Histology of skin
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from authoritative histology textbooks. Let me compile the full detailed answer.
Histology of Skin
The skin (cutis/integument) is the largest organ of the body, covering ~1.8 m² and constituting 15-20% of total body mass. It consists of three main layers: the epidermis, the dermis, and the hypodermis (subcutaneous layer).
Layers Overview
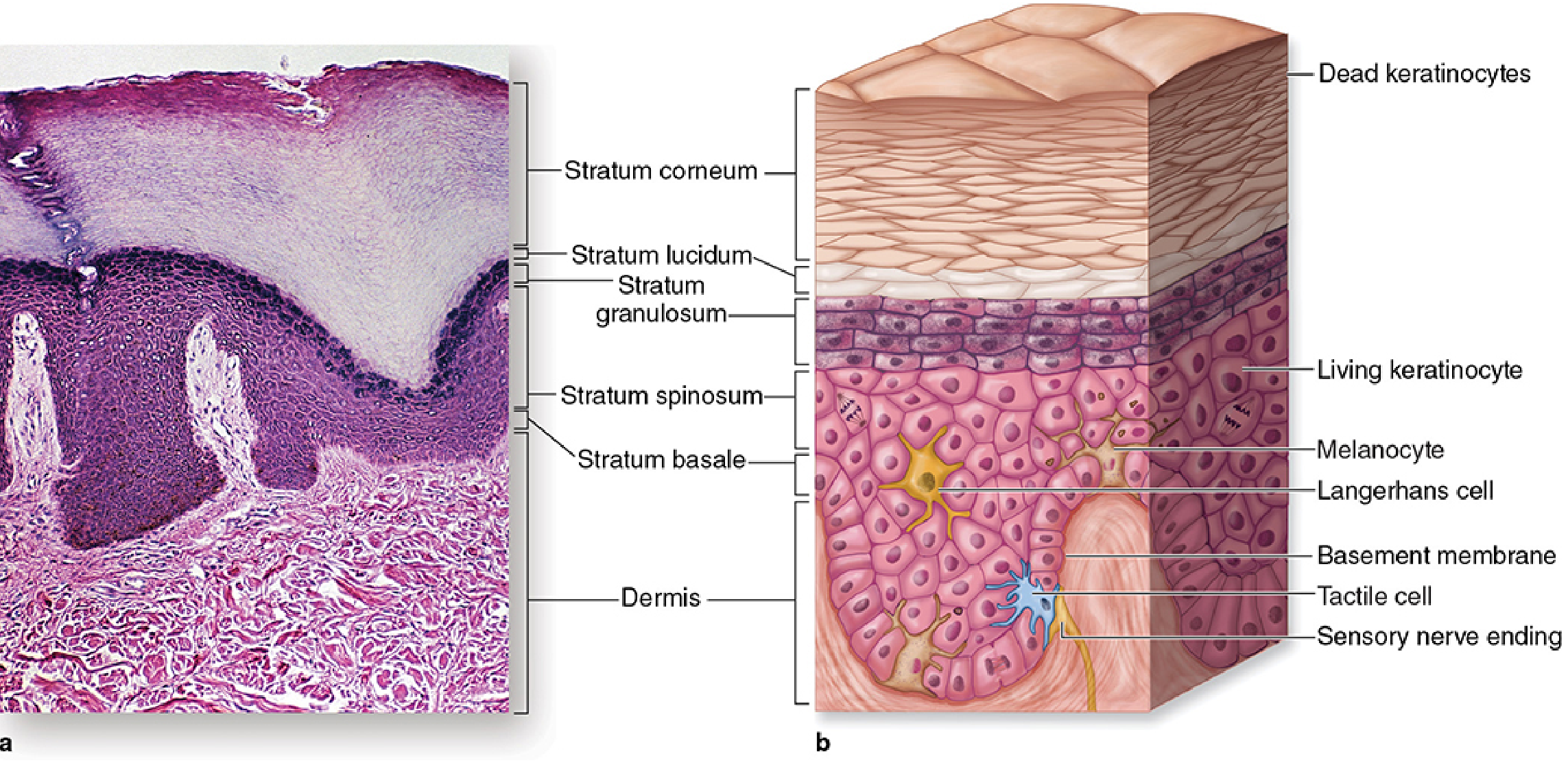
Thick skin showing all five epidermal strata and the underlying dermis (Junqueira's Basic Histology, 17e)
1. EPIDERMIS
The epidermis is a keratinized stratified squamous epithelium derived from ectoderm. It constitutes about 5% of skin thickness and has no blood vessels - cells receive nutrition by diffusion from the dermis.
