Peroneal nerve palsy
Reading File
Finding Sources
Finding Sources
Searching Images
peroneal nerve palsy anatomy foot drop
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
common peroneal nerve anatomy fibular head branches diagram
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive overview of Peroneal Nerve Palsy based on authoritative textbook sources:
Peroneal Nerve Palsy (Common Fibular Neuropathy)
Anatomy
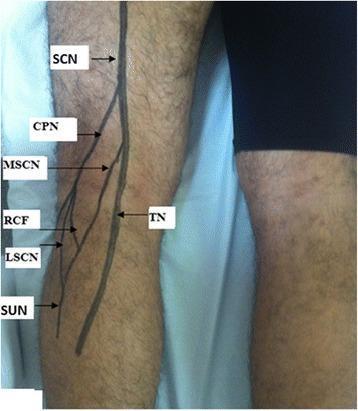
The common peroneal (fibular) nerve is the lateral terminal branch of the sciatic nerve, arising in the popliteal fossa. It winds around the fibular head — where it is superficial and poorly protected — before dividing into two main branches:
- Deep peroneal nerve → innervates toe and foot dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus); sensory to the 1st web space
- Superficial peroneal nerve → innervates peronei (foot evertors); sensory to the lateral lower leg and dorsum of the foot (sparing the 1st web space)
The fibular head is the most common site of injury because the nerve is superficial, poorly cushioned, and tethered as it wraps anteriorly around the bone.
Causes
In a series of 318 knee-level peroneal nerve lesions, the distribution was:
- Stretch/contusion without fracture (44%)
- Tumors (13%)
- Laceration (12%)
- Entrapment (9%)
- Stretch/contusion with fracture (7%)
- Compression (7%)
- Iatrogenic (4%)
- Gunshot wounds (4%)
Common specific scenarios:
- Leg crossing — habitual pressure at the fibular head
- Prolonged bed rest / weight loss — loss of subcutaneous padding
- Lithotomy position — stretch with hip/knee flexion
- Lateral decubitus positioning (operative) — limb resting against a leg strap
- Total knee arthroplasty (TKA) — valgus-flexion deformity is the highest-risk configuration; aberrant retractor placement compressing the nerve against the proximal fibula
- Knee dislocation — traction or blunt injury to the lateral knee
- Sports injury — "punter's palsy" from forced inversion/plantarflexion
- Intraneural ganglia — from the superior tibiofibular joint capsule (underappreciated but treatable); associated with higher BMI, knee/peroneal distribution pain, and fluctuating weakness with weight bearing
- Casts, Baker cysts, tumors, hematomas, leprosy
— Localization in Clinical Neurology, 8e, p. 153–157; Miller's Review of Orthopaedics 9th Edition, p. 484
Clinical Features
Motor deficits:
| Deficit | Muscle | Branch |
|---|---|---|
| Foot drop (impaired dorsiflexion) | Tibialis anterior | Deep peroneal |
| Toe extension weakness | EHL, EDL | Deep peroneal |
| Foot eversion weakness | Peroneus longus/brevis | Superficial peroneal |
- The deep branch is more commonly affected than the superficial, so foot drop tends to dominate over eversion weakness
- In some patients, only the extensor hallucis longus is affected, producing big toe drop rather than full foot drop
- Gait: high-stepping (steppage gait) to avoid tripping
Sensory deficits:
- Dorsum of the foot and toes
- Lateral distal lower leg
- 1st web space (deep branch only)
Reflexes: Ankle (Achilles) reflex is preserved (tibial nerve function)
Tinel sign may be elicited by percussion at the fibular head.

Differential Diagnosis
The key differentials for foot drop include:
| Condition | Distinguishing feature |
|---|---|
| L5 radiculopathy | Back/leg pain; hip abduction and foot inversion also weak; normal EMG at fibular head |
| Lumbosacral plexopathy | Widespread L4–S1 weakness |
| Sciatic nerve palsy | Hamstring weakness + tibial distribution deficit |
| Paramedian cerebrocortical lesion | Foot inversion also weak (tibial nerve territory); UMN signs (brisk Achilles, upgoing plantar) |
| Tibialis anterior tendon rupture | No toe extensor or eversion weakness; palpable tendon defect; normal EMG |
Key distinguishing feature: In peroneal nerve palsy, foot inversion is preserved (tibialis posterior is tibial nerve). Weakness of foot inversion suggests a central or proximal (sciatic/plexus) lesion.
— Bradley and Daroff's Neurology in Clinical Practice, p. 480
Investigations
- EMG/Nerve Conduction Studies (NCS): Localise the lesion to the fibular head; distinguish axonotmesis from neuropraxia; assess prognosis
- MRI: Can identify intraneural ganglia, tumors, cysts, or structural compression
- If intraneural ganglion suspected: MRI of the knee with dedicated nerve imaging (SPGR FS sequences show fascicular architecture at the fibular head)
Management
Conservative (most cases):
- Remove compressive factors — change position, remove casts/wraps, avoid leg crossing
- Ankle-foot orthosis (AFO) — maintains ankle at 90° to prevent equinus contracture while awaiting nerve recovery
- Physiotherapy — maintain joint range of motion and muscle conditioning
Postoperative peroneal palsy (e.g., after TKA):
- First step: flex the knee and remove compressive wraps to decompress the nerve
Surgical:
- If no recovery after 3 months and nerve is intact on EMG/NCV → surgical exploration and decompression
- If intraneural ganglion: resection of the articular branch and ganglion with joint capsule repair
- For complete laceration or failed decompression: nerve repair or transfer
— Miller's Review of Orthopaedics 9th Edition, p. 484; ROSEN's Emergency Medicine, p. 3225–3228; Localization in Clinical Neurology, 8e, p. 155–157
Prognosis
- Neuropraxia (compression only, axons intact): Most recover within days to weeks; if not cut, most palsies show return within 3 months
- Axonotmesis: Slower recovery (axonal regeneration ~1–3 mm/day); outcome depends on length of nerve to reinnervate
- Neurotmesis (complete severance): Poor spontaneous recovery; requires surgical reconstruction
- Intraneural ganglia treated surgically have good outcomes if decompressed early
Summary: Peroneal nerve palsy most commonly results from compression at the fibular head, producing foot drop, toe extension weakness, and variable eversion deficit with sensory loss over the dorsum of the foot. EMG/NCS confirm localisation and guide prognosis. Management is initially conservative with an AFO; surgical decompression is indicated if no recovery by 3 months.
This is a shared conversation. Sign in to Orris to start your own chat.