Minimally invasive procedures and their concepts in conservative dentistry . Give me answer for 25 marks with hand drawn exam style answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
minimally invasive dentistry concepts procedures conservative dentistry exam notes
Generating Image
Loading Image
The hand-drawn exam-style answer is generated. Now let me provide the full written answer text below it for complete 25-mark coverage.
Full Written Answer: Minimally Invasive Procedures and Concepts in Conservative Dentistry (25 Marks)
1. DEFINITION (2 marks)
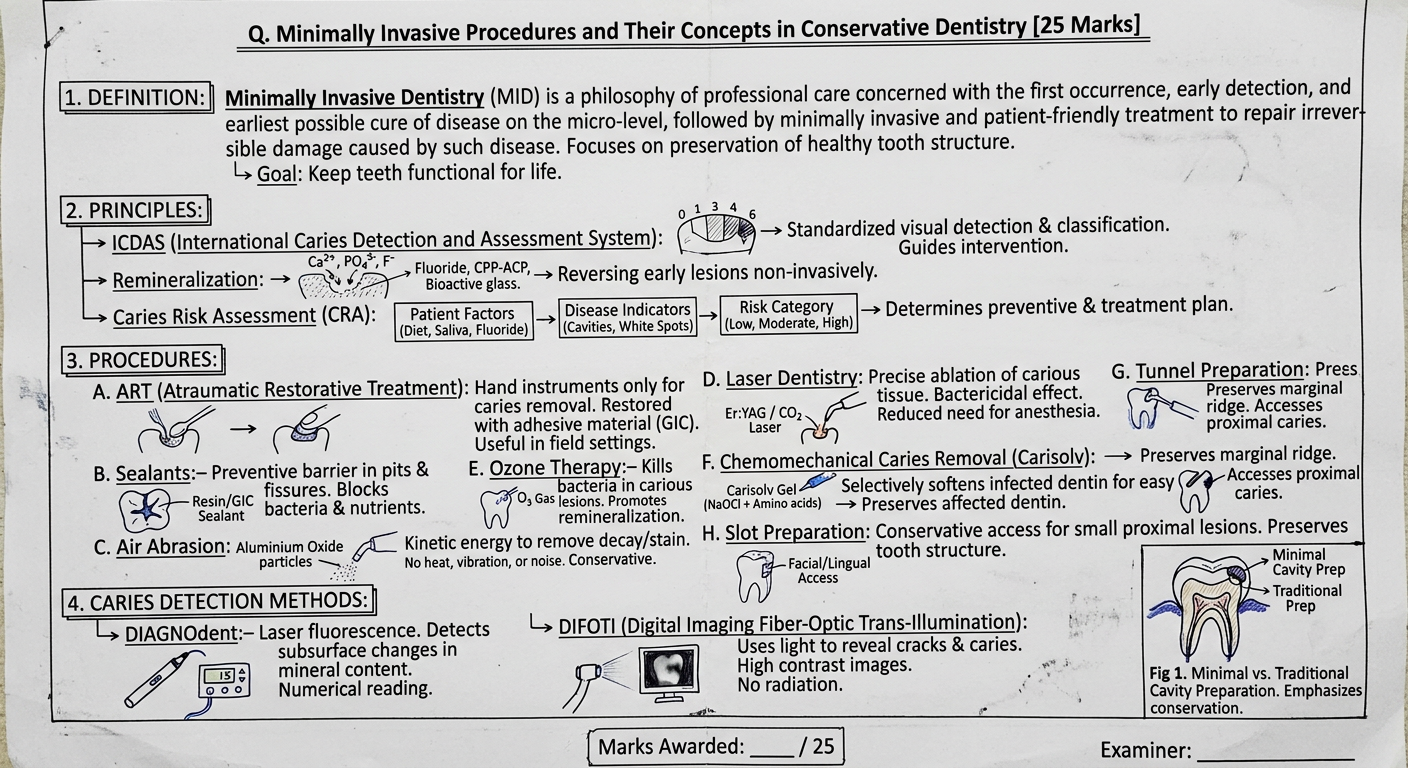
Minimally Invasive Dentistry (MID) is a philosophy of professional care concerned with the first occurrence, earliest detection, and earliest possible cure of dental disease at the micro-level, followed by minimally invasive and patient-friendly treatment to repair irreversible damage.