Layers of the Epidermis (deep to superficial)
In thick skin (palms, soles), five layers are present. In thin skin (most body surfaces), the stratum lucidum is absent.
| Layer | Key Features |
|---|---|
| Stratum basale | Single layer; stem cells; active mitosis |
| Stratum spinosum | Several cells thick; prickle cells; tonofibrils |
| Stratum granulosum | Keratohyalin granules; lamellar bodies |
| Stratum lucidum | Thick skin only; translucent, anucleate |
| Stratum corneum | Fully keratinized; dead, flattened squames |
Stratum Basale (Stratum Germinativum)
A single layer of small, cuboidal to low-columnar cells resting on the basal lamina. These are the epidermal stem cells that give rise to all keratinocytes by mitotic division. Key features:
- Basophilic cytoplasm (closely spaced nuclei impart a deep blue stain)
- Connected to each other and overlying spinous cells by desmosomes
- Attached to the basal lamina by hemidesmosomes
- Contains scattered melanin granules transferred from neighboring melanocytes
- New keratinocytes generated here migrate upward, beginning their terminal differentiation journey
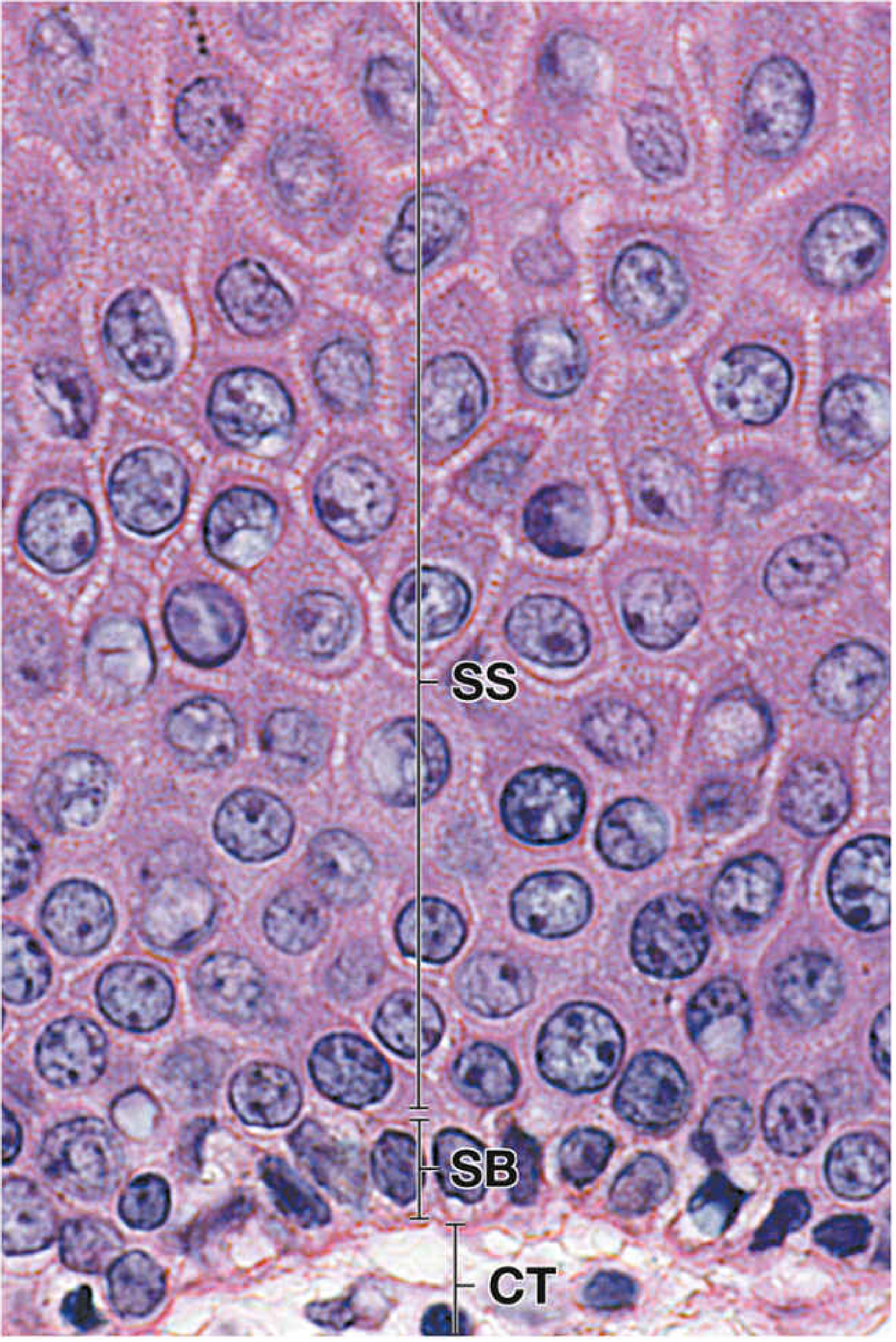
High-power H&E of the basal epidermis: SB = stratum basale, SS = stratum spinosum, CT = connective tissue (Histology: A Text and Atlas, 8e)
Stratum Spinosum (Prickle Cell Layer)
At least several cells thick. Keratinocytes here are larger than basal cells and characteristically show:
- Cytoplasmic spines (processes) linked to adjacent cells by desmosomes - visible as the "node of Bizzozero" (slight thickenings at desmosomal sites)
- Called "prickle cells" because cells shrink during histological processing, leaving expanded intercellular spaces between the spines
- Keratin intermediate filaments (tonofibrils) assemble here and converge at desmosomes
- Cells become progressively more flattened toward the surface
Stratum Granulosum
2-5 layers of flattened cells containing two distinctive features:
- Keratohyalin granules - basophilic, irregular granules containing loricrin and profilaggrin, which cross-link keratin filaments
- Lamellar bodies (membrane-coating granules / Odland bodies) - secreted at the interface with stratum corneum to form the epidermal water barrier (lipid-rich secretion). The turnover time through stratum spinosum + granulosum is ~31 days.
