG Appearance
The ECG shows a series of ventricular premature beats occurring consecutively, with wide, bizarre QRS complexes without normal beats interspersed.
Causes
- Ischemic cardiomyopathy (most common)
- Non-ischemic cardiomyopathy
- Digitalis toxicity (irritable foci)
- Electrolyte disturbances
- Prolonged QT (for Torsades de Pointes - hypokalemia, hypomagnesemia, drugs like class IA/IC agents)
Why It's Dangerous
- VT usually indicates significant ischemic myocardial damage
- It frequently degenerates into ventricular fibrillation, which is almost invariably fatal without immediate intervention
Treatment
| Scenario | Treatment |
|---|---|
| Stable VT | Amiodarone 3-5 mg/kg IV over 20 min (up to 90% success) as first line; Procainamide 30-50 mg/min IV (second line); Lidocaine 1.0-1.5 mg/kg IV as alternative |
| Unstable VT / refractory | Synchronized cardioversion (100 J biphasic; escalate to 200 J or 360 J monophasic if needed) |
| Refractory/recurrent VT | Catheter ablation; surgical subendocardial resection or cryoablation (85-90% success, but 5-15% operative mortality) |
| Long-term | ICD implantation; cardiology referral |
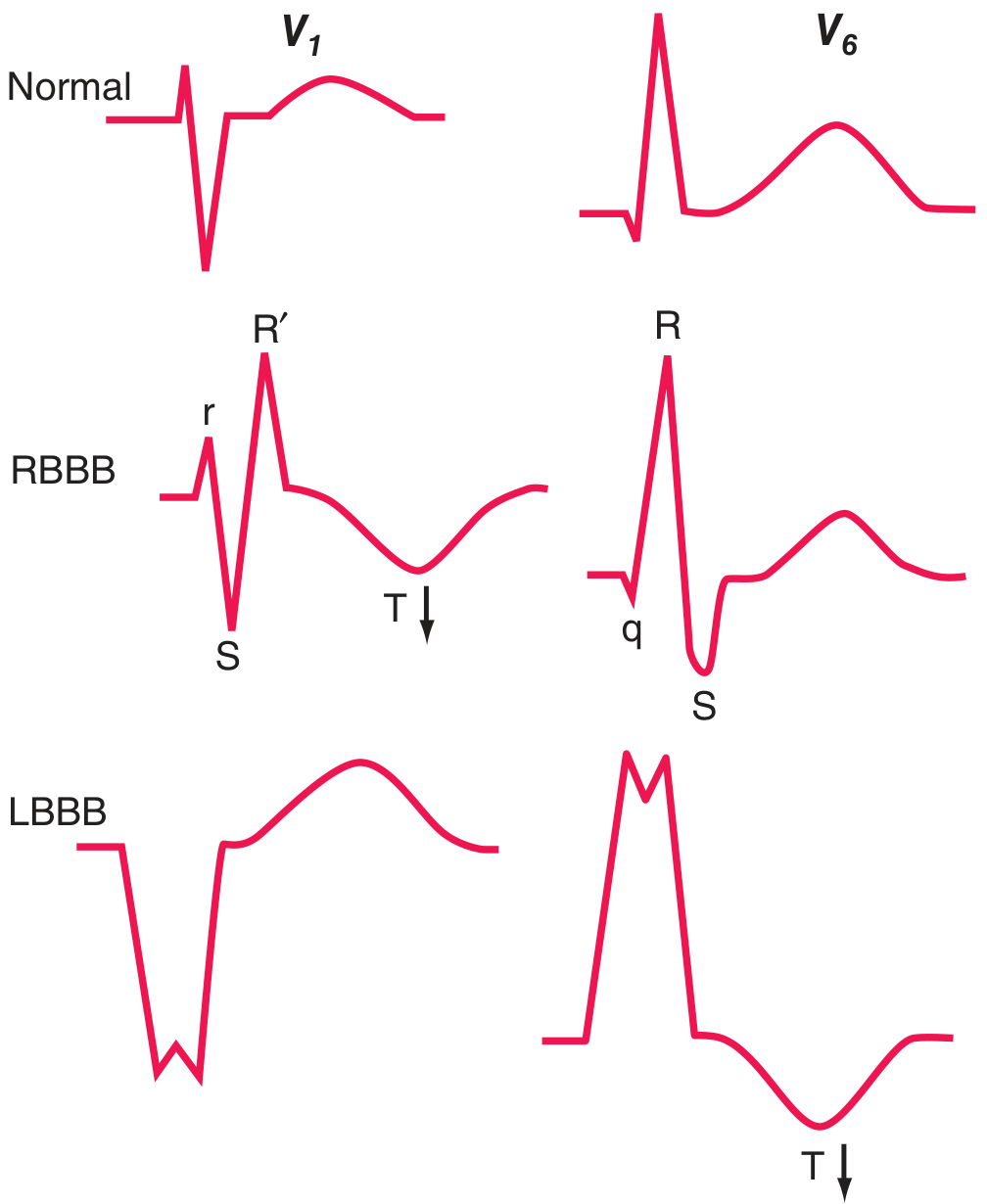
Left Bundle Branch Block (LBBB)
Definition & Mechanism
LBBB is a conduction abnormality in which the left bundle branch fails to conduct normally, causing delayed and abnormal depolarization of the left ventricle. As a result, depolarization spreads from the right ventricle to the left, producing characteristic ECG changes.
ECG Features
- Wide QRS (≥120 ms)
- V1: broad, predominantly negative (QS) complex
- V6: entirely positive, wide R wave
- T-wave discordance: T wave is typically opposite in polarity to the last QRS deflection (secondary repolarization change)
Causes / Associated Conditions
LBBB is often a marker of serious underlying cardiac disease (unlike RBBB, which can be seen in healthy individuals). The four main associations are:
- Coronary artery disease (often with impaired LV function)
- Hypertensive heart disease
- Aortic valve disease (including post-TAVR)
- Cardiomyopathy
LBBB may be chronic, intermittent, or rate-related (appearing when heart rate exceeds a critical threshold).
Clinical Significance
- Masks ST-segment analysis: LBBB obscures ischemia detection on ECG
- New LBBB + clinical findings of acute MI: treated as STEMI equivalent - patient should undergo the same triage and reperfusion pathway
- Specific ECG clues to MI in the setting of LBBB include:
- Q waves in two of leads I, aVL, V5, V6
- R wave regression V1 to V4
- ST elevation ≥1 mm in leads with a positive QRS
- ST depression ≥1 mm in V1, V2, or V3
- ST elevation ≥5 mm in leads with a negative QRS (Sgarbossa criteria)
Treatment
- LBBB itself may not require direct treatment if asymptomatic
- In heart failure with reduced EF + LBBB: strong indication for cardiac resynchronization therapy (CRT/biventricular pacing) - or increasingly, left bundle branch area pacing (LBBAP)
- For bifascicular block with syncope: pacemaker implantation preferred over ICD monitor alone
Key Link Between VT and LBBB: LBBB can rarely be associated with sudden cardiac arrest, as slow and dyssynchronous conduction may induce regional ventricular stretch and predispose to arrhythmias. Also, differentiating VT from aberrant conduction (e.g., LBBB morphology SVT) is a common clinical challenge - broad complex tachycardias with LBBB morphology must be carefully evaluated.
Sources: Goldman-Cecil Medicine; Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22e; Guyton & Hall Medical Physiology - medical textbook library
This is a shared conversation. Sign in to Orris to start your own chat.