- Also called Minimal Intervention Dentistry (MI Dentistry)
- Proposed and popularized by the FDI World Dental Federation
- Core idea: Maximum preservation of healthy tooth structure
2. CONCEPTS / PRINCIPLES OF MID (5 marks)
| Principle | Explanation |
|---|---|
| Early caries detection | Use ICDAS, DIAGNOdent, DIFOTI to detect pre-cavitation lesions |
| Caries Risk Assessment (CRA) | Categorize patients as low/moderate/high risk; tailor prevention |
| Remineralization | Reverse early enamel lesions using fluoride, CPP-ACP, bioactive glass |
| Minimal cavity preparation | Remove only infected, not affected, dentine |
| Repair, not replace | Repair failed restorations rather than completely replacing them |
| Patient compliance | Dietary modification, oral hygiene, recall schedules |
3. CARIES DETECTION METHODS (3 marks)
a) DIAGNOdent
- Laser fluorescence device (655 nm red laser)
- Detects subsurface caries by measuring fluorescence of bacterial porphyrins
- Gives numerical reading: 0-99 (>21 = cavitated caries)
- Non-invasive, no radiation
b) DIFOTI (Digital Imaging Fiber-Optic Trans-Illumination)
- Uses visible light passed through tooth
- High-contrast digital images show cracks, caries, fractures
- No radiation; real-time images
c) ICDAS (International Caries Detection & Assessment System)
- Scores 0-6 based on visual-tactile examination
- Standardizes caries diagnosis and intervention thresholds
4. MINIMALLY INVASIVE PROCEDURES (12 marks)
A. Atraumatic Restorative Treatment (ART) (2 marks)
- Uses hand instruments only (no rotary burs, no electricity)
- Caries removed with excavators; cavity restored with GIC (Glass Ionomer Cement)
- GIC releases fluoride - promotes remineralization
- Ideal for: field settings, developing countries, anxious/young patients
- Evidence base: WHO promotes ART globally
B. Pit and Fissure Sealants (1 mark)
- Resin or GIC applied to susceptible pits and fissures of posterior teeth
- Blocks bacterial colonization and nutrient supply
- Most effective when applied soon after tooth eruption
- Preventive, not restorative
C. Air Abrasion (1 mark)
- High-velocity stream of aluminium oxide particles through pressurized air
- Removes caries/stains via kinetic energy
- Advantages: no heat, no vibration, no noise, no anesthesia needed
- Preserves healthy tooth structure
D. Laser Dentistry (2 marks)
- Er:YAG laser and CO2 laser used for caries removal
- Precisely ablates carious tissue without damaging healthy dentine
- Bactericidal effect on residual bacteria
- Reduced need for anesthesia; promotes adhesive bonding
- Also used for: cavity preparation, caries prevention (laser fluoride)
E. Ozone Therapy (1 mark)
- Ozone gas (O3) applied to carious lesion
- Kills cariogenic bacteria (S. mutans) by oxidative damage
- Promotes remineralization of early lesions
- Non-invasive for initial/root caries
F. Chemomechanical Caries Removal - Carisolv (2 marks)