Cells in this layer show apoptotic nuclear morphology (DNA fragmentation) but do not undergo cellular fragmentation - instead they fill with keratin filaments.
Stratum Lucidum
Found only in thick skin. A pale, translucent band of 2-3 layers of anucleate, eosinophilic, densely packed cells. Considered a subdivision of the stratum corneum.
Stratum Corneum
The outermost layer of fully keratinized, dead, flattened squames (cornified cells):
- Cells (corneocytes) lack nuclei and organelles
- Packed with keratin filaments within a cornified envelope
- Cells are eventually shed (desquamation) from the surface
- Average thickness: 16-20 cell layers; turnover ~14 days in this layer
- The total epidermal turnover time is ~15-30 days
Non-Keratinocyte Cells of the Epidermis
Four cell types inhabit the epidermis:
1. Keratinocytes (~80%)
The structural cell; undergoes terminal differentiation (a form of specialized apoptosis) as it migrates from basale to corneum.
2. Melanocytes
- Dendritic cells of neural crest origin, located mainly in the stratum basale (1 per 4-40 basal keratinocytes - constant ratio across all skin types)
- Produce melanin in lysosome-related organelles called melanosomes (derived from Golgi)
- Synthesis pathway: L-tyrosine → L-DOPA → L-DOPAquinone → eumelanin (black-brown, when cysteine insufficient) or pheomelanin (yellow-red, when cysteine abundant), via the enzyme tyrosinase
- Mature melanosomes (Stage IV) travel to the tips of dendritic processes and are transferred to adjacent keratinocytes by a process called pigment donation - keratinocytes phagocytose the tips of melanocyte processes
- Melanosomes accumulate above and around keratinocyte nuclei, forming a "melanosome microparasol" that shields nuclear DNA from UV radiation
