Told me everything about abg , compensation,acid - based correction
Reading File
Finding Sources
Finding Sources
Searching the Web
ABG interpretation acid base compensation correction 2024 clinical guide
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
How to check compensation status of abg
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all four compensation formulas with their interpretation rules. Here is the complete, organized answer:
How to Check Compensation Status on an ABG
The core principle: identify the primary disorder first, then apply the matching compensation formula. Calculate the expected value of the compensating parameter and compare it to the measured value. The result tells you whether compensation is appropriate (simple disorder), insufficient (mixed disorder), or excessive (mixed disorder).
Step-by-Step Logic
1. Identify primary disorder (from pH + the changed parameter)
2. Apply the compensation formula → get the EXPECTED value
3. Compare EXPECTED vs MEASURED
- MEASURED = EXPECTED → Appropriate compensation (simple disorder)
- MEASURED > EXPECTED → Additional acidifying process present
- MEASURED < EXPECTED → Additional alkalinizing process present
The 4 Primary Disorders & Their Compensation Formulas
1. Metabolic Acidosis
Primary change: pH ↓, HCO3- ↓
Compensates via: Lungs hyperventilate → CO2 blown off → PaCO2 ↓
Formula - Winter's Formula:
Expected PaCO2 = (1.5 × [HCO3-]) + 8 ± 2
| Measured PaCO2 vs Expected | Interpretation |
|---|---|
| Measured PaCO2 = Expected | Appropriate respiratory compensation (simple metabolic acidosis) |
| Measured PaCO2 > Expected | Concomitant respiratory acidosis (not blowing off enough CO2) |
| Measured PaCO2 < Expected | Concomitant respiratory alkalosis (blowing off too much CO2) |
Example: HCO3- = 14 mEq/L
Expected PaCO2 = (1.5 × 14) + 8 = 21 + 8 = 29 ± 2 mm Hg
- If measured PaCO2 = 29 → simple metabolic acidosis ✓
- If measured PaCO2 = 38 → mixed metabolic acidosis + respiratory acidosis
- If measured PaCO2 = 20 → mixed metabolic acidosis + respiratory alkalosis
2. Metabolic Alkalosis
Primary change: pH ↑, HCO3- ↑
Compensates via: Lungs hypoventilate → CO2 retained → PaCO2 ↑
Formula:
Expected PaCO2 = 0.7 × ([HCO3-] − 24) + 40 ± 2
| Measured PaCO2 vs Expected | Interpretation |
|---|---|
| Measured PaCO2 = Expected | Appropriate respiratory compensation (simple metabolic alkalosis) |
| Measured PaCO2 > Expected | Concomitant respiratory acidosis |
| Measured PaCO2 < Expected | Concomitant respiratory alkalosis |
Example: HCO3- = 34 mEq/L
Expected PaCO2 = 0.7 × (34 - 24) + 40 = 7 + 40 = 47 ± 2 mm Hg
3. Respiratory Acidosis
Primary change: pH ↓, PaCO2 ↑
