1. Define osteomyelitis. Discuss it's etiology pathogenesis morphology and complications. 2.describe Acute pyogenic osteomyelitis with reference to sequestrum and invulcrum 3.Discuss clinicopathological features of chronic osteomyelitis.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and images needed. Let me compose a comprehensive, well-structured answer.
Osteomyelitis - Comprehensive Pathology Notes
1. Definition, Etiology, Pathogenesis, Morphology, and Complications
Definition
Osteomyelitis is inflammation of bone and bone marrow, virtually always secondary to infection. It may arise as a complication of any systemic infection but frequently presents as a primary solitary focus. All types of organisms - viruses, parasites, fungi, and bacteria - can cause osteomyelitis, but pyogenic bacteria and mycobacteria are by far the most common.
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
Etiology
Organisms reach bone by three main routes:
| Route | Details |
|---|---|
| Hematogenous spread | Most common in children; bacteremia from trivial mucosal injuries or minor skin infections seeds the metaphysis |
| Extension from a contiguous site | Direct spread from adjacent infected soft tissue or joint |
| Direct implantation | Compound fractures, orthopedic surgery, penetrating trauma |
Causative organisms by context:
- Staphylococcus aureus - responsible for 80-90% of culture-positive pyogenic osteomyelitis; staphylococcal cell wall proteins bind bone matrix components (e.g., collagen), facilitating adherence
- Neonates - group B Streptococci and E. coli
- Older children - gram-positive organisms, predominantly S. aureus
- Sickle cell disease - Salmonella and gram-negative organisms (areas of bone infarction serve as a bacterial nidus; loss of splenic function impairs immune response)
- Open fractures / surgical sites - mixed bacterial infections
- Diabetic foot - polymicrobial; gram-negative and anaerobic organisms more common