- Skin color differences arise from the number, size, and distribution of melanosomes - not the number of melanocytes
- Regulated by MSH (via MC1R receptor), ACTH, sex steroids, and UV exposure
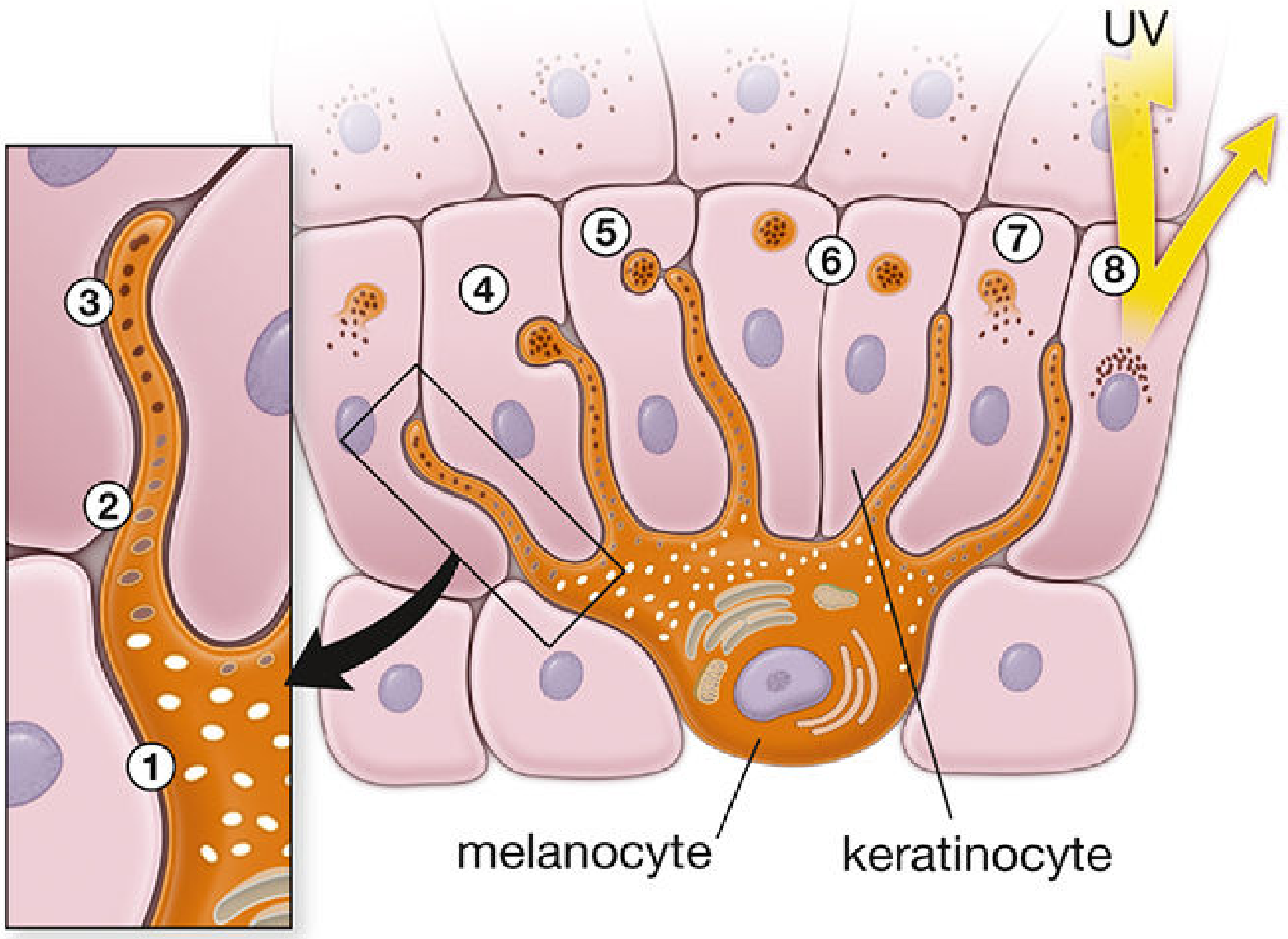
Melanin formation and pigment donation to keratinocytes (Histology: A Text and Atlas, 8e)
3. Langerhans Cells
- Dendritic antigen-presenting cells (resident macrophages) of the epidermis
- Derived from erythro-myeloid progenitor cells of the yolk sac - self-renewing, cannot be replenished by bone marrow monocytes
- Located primarily in the stratum spinosum
- In H&E sections appear as clear cells (like melanocytes, they do not pick up conventional stains well)
- Identified by CD1a, CD207 (langerin), and Birbeck granules (racket-shaped, visible only on electron microscopy - pathognomonic)
- Function: immunosurveillance - extend processes through tight junctions to sample the epidermal microenvironment; process antigens and migrate to lymph nodes as immunostimulatory cells
- Respond to pathogens and contact sensitizers (relevant in allergic contact dermatitis)
4. Merkel Cells
- Located in the stratum basale, especially in touch-sensitive areas (fingertips, lips)
- Modified epithelial cells acting as mechanoreceptors for light touch
- Contain dense-core granules with neuropeptides
- Associated with disc-shaped terminals of myelinated sensory (Type II) nerve fibers
- The Merkel corpuscle = Merkel cell + associated disc receptor
- Clinically relevant: Merkel cell carcinoma is an aggressive neuroendocrine skin tumor
2. DERMIS
The dermis constitutes 95% of skin thickness and is derived from mesoderm. It is composed of dense irregular connective tissue providing mechanical support, strength, and thickness.