- Carisolv gel (NaOCl + amino acids) applied to carious dentine
- Selectively softens and dissolves infected (denatured collagen) dentine only
- Affected (remineralizable) dentine is preserved
- Removed with special hand instruments (no bur required)
- Advantages: painless, conservative, no anesthesia in most cases
G. Tunnel Preparation (1 mark)
- Access to proximal caries from the occlusal surface through a tunnel
- Preserves the marginal ridge - most important contact area
- Restored with GIC
- Indication: Class II proximal caries with intact marginal ridge
H. Slot Preparation (1 mark)
- Access to proximal lesion from facial or lingual surface
- Conservative alternative to traditional Class II box preparation
- Preserves more tooth structure than conventional cavity
I. Ultrasonic/Sonic Preparation (1 mark)
- Oscillating tips remove caries with minimal vibration
- More conservative than conventional burs
- Useful in tight proximal areas
5. CAVITY DESIGN PRINCIPLES IN MID (2 marks)
| Traditional (G.V. Black) | Minimally Invasive |
|---|---|
| "Extension for prevention" | No extension; only diseased tissue removed |
| Outline form predetermined | Outline form dictated by extent of caries |
| Straight walls, flat floors | Irregular walls acceptable |
| Large restorations | Small, adhesive restorations (composite, GIC) |
- Adhesive dentistry has replaced mechanical retention as the foundation
- Composites and GIC bond to tooth - no need for undercuts
6. SUMMARY DIAGRAM
MINIMALLY INVASIVE DENTISTRY
|
┌──────┼──────────────┐
| | |
DETECT PREVENT TREAT
(ICDAS, (Fluoride, (ART, Laser,
DIAGNOdent, Sealants, Carisolv,
DIFOTI) CRA) Air Abrasion,
Ozone, Tunnel)
KEY TAKEAWAY
MID replaces the G.V. Black philosophy of "extension for prevention" with "prevention of extension" - treat only what is diseased, preserve what is healthy, and use modern bonded materials that do not require retentive cavity forms.
Mark distribution suggestion:
- Definition: 2 marks
- Principles/Concepts: 5 marks
- Detection methods: 3 marks
- Procedures (8-9 procedures): 12 marks
- Cavity design comparison: 2 marks
- Diagram/presentation: 1 mark
Some more information please this is not enough
Searching the Web
minimally invasive dentistry ART sealants air abrasion laser ozone carisolv detailed notes BDS exam
Searching the Web
minimally invasive dentistry CAMBRA silver diamine fluoride stepwise excavation hall technique conservative dentistry
Finding Sources
Reading Web Page
minimally invasive dentistry procedures concepts techniques caries
Generating Image
Loading Image
Generating Image
Generating Image
Here is the extended, detailed answer. The second hand-drawn sheet above covers many new procedures - and below is the full expanded written content:
EXTENDED ANSWER: Minimally Invasive Dentistry - Additional Topics
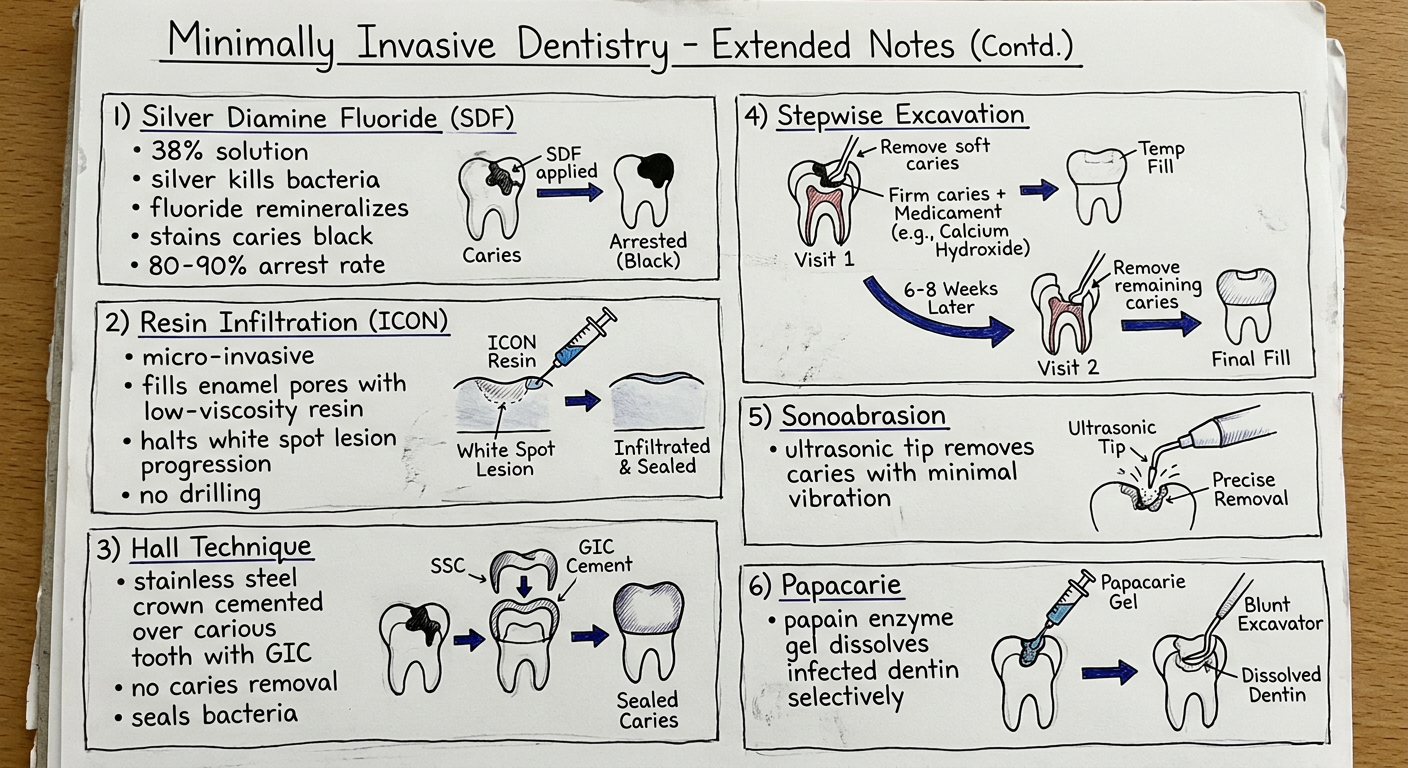
5. SILVER DIAMINE FLUORIDE (SDF)
- Composition: 38% aqueous solution of silver diamine fluoride
- Mechanism:
- Silver ions: bactericidal - kills S. mutans and other cariogenic bacteria
- Fluoride ions: promotes remineralization of softened enamel/dentine
- Together: arrests active caries lesions
- Clinical procedure: Apply with microbrush to carious lesion; no drilling
- Efficacy: 80-90% caries arrest rate in primary teeth (clinical trials)
- Limitation: Stains arrested caries permanently black (cosmetic concern)
- Uses: Elderly, anxious patients, pre-cooperative children, patients with special healthcare needs (SHCN)
- Classification: Non-operative (no cavity preparation required)
6. RESIN INFILTRATION (ICON - DMG, Hamburg)
- Classification: Micro-invasive procedure
- Indication: White spot lesions (initial enamel caries, ICDAS 1-2), non-cavitated proximal caries
- Mechanism: Fills enamel micropores with low-viscosity resin; halts progression by blocking acid diffusion pathways
- Step-by-step protocol:
- Etch with 15% HCl gel (Icon-Etch) for 2 min - opens enamel pores
- Dry with ethanol (Icon-Dry) - removes moisture, shows final optical result
- Infiltrate with low-viscosity resin (Icon-Infiltrant) - fills pores
- Light cure 40 sec
- Advantages: No drilling, no anaesthesia, prevents lesion from becoming cavitated, improves aesthetics (white spot disappears)
- Limitations: Only for non-cavitated lesions; not for active cavities
7. HALL TECHNIQUE (Stainless Steel Crown - Modified)
- Concept: Sealing caries rather than excavating it
- Procedure: Stainless Steel Crown (SSC) cemented over carious primary molar with GIC - no caries removal, no tooth preparation, no drilling
- Principle: Sealing bacteria from their carbohydrate substrate arrests the lesion (bacteria starve and become inactive)
- Evidence: 5 RCTs show clinical success equivalent to conventional SSC placement
- Best for: Primary molars in children, anxious/pre-cooperative patients
- Originator: Dr. Norna Hall, Scotland, 1990s
8. STEPWISE EXCAVATION
- Indication: Deep caries approaching pulp where complete removal risks pulp exposure
- Aim: Avoid unnecessary pulp exposure while removing infected caries
- Two-visit technique:
| Visit 1 | Visit 2 (after 6-8 weeks) |
|---|---|
| Remove soft (wet) caries only | Remove remaining firm caries |
| Leave firm (leathery) caries near pulp | Pulp usually protected by reactionary dentine laid down |
| Apply calcium hydroxide or Biodentine as base | Place definitive restoration |
| Seal with GIC | Verify no pulp exposure |
- Why it works: Sealing caries stimulates odontoblasts to lay down tertiary/reactionary dentine, increasing pulp-to-caries distance
- Modern alternative: Single-visit partial caries removal (selective caries removal to firm dentine) - ICCMS guidelines
9. SELECTIVE CARIES REMOVAL (ICCMS Guidelines - 2019)
- Replaces the old concept of "complete caries removal"
- Based on dentine hardness and proximity to pulp:
| Zone | Dentine Type | Action |
|---|---|---|
| Periphery of cavity | Soft/infected | Remove completely |