Compensates via: Kidneys retain HCO3- → HCO3- ↑
(Kidney compensation is slow - takes 3-5 days, so acute vs chronic distinction is critical)
Formula:
Acute: For every ↑10 mm Hg in PaCO2 above 40 → HCO3- ↑ by 1 mEq/L
Chronic: For every ↑10 mm Hg in PaCO2 above 40 → HCO3- ↑ by 4-5 mEq/L
| Measured HCO3- vs Expected | Interpretation |
|---|---|
| Measured HCO3- = Expected | Appropriate compensation |
| Measured HCO3- > Expected | Concomitant metabolic alkalosis |
| Measured HCO3- < Expected | Concomitant metabolic acidosis |
Example (acute): PaCO2 = 60 mm Hg (↑20 above 40)
Expected HCO3- increase = 20/10 × 1 = 2 mEq/L → Expected HCO3- = 24 + 2 = 26 mEq/L
Example (chronic): PaCO2 = 60 mm Hg
Expected HCO3- increase = 20/10 × 4-5 = 8-10 mEq/L → Expected HCO3- = 32-34 mEq/L
4. Respiratory Alkalosis
Primary change: pH ↑, PaCO2 ↓
Compensates via: Kidneys excrete HCO3- → HCO3- ↓
Formula:
Acute: For every ↓10 mm Hg in PaCO2 below 40 → HCO3- ↓ by 2 mEq/L
Chronic: For every ↓10 mm Hg in PaCO2 below 40 → HCO3- ↓ by 4-5 mEq/L
| Measured HCO3- vs Expected | Interpretation |
|---|---|
| Measured HCO3- = Expected | Appropriate compensation |
| Measured HCO3- > Expected | Concomitant metabolic alkalosis |
| Measured HCO3- < Expected | Concomitant metabolic acidosis |
Example (acute): PaCO2 = 20 mm Hg (↓20 below 40)
Expected HCO3- decrease = 20/10 × 2 = 4 mEq/L → Expected HCO3- = 24 - 4 = 20 mEq/L
Quick Reference Summary Table
| Primary Disorder | Compensating Organ | Parameter That Changes | Formula |
|---|---|---|---|
| Metabolic Acidosis | Lungs | PaCO2 ↓ | PaCO2 = (1.5 × HCO3-) + 8 ± 2 |
| Metabolic Alkalosis | Lungs | PaCO2 ↑ | PaCO2 = 0.7 × (HCO3- - 24) + 40 ± 2 |
| Respiratory Acidosis (acute) | Kidneys | HCO3- ↑ | +1 mEq/L per ↑10 mm Hg CO2 |
| Respiratory Acidosis (chronic) | Kidneys | HCO3- ↑ | +4-5 mEq/L per ↑10 mm Hg CO2 |
| Respiratory Alkalosis (acute) | Kidneys | HCO3- ↓ | -2 mEq/L per ↓10 mm Hg CO2 |
| Respiratory Alkalosis (chronic) | Kidneys | HCO3- ↓ | -4-5 mEq/L per ↓10 mm Hg CO2 |
Key Rules to Remember
- Compensation never fully corrects pH - the pH always stays on the side of the primary disorder. If the pH is fully normal, suspect a mixed disorder.
- Metabolic disorders are compensated by the lungs (fast - minutes to hours).
- Respiratory disorders are compensated by the kidneys (slow - 3-5 days for full chronic compensation).
- Acute vs chronic matters only for respiratory disorders - the degree of expected renal compensation differs significantly.
- If measured compensation is more than expected → a second alkalinizing process is present alongside.
- If measured compensation is less than expected → a second acidifying process is present alongside.