- Note: No organism is identified in approximately 50% of cases
Pathogenesis
The pathogenesis is governed by the vascular anatomy of bone, which changes with age:
Step-by-step sequence:
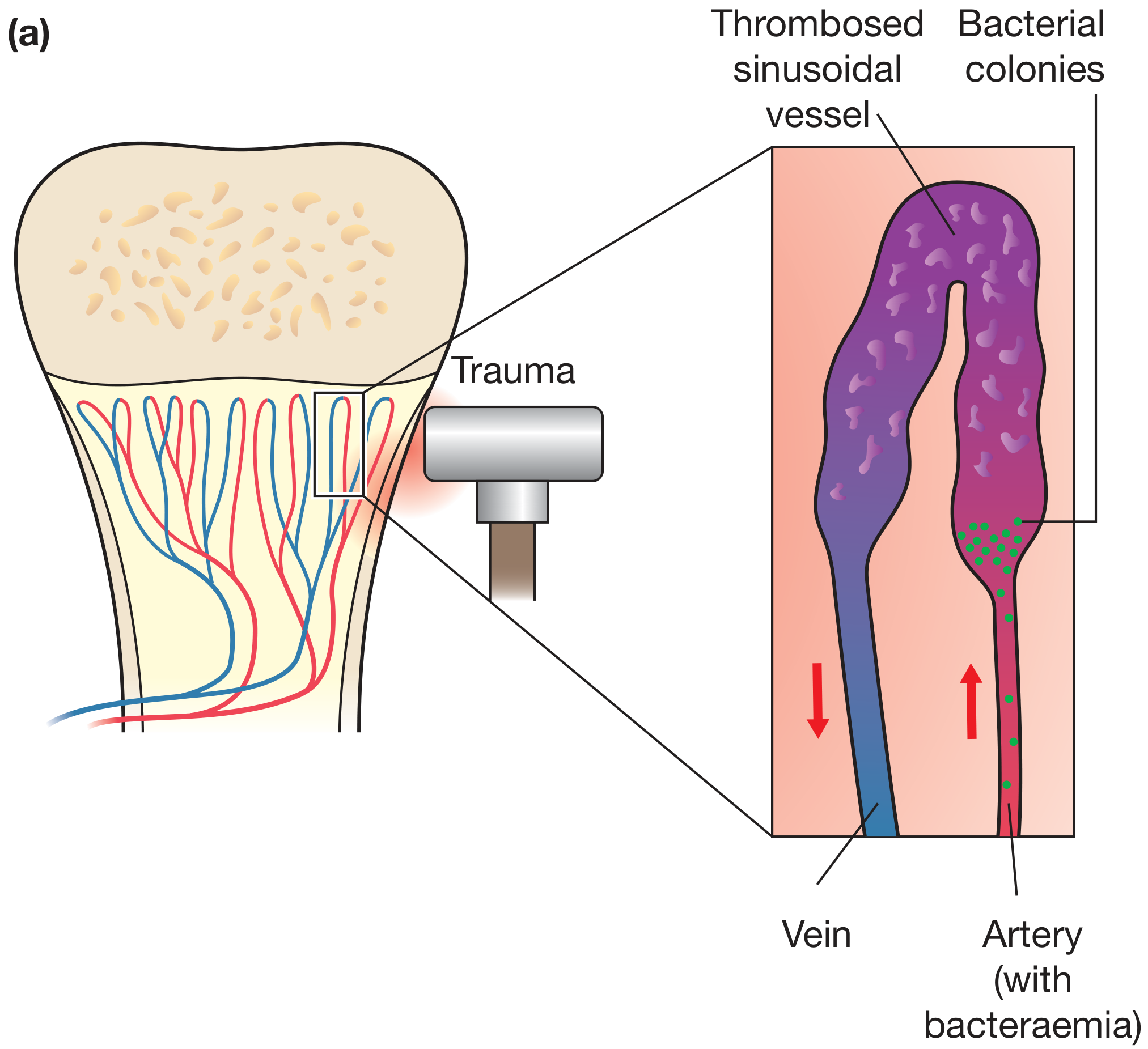
- Bacteraemia seeds the metaphysis - in children, the looped sinusoidal vessels of the metaphysis have slow blood flow and are susceptible to bacterial trapping, especially after microtrauma
- Bacteria proliferate and trigger an acute neutrophilic inflammatory response
- Bone and marrow necrosis occurs within the first 48 hours
- Bacteria and inflammation spread longitudinally and radially through Haversian (osteon) canals toward the periosteum
- In children, the periosteum is loosely attached to cortex and can be stripped by the inflammatory exudate, forming a subperiosteal abscess - periosteal lifting further cuts off cortical blood supply and worsens necrosis
- Periosteal rupture creates a soft tissue abscess that may track to the skin as a draining sinus
- If infection spreads to the epiphysis or joint space, septic/suppurative arthritis results, with destruction of articular cartilage
Age-related vascular anatomy:
| Age | Vascular pattern | Consequence |
|---|---|---|
| Neonate | Metaphyseal vessels penetrate growth plate | Infection of metaphysis, epiphysis, or both; easy joint spread |
| Children | Metaphyseal vessels end at growth plate | Metaphyseal focus is typical |
| Adults | Growth plate closure creates metaphyseal-epiphyseal anastomoses | Epiphyseal and subchondral involvement more common |
Morphology
Changes depend on the stage (acute, subacute, chronic) and location of infection.
Acute Phase (first 48 hours)
- Bacteria proliferate in marrow
- Neutrophilic infiltrate - the hallmark of acute inflammation
- Necrosis of osteocytes and marrow fat/hematopoietic elements within 48 hours
- Spread through Haversian canals to the periosteum
- Subperiosteal abscess formation