Two Layers
Papillary Layer (superficial)
- Loose connective tissue immediately beneath the epidermis
- Thin collagen fibers: predominantly type I and type III collagen (ratio of type III:I increases with age)
- Thread-like elastic fibers forming an irregular network
- Contains dermal papillae and dermal ridges that interdigitate with the epidermis (increasing surface area of dermal-epidermal junction)
- Rich in blood vessels (capillary loops supplying but not entering the epidermis), lymphatics, and nerve processes
- Sensory nerve endings and receptors are concentrated here (Meissner corpuscles in dermal papillae)
Reticular Layer (deep)
- Always thicker and less cellular than the papillary layer
- Thick, irregular bundles of predominantly type I collagen and coarser elastic fibers
- Collagen = tensile strength; Elastic fibers = elasticity and resiliency
- Collagen/elastic bundles run in regular Langer's lines (cleavage lines) - surgical incisions parallel to these lines heal with minimal scarring
- Contains adnexal structures (hair follicles, sweat glands, sebaceous glands), smooth muscle (arrector pili), blood vessels, and nerves
Cells of the Dermis
- Fibroblasts - dominant structural cells; secrete collagen (types I, II, III, V, VII), proteoglycans, glycosaminoglycans, and multiadhesive glycoproteins; also have immune defense roles (express toll-like receptors)
- Dermal dendritic cells and resident macrophages (mononuclear phagocyte system)
- Mast cells - scattered throughout
- Lymphocytes - CD4+, CD8+, γ/δ T cells, regulatory T cells, NK cells, skin-resident memory T cells (Trm)
- Note: neutrophils are normally absent but infiltrate with injury or UV exposure
3. HYPODERMIS (Subcutaneous Layer)
- Equivalent to the subcutaneous fascia of gross anatomy
- Contains variable amounts of adipose tissue arranged in lobules separated by connective tissue septa
- Provides thermal insulation and energy reserve
- Contains the lower portions of hair follicles and sweat glands, larger blood vessels, and nerves
- The thin, largely vestigial panniculus carnosus (striated muscle) lies deep to the hypodermis; remnants persist as platysma and facial expression muscles in humans
4. SKIN APPENDAGES (Adnexal Structures)
All are downgrowths of the epidermis:
| Structure | Type | Key Features |
|---|---|---|
| Hair follicles | Invagination of epidermis | Arrector pili muscle attached; surrounds hair shaft |
| Eccrine sweat glands | Simple coiled tubular | Merocrine secretion; thermoregulation; present everywhere |
| Apocrine sweat glands | Modified sweat glands | In axilla, groin, areola; open into hair follicles; activated at puberty |
| Sebaceous glands | Holocrine | Open into hair follicles; secrete sebum; lubrication and antimicrobial |
| Nails | Plate of hard keratin | From nail matrix |
| Mammary glands | Modified apocrine | Produce milk |