| Pulpal wall (deep) | Firm/affected | Leave in situ if near pulp |
- Selective to firm dentine: For shallow-moderate lesions
- Selective to soft dentine: For deep lesions near pulp (then seal)
- Reduces pulp exposure risk significantly
10. SONOABRASION
- Uses ultrasonic oscillating tips (not rotating burs) to remove caries
- Produces less heat, vibration, and noise than conventional drilling
- Tips are shaped like inverted cones or chisel tips
- Useful for tight proximal areas and tunnel preparations
- More conservative than rotary instruments
11. PAPACARIE (Enzymatic Caries Removal)
- Active agent: Papain enzyme (from papaya) + Chloramine + Toluidine blue
- Mechanism: Papain selectively digests denatured (infected) collagen in carious dentine; does NOT affect intact (sound) collagen
- Procedure: Apply gel, wait 30-60 sec, remove softened dentine with blunt excavator; repeat
- Advantages: Selective, painless, no drilling, low cost, no anesthesia needed
- Limitations: Multiple applications needed; less effective for enamel caries
12. PREVENTIVE RESIN RESTORATION (PRR)
- Introduced by Simonsen (1978) - one of earliest MID techniques
- Indication: Pit and fissure caries with minimal enamel involvement
- Technique:
- Air abrasion or small bur removes minimal carious enamel
- Composite resin placed only in the carious portion
- Remaining pits and fissures sealed with sealant
- Types: Type A (sealant only), Type B (small composite + sealant), Type C (larger composite + sealant)
- Maximally preserves tooth structure while treating and preventing caries
13. GLASS IONOMER CEMENT (GIC) IN MID
GIC is the preferred restorative material for MID because:
| Property | Significance |
|---|---|
| Fluoride release & recharge | Continuous remineralization; "slow release fluoride" |
| Chemical adhesion to dentine & enamel | No mechanical retention needed - preserves tooth structure |
| Biocompatibility | No pulpal irritation |
| Thermal expansion similar to tooth | Minimal stress at margins |
| Antibacterial activity | Inhibits S. mutans growth |
| Hydrophilic | Works in moist conditions (field settings) |
- RMGIC (Resin-Modified GIC): Improved aesthetics and strength; used in ART
- High-viscosity GIC: Stronger; used in ART for posterior teeth (Fuji IX, Ketac Molar)
14. REMINERALIZING AGENTS
a) Fluoride (multiple delivery systems)
- Fluoride varnish (5% NaF): 22,600 ppm F; applied every 3-6 months
- Fluoride toothpaste: 1000-1450 ppm F daily use
- Mechanism: Fluorapatite formation - more acid resistant than hydroxyapatite
b) CPP-ACP (Casein Phosphopeptide - Amorphous Calcium Phosphate)
- Trade name: Recaldent (in GC Tooth Mousse)
- CPP acts as a carrier that stabilizes ACP at the tooth surface
- ACP provides Ca2+ and PO4³- for remineralization
- Effective for white spot lesions, root caries, post-orthodontic demineralization
c) Self-Assembling Peptides (P11-4 / Curodont)