Source: Frameworks for Internal Medicine; Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
Show how to identify mixed acid-base disorders
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
All the data I need is in hand. Here is the complete, organized answer:
Identifying Mixed Acid-Base Disorders
A mixed disorder exists when two or more primary acid-base disturbances are present simultaneously - not just compensation for one. There are four tools to detect them.
The Gold Standard Nomogram (Harrison's, 2025)
The blue zones below represent the 90% confidence limits of normal compensation for each simple disorder. Any ABG that plots outside these zones is a mixed disorder.
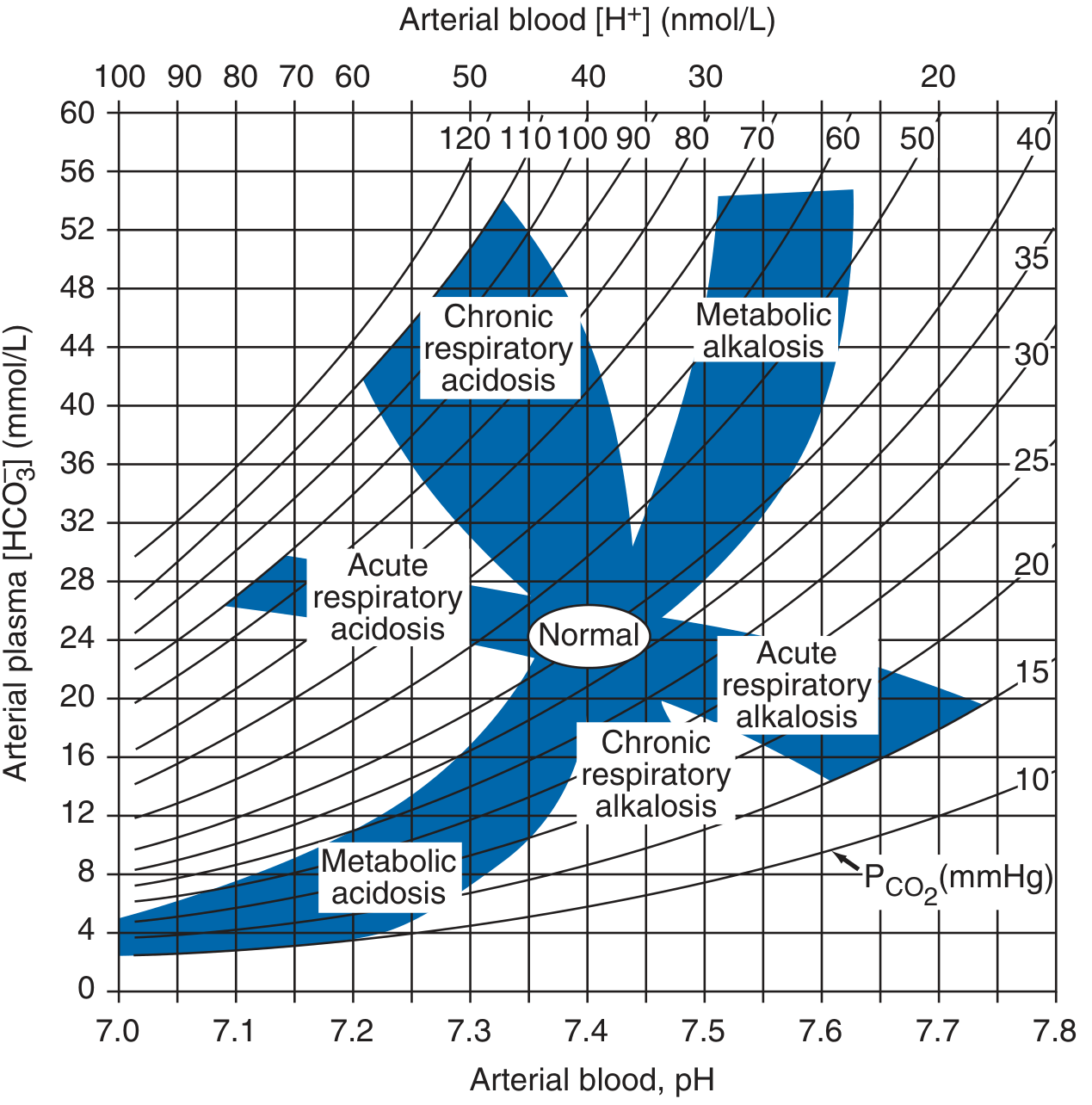
If your ABG falls in the white space between zones, you have a mixed disorder.
4 Detection Tools - Use All of Them Systematically
Tool 1: The Opposite-Direction Rule (Quick Screen)
"PaCO2 and HCO3- always change in the SAME direction in simple disorders (compensation). If they move in OPPOSITE directions, a mixed disorder is present by definition."
- Morgan & Mikhail's Clinical Anesthesiology, 7e
| PaCO2 | HCO3- | Meaning |
|---|---|---|
| ↑ | ↑ | Same direction - could be simple (respiratory acidosis + renal compensation) |
| ↓ | ↓ | Same direction - could be simple (respiratory alkalosis + renal compensation) |
| ↑ | ↓ | OPPOSITE - always mixed (respiratory acidosis + metabolic acidosis) |
| ↓ | ↑ | OPPOSITE - always mixed (respiratory alkalosis + metabolic alkalosis) |
Tool 2: Compare Measured vs Expected Compensation
After identifying the primary disorder, apply the formula. If the measured value is outside the expected range, a second primary process is present.
| Primary Disorder | Formula | If Measured > Expected | If Measured < Expected |
|---|---|---|---|
| Metabolic Acidosis | PaCO2 = (1.5 × HCO3-) + 8 ± 2 | + Respiratory acidosis | + Respiratory alkalosis |
| Metabolic Alkalosis | PaCO2 = 0.7 × (HCO3- - 24) + 40 ± 2 | + Respiratory acidosis | + Respiratory alkalosis |
| Resp. Acidosis (acute) | HCO3- ↑ 1 mEq/L per ↑10 mmHg CO2 | + Metabolic alkalosis | + Metabolic acidosis |
| Resp. Acidosis (chronic) | HCO3- ↑ 4-5 mEq/L per ↑10 mmHg CO2 | + Metabolic alkalosis | + Metabolic acidosis |
| Resp. Alkalosis (acute) | HCO3- ↓ 2 mEq/L per ↓10 mmHg CO2 | + Metabolic alkalosis | + Metabolic acidosis |
| Resp. Alkalosis (chronic) | HCO3- ↓ 4-5 mEq/L per ↓10 mmHg CO2 | + Metabolic alkalosis | + Metabolic acidosis |
Tool 3: The Delta-Delta Ratio (ΔΔ) - Used in High Anion Gap Acidosis
When a high anion gap (AG) metabolic acidosis is confirmed, calculate the ΔΔ to see if another metabolic disorder is hiding underneath.