Arrector pili muscles - smooth muscle bundles running from deep hair follicle to superficial dermis; contraction causes hair erection and "goose flesh" (cutis anserina)
5. SENSORY RECEPTORS OF THE SKIN
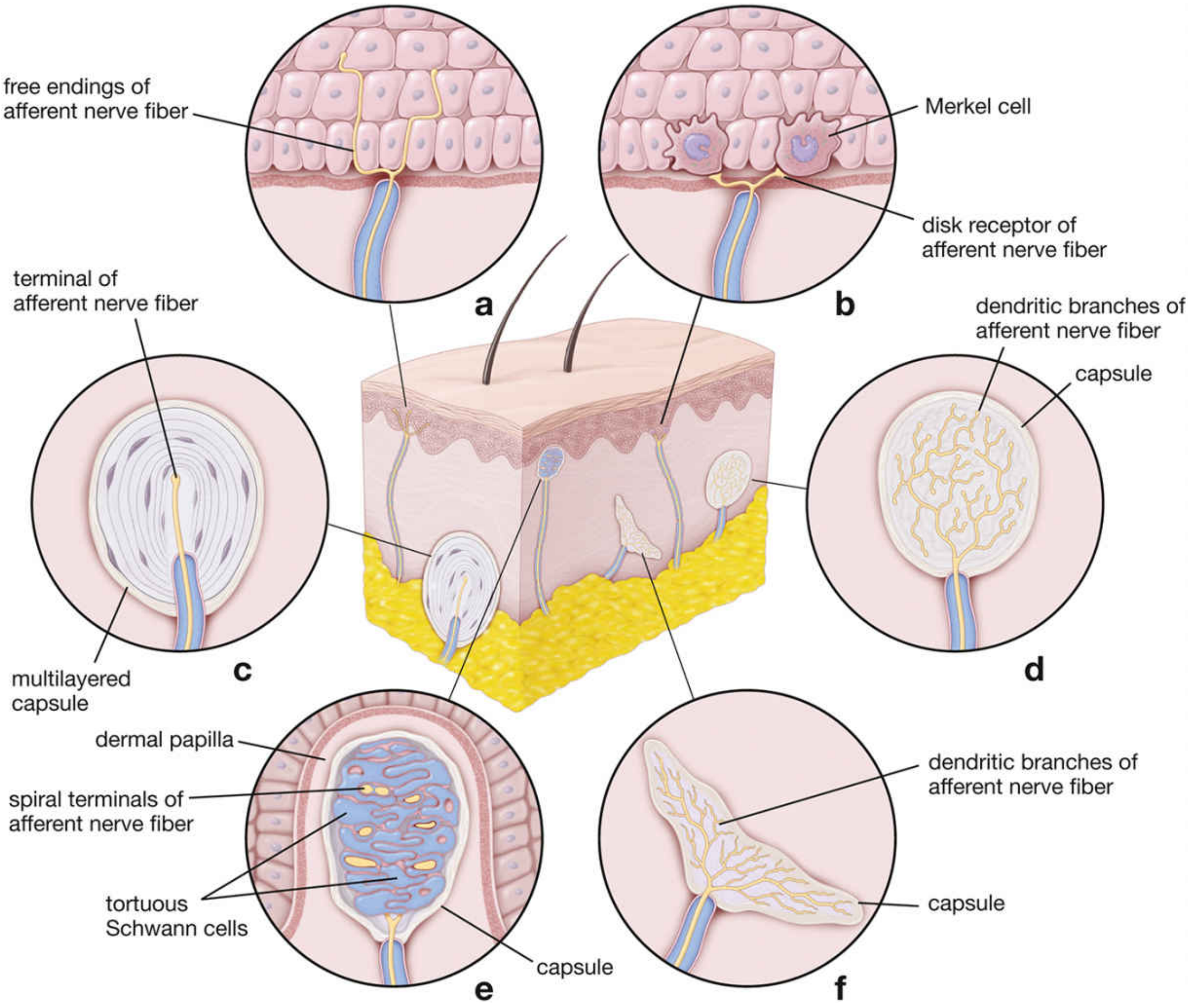
Types of cutaneous sensory receptors (Histology: A Text and Atlas, 8e)
| Receptor | Location | Modality |
|---|---|---|
| Free nerve endings | Epidermis (to stratum granulosum) | Pain, temperature, crude touch |
| Merkel corpuscles | Stratum basale | Light touch, sustained pressure |
| Meissner corpuscles | Dermal papillae | Fine/discriminative touch, vibration (low freq) |
| Pacinian corpuscles | Deep dermis/hypodermis | Deep pressure, high-frequency vibration |
| Ruffini corpuscles | Deep dermis | Skin stretch, joint position |
| Krause end bulbs | Dermis | Cold sensation |
6. THICK SKIN vs. THIN SKIN
| Feature | Thick Skin | Thin Skin |
|---|---|---|
| Location | Palms, soles | Most of body |
| Stratum lucidum | Present | Absent |
| Hair follicles | Absent | Present |
| Stratum corneum | Much thicker | Thinner |
| Eccrine sweat glands | Abundant | Present but fewer |
7. VASCULAR SUPPLY
The epidermis contains no blood vessels - all epidermal cells are nourished by diffusion from dermal capillaries. Blood anastomoses form five plexi: subfascial, fascial, subdermal, dermal, and subepidermal.
Clinical Correlations
- Vitiligo: selective loss of melanocytes → depigmentation
- Albinism: normal melanocyte count but defective melanin synthesis pathway
- Psoriasis: keratinocyte hyperproliferation → loss of granular layer, parakeratosis
- Langerhans cell histiocytosis: clonal proliferation of Langerhans cells; diagnosed by Birbeck granules on EM or CD1a/CD207 on immunohistochemistry
- Merkel cell carcinoma: aggressive neuroendocrine tumour of skin
- Langer's lines: incisions parallel to these heal with minimal scarring - important in surgery
- Friction blisters: space formed between epidermis and dermis of thick skin; calluses represent protective hyperkeratosis
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina & Ross), 8e; Junqueira's Basic Histology, Text and Atlas, 17e; Bailey & Love's Short Practice of Surgery, 28e
Cerebrospinal fluid renoria
Reading File
Finding Sources
Finding Sources
Searching the Web
CSF rhinorrhea cerebrospinal fluid nasal leak diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the essential content. Let me compile a comprehensive answer.
Note: "Renoria" appears to be a spelling variant or typo for rhinorrhea. This answer covers CSF rhinorrhea (cerebrospinal fluid leaking through the nose).
Cerebrospinal Fluid (CSF) Rhinorrhea
CSF rhinorrhea occurs when a skull base defect permits drainage of CSF from the intracranial subarachnoid space into the nose and paranasal sinuses. It requires a breach in the arachnoid/dura, skull base bone, and sinonasal mucosa - plus a pressure gradient to drive fluid flow.