- Pus may decompress through cortical bone and elevator the periosteum
Subacute/Evolving Phase (after first week)
- Chronic inflammatory cells (lymphocytes, plasma cells, macrophages) are recruited
- Cytokines released → stimulate osteoclastic bone resorption, fibrous tissue ingrowth, and deposition of reactive woven bone at the periphery
Chronic Phase
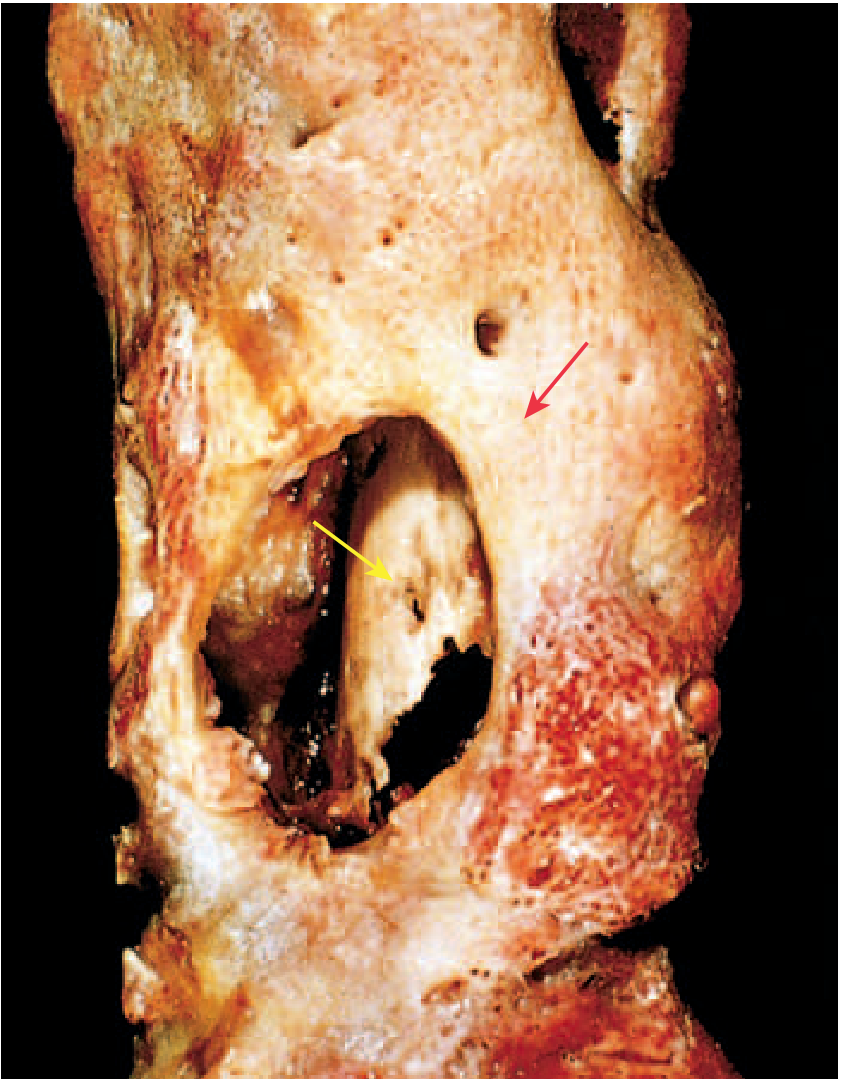
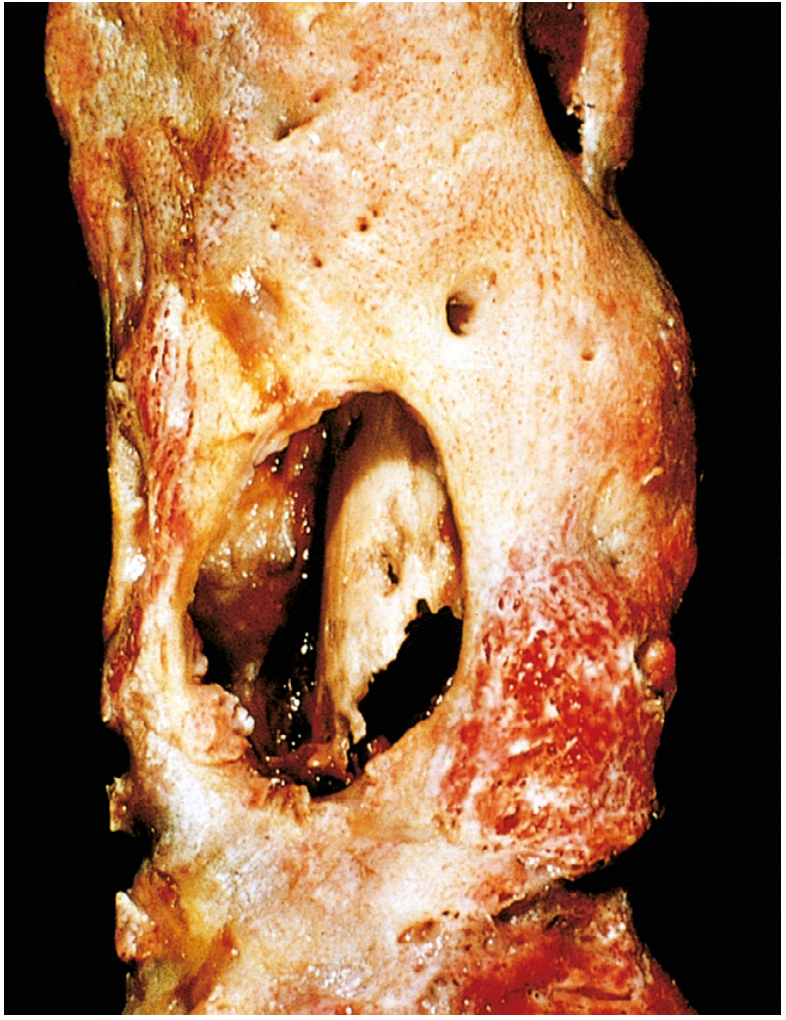
- Sequestrum: the fragment of dead, necrotic bone entrapped within the infected zone. It is devascularised, often yellow-white, surrounded by pus
- Involucrum: a shell of living reactive (subperiosteal) new bone deposited around the devitalised, infected bone segment by the stripped-up periosteum. It creates the radiographic "bone-within-a-bone" appearance
- Cloaca: openings/perforations in the involucrum through which pus and bone fragments drain to the skin surface via a sinus tract
- Marrow fibrosis and chronic inflammatory infiltrate of lymphocytes and plasma cells
Gross/Histologic summary table:
| Feature | Acute | Chronic |
|---|---|---|
| Dominant cell | Neutrophils | Lymphocytes, plasma cells |
| Bone status | Necrosis beginning | Sequestrum established |
| New bone | Absent | Involucrum formed |
| Marrow | Oedema, congestion | Fibrosis |
| Sinus | May form | Often present |
Classic gross specimen:
Complications
| Complication | Mechanism |
|---|---|
| Chronic osteomyelitis | Failure of resolution in 5-25% of acute cases; associated with delayed diagnosis, extensive necrosis, inadequate debridement, or impaired immunity |
| Pathological fracture | Bone destruction and weakening |
| Septic arthritis | Spread to joint space, especially in neonates (metaphysis intracapsular) |
| Subperiosteal abscess | Pus elevates periosteum |
| Soft tissue abscess and draining sinus | Periosteal rupture and skin tract formation |