- Synthetic peptide matrix that assembles into scaffold at caries site
- Attracts calcium and phosphate - biomimetic enamel regeneration
- Applied non-invasively; promotes remineralization of ICDAS 1-2 lesions
d) Bioactive Glass (Novamin - SrSiO2 + CaO + Na2O + P2O5)
- Releases calcium, sodium, phosphate when in contact with water
- Forms hydroxyapatite layer on tooth surface
- Used in toothpastes (Sensodyne Repair & Protect)
15. CARIES RISK ASSESSMENT (CRA) - CAMBRA PROTOCOL
CAMBRA = Caries Management By Risk Assessment
| Risk Factor | Low Risk | High Risk |
|---|---|---|
| Past caries experience | No new cavities >3 yrs | New cavity every year |
| Visible plaque / poor OH | No | Yes |
| Saliva flow | Normal | Reduced (xerostomia) |
| Diet | Non-cariogenic | High sugar/acid frequency |
| Fluoride exposure | Daily | None |
| Social factors | - | Low SES, no dental access |
- Low risk: Preventive measures + annual recall
- Moderate risk: Fluoride varnish + dietary advice + 6-monthly recall
- High risk: SDF + ART + intensive fluoride + 3-monthly recall
16. HISTORICAL TIMELINE OF MID
| Year | Development |
|---|---|
| 1970s | Silver Diamine Fluoride introduced |
| 1978 | Preventive Resin Restoration (Simonsen) |
| 1980s | ART developed (WHO, South Africa) |
| 1990s | Chemomechanical removal (Carisolv) |
| 1990s | Air abrasion re-emergence |
| 2000s | Ozone therapy (HealOzone) |
| 2000s | DIAGNOdent widely used |
| 2010s | Resin Infiltration (ICON) |
| 2019 | ICCMS selective caries removal guidelines |
17. COMPARISON TABLE: Conventional vs. Minimally Invasive Approach
| Feature | G.V. Black (Conventional) | Minimally Invasive |
|---|---|---|
| Philosophy | "Extension for prevention" | "Prevention of extension" |
| Cavity design | Predetermined outline forms | Lesion-guided |
| Tissue removal | Removes infected + affected | Removes only infected dentine |
| Retention | Mechanical undercuts | Adhesive bonding |
| Material | Amalgam | Composite / GIC |
| Aim | Restore function | Restore + preserve biology |
| Recurrence | Cavity enlarged at each replacement | Repair, not full replacement |
18. ADHESIVE DENTISTRY - Foundation of MID
- Modern MID relies entirely on adhesive (bonded) restorations
- Composites and GICs bond chemically/micromechanically to enamel and dentine
- No need for mechanical retention (no undercuts, no resistance/retention form)
- This allows very small, conservative cavity designs
- Total-etch, self-etch, and universal adhesives used based on substrate
EXAMINER'S TIPS - How to score full 25 marks:
- Definition - must include FDI's definition (2 marks)
- Principles - ICDAS, remineralization, CRA, repair vs replace (4 marks)
- Procedures - min. 6-8 procedures with mechanisms + diagrams (12 marks)
- Biomaterials - GIC, CPP-ACP, SDF, ICON (4 marks)
- Comparison table - conventional vs MID (2 marks)
- Neat presentation - diagrams, labels, arrows (1 mark)
This is a shared conversation. Sign in to Orris to start your own chat.