CSF Physiology (Background)
- CSF is produced by the choroid plexus in the ventricles at a rate of ~20 mL/hour in adults
- Total CSF volume = 140 mL: 20 mL in ventricles, 50 mL in intracranial subarachnoid space, 70 mL in paraspinal subarachnoid space
- Normal CSF pressure: 4 cm H₂O (infants) to 14 cm H₂O (adults)
- Pressure fluctuates with respiration, arterial pulsation, and head position
- CSF resorption by arachnoid villi plays the major role in maintaining ICP - disruption leads to elevated ICP
Classification (Ommaya et al.)
I. TRAUMATIC
A. Accidental
- Immediate (within 48 hrs)
- Delayed (days to weeks after injury)
B. Surgical (Iatrogenic)
- Neurosurgical procedures - transsphenoidal hypophysectomy, frontal craniotomy, other skull base procedures
- Rhinologic procedures - endoscopic sinus surgery (ESS), septoplasty, combined skull base procedures
II. NONTRAUMATIC
A. Elevated Intracranial Pressure (ICP)
- Hydrocephalus
- Intracranial masses
- Empty sella syndrome (ESS) - pulsatile CSF pressure transmitted through arachnoid herniation into sella
B. Normal ICP
- Neoplasm (direct erosion of skull base)
- Infection (e.g., osteomyelitis)
- Granulomatous disease (granulomatosis with polyangiitis)
C. Idiopathic ("Spontaneous")
- Actually, most "idiopathic" cases have occult elevated ICP (mean 26-32 cm H₂O on lumbar puncture) - the CSF leak may serve as a pressure release valve
Epidemiology
- ~80% of CSF rhinorrhea results from accidental trauma (mostly closed head injury)
- CSF rhinorrhea occurs in only 2-3% of serious head trauma cases
- Skull base fracture is associated with a CSF fistula in 12-30% of cases
- More than 50% of traumatic CSF fistulas are at the anterior cranial base, mostly at the cribriform plate
- Only 4% of all CSF leaks are truly nontraumatic
- 16% result from intracranial/extracranial procedures
- Iatrogenic leaks are increasingly common: ~0.5% rate during endoscopic sinus surgery
- Most traumatic CSF leaks manifest within 2 days and almost all within 3 months of injury
Common Sites of Skull Base Defects
| Site | Common Cause |
|---|---|
| Cribriform plate | Head trauma, ESS |
| Ethmoid roof (fovea ethmoidalis) | Iatrogenic (sinus surgery) |
| Sphenoid sinus (lateral recess) | Idiopathic/elevated ICP |
| Frontal sinus | Anterior fossa fracture |
| Sella/parasellar | Transsphenoidal surgery |
The cribriform plate is the thinnest part of the skull base and is the most frequently involved site.
Clinical Features
Symptoms
- Watery, clear, unilateral nasal discharge - the hallmark; often described as salty tasting
- Volume increases with head-down position (Valsalva, straining, coughing, bending forward)
- Bilateral rhinorrhea suggests bilateral skull base defects
- Headache - positional, often relieved when lying flat (from intracranial hypotension when actively leaking)
- History of head trauma, prior skull base surgery, or trans-sphenoidal procedure is key
"Halo" or "Ring" Sign
- When CSF-containing nasal discharge drips onto a pillow or gauze, the CSF migrates further than blood/mucus, forming a pale outer ring around a darker central spot
- Not a specific test but raises suspicion
Diagnosis
The diagnostic process has two goals:
- Confirm the presence of CSF in the nasal secretion
- Localize the skull base defect
Step 1 - Confirm CSF
Beta-2 Transferrin (β-2 transferrin)
- Gold standard chemical marker
- A isoform of transferrin found almost exclusively in CSF (also in perilymph and aqueous humor - not in nasal secretions, serum, or saliva)
- Highly specific and sensitive
- Method: fluid is collected, sent for protein electrophoresis
- Limitations: requires ~0.5 mL of fluid; result may take days
Beta-trace Protein (β-TP / prostaglandin D2 synthase)
- Another highly specific CSF marker
- Faster turnaround than β-2 transferrin
- Both tests have significantly replaced older, less specific cisternography tests
Glucose Testing
- A nasal secretion glucose >30 mg/dL suggests CSF, but this is non-specific (glucose is also elevated in hyperglycemia, secretory rhinitis) - not reliable
Intrathecal Fluorescein
- Fluorescein dye injected intrathecally (into CSF)
- Used intraoperatively (and sometimes preoperatively) for precise localization of the leak
- Nasal endoscopy reveals a greenish hue at the defect site
- Confirms active leak and guides repair
- Not FDA-approved for intrathecal use but widely employed off-label
Step 2 - Localize the Defect
High-Resolution CT (HRCT) of the Skull Base
- First-line imaging after chemical confirmation
- 1 mm direct coronal images (or reformatted from 1 mm axial data)
- Identifies bony skull base dehiscences, fracture lines
- Provides excellent bony anatomical detail