ΔΔ = ΔAG / ΔHCO3-
= (Measured AG - 12) / (24 - Measured HCO3-)
| ΔΔ Value | Interpretation |
|---|---|
| < 1.0 | Mixed: AG metabolic acidosis + non-AG (hyperchloremic) metabolic acidosis |
| 1 - 2 | Pure high AG metabolic acidosis |
| > 2.0 | Mixed: AG metabolic acidosis + metabolic alkalosis (or compensated chronic respiratory acidosis) |
Why it works: In a pure AG acidosis, every 1 mEq/L rise in AG corresponds to a 1 mEq/L fall in HCO3-. If HCO3- hasn't dropped as much as the AG rose (ΔΔ > 2), the baseline HCO3- was already high (metabolic alkalosis coexisting). If HCO3- dropped more than expected (ΔΔ < 1), there is an additional source of HCO3- loss.
Tool 4: The pH Clue - When pH is Normal But Parameters Are Abnormal
A normal pH with abnormal PaCO2 and HCO3- is a red flag for a mixed disorder, especially one where acidosis and alkalosis are cancelling each other out.
Always calculate the AG even when pH is normal - a hidden high AG acidosis may be masked by a coexisting metabolic alkalosis.
Common Clinical Mixed Disorders
| Clinical Scenario | Mixed Disorder | Clue |
|---|---|---|
| Cardiac arrest | Respiratory acidosis + Metabolic acidosis | PaCO2 ↑, HCO3- ↓ (opposite directions) |
| Septic shock | Respiratory alkalosis + Metabolic acidosis (lactic) | pH may be near normal, but both abnormal |
| DKA + vomiting | AG metabolic acidosis + Metabolic alkalosis | ΔΔ > 2, HCO3- higher than expected for AG rise |
| COPD + diuretics | Respiratory acidosis + Metabolic alkalosis | HCO3- higher than expected for chronic compensation |
| Salicylate OD | Respiratory alkalosis + Metabolic acidosis | Stimulates respiratory center AND generates organic acids |
| Renal failure + NG drainage | Metabolic acidosis + Metabolic alkalosis | pH may appear near-normal; AG elevated |
| Liver failure | Respiratory alkalosis + any developing disorder | Hepatic encephalopathy drives hyperventilation |
Worked Example: DKA + Vomiting
ABG: pH 7.35 | PaCO2 38 mmHg | HCO3- 15 mEq/L | Na 140 | Cl 90
Step 1 - Primary disorder: pH ↓ with HCO3- ↓ → metabolic acidosis
Step 2 - AG: 140 - (90 + 15) = 35 mEq/L (markedly elevated - high AG acidosis)
Step 3 - Check compensation (Winter's): Expected PaCO2 = (1.5 × 15) + 8 = 30.5 ± 2 mmHg
- Measured PaCO2 = 38 mmHg > 32.5 → concomitant respiratory acidosis (not compensating adequately) Step 4 - ΔΔ: (35 - 12) / (24 - 15) = 23/9 = 2.6 → > 2.0
- This means a metabolic alkalosis is also present (from vomiting) that raised baseline HCO3-
Final interpretation: Triple disorder - High AG metabolic acidosis + Metabolic alkalosis (vomiting) + Respiratory acidosis (inadequate ventilation)
This is clinically the diabetic vomiting case described in Fishman's Pulmonary Diseases and Disorders - the unmeasured anion concentration added to plasma HCO3- gives a value >30 mEq/L, proving a pre-existing alkalosis.
Key Rules Summary
- Compensation never overshoots - if pH is fully corrected or swings past normal, it is mixed.
- PaCO2 and HCO3- in opposite directions = always mixed.
- Always calculate the AG, even with a normal pH - a hidden mixed disorder may be present.
- Use ΔΔ whenever you find a high AG acidosis - a second metabolic disorder is frequently hiding.
- Clinical context is essential - vomiting, renal failure, liver disease, sepsis, and certain toxins classically produce specific mixed patterns.
Sources: Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22e (2025); Morgan & Mikhail's Clinical Anesthesiology 7e; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.