- A bony defect on CT alone (without positive β-2 transferrin) is insufficient to diagnose active CSF leak
MRI of the Skull Base
- Complementary to CT
- Superior soft tissue detail
- Identifies meningoceles and meningoencephaloceles herniating through defects
- Detects empty sella (suggesting elevated ICP as etiology)
- MR with gadolinium or MR angiography helps identify vessels within encephaloceles (to avoid stroke during repair)
CT/MR Fusion
- Hybrid technique combining CT bony detail with MR soft tissue signal
- Emerging tool for complex defects
Cisternography (Radionuclide or CT)
- Now relegated to selected cases only due to high specificity of β-2 transferrin and β-TP
- CT cisternography: intrathecal iodinated contrast + CT; useful for large defects or when multiple potential sites are present
Management
Conservative (Non-Surgical)
Indicated first-line for most traumatic/accidental CSF leaks:
- Bed rest with head of bed elevation (30°)
- Avoidance of nose-blowing, Valsalva, straining
- Lumbar drainage (CSF diversion) - reduces ICP and flow through the defect
- Most traumatic leaks resolve spontaneously within 1 week with conservative measures
- Prolonged CSF leak > 7-10 days increases meningitis risk - earlier surgical intervention warranted
Surgical Management
Indicated for:
- All spontaneous/idiopathic leaks (will not resolve without repair)
- All iatrogenic leaks
- Traumatic leaks that fail conservative management (>7-10 days)
- Leaks with pneumocephalus
- Prevention of ascending meningitis
Endoscopic Repair (Primary Surgical Approach)
Since the 1980s, transnasal endoscopic repair has become the gold standard - it has supplanted open (intracranial) approaches for the vast majority of anterior skull base defects.
Steps:
- Standard endoscopic dissection for exposure of defect
- Intrathecal fluorescein administered to identify the defect
- Preparation of defect margins: mucosa within 5 mm of the defect removed (to allow graft adherence)
- Fulguration of any herniated meningocele/meningoencephalocele (never push it intracranially - risk of CSF gush and pneumocephalus)
- Graft placement
Grafting materials:
- Temporalis fascia, fascia lata
- Pedicled middle turbinate flaps
- Free cartilage/bone grafts (nasal septum, calvarium)
- Autogenous fat ("bath-plug" technique for small defects)
- Acellular dermal allograft
- Xenogeneic collagen dural substitutes (Durepair, Dura-Gen) for larger defects
- Meta-analysis (Hegazy et al., 289 fistulae): graft material choice does not significantly alter outcome
Graft placement technique:
- Underlay technique: graft placed on the intracranial side of the defect - ambient ICP holds it in place
- Bath-plug technique (Wormald): intracranial fat graft anchored by ICP
- Free grafts generally preferred over pedicled grafts (lower failure rate)
Success rate: Endoscopic repair achieves >90% success for most anterior skull base defects.
Intracranial (Open) Repair
- Reserved for complex, large, or posterior defects not accessible endoscopically
- Involves frontal craniotomy with direct dural repair
- Higher morbidity; anosmia risk (if cribriform plate dissected)
- Transglabellar subcranial approach allows direct access to anterior fossa floor with less frontal lobe retraction
Management of Elevated ICP
- All nontraumatic/idiopathic CSF rhinorrhea should be evaluated for occult raised ICP (even after successful repair)
- Lumbar puncture opening pressure measurement is essential post-repair
- If elevated ICP confirmed: treat with acetazolamide, weight loss (if obese), or CSF diversion (ventriculoperitoneal shunt, lumboperitoneal shunt)
- Failure to address elevated ICP leads to recurrence of the CSF leak after repair
Complications of Untreated CSF Rhinorrhea
| Complication | Notes |
|---|---|
| Bacterial meningitis | Most feared - risk increases with duration of leak; recurrent meningitis is the usual presentation of missed/delayed CSF rhinorrhea |
| Pneumocephalus | Air entering the subarachnoid space through the defect; tension pneumocephalus is life-threatening |
| Brain abscess | Rare |
| Encephalitis | Ascending infection |
The longer the CSF leak persists, the greater the risk of meningitis - early intervention is therefore preferred.
Antibiotic Prophylaxis
The routine use of prophylactic antibiotics for CSF rhinorrhea is controversial and not recommended by most guidelines. Evidence does not support reduced meningitis rates, and antibiotic use may select for resistant organisms.
Sources: Cummings Otolaryngology: Head and Neck Surgery, 7e (Chapter 48 - CSF Rhinorrhea and Anterior Skull Base)
This is a shared conversation. Sign in to Orris to start your own chat.