| Secondary (reactive) amyloidosis | Chronic infection drives sustained SAA production (systemic AA amyloidosis) |
| Endocarditis / sepsis | Haematogenous dissemination |
| Squamous cell carcinoma (Marjolin's ulcer) | Malignant transformation in longstanding draining sinus tracts |
| Sarcoma | Rarely, osteosarcoma or fibrosarcoma in chronically infected bone |
| Growth disturbance | In children, epiphyseal plate damage causes limb length discrepancy or deformity |
(Robbins Basic Pathology; Robbins, Cotran & Kumar PBD)
2. Acute Pyogenic Osteomyelitis - with Sequestrum and Involucrum
Definition
Acute pyogenic osteomyelitis is a rapidly evolving infection of bone and marrow caused by pyogenic bacteria, characterised by suppurative (pus-forming) inflammation and bone necrosis.
Clinical Presentation (Acute)
- Systemic illness: malaise, fever, chills, leukocytosis
- Intense throbbing pain over the affected bone
- Local warmth, swelling, and erythema
- Infants: often subtle - unexplained fever, irritability, pseudoparalysis of the limb
- Adults: may present with only localised pain; often post-fracture or post-surgical
Preferred Site
- Metaphysis of long bones (distal femur, proximal tibia, proximal humerus most common in children)
- In neonates: both metaphysis and epiphysis
- In adults: vertebral bodies (haematogenous), foot bones (diabetic)
Pathological Sequence in Acute Stage
- Bacteria seed the metaphyseal sinusoidal loops during a bacteraemia (often precipitated by microtrauma)
- Neutrophilic response - pus accumulates in the marrow cavity, raising intramedullary pressure
- Pus dissects through Haversian and Volkmann's canals to reach the periosteum
- Subperiosteal abscess forms - periosteal elevation further devascularises the cortex
- Pus may penetrate the periosteum to form a soft tissue abscess, which may then track to the skin as a sinus tract
- In children: metaphyseal infection can spread to the joint (septic arthritis)
- In neonates: the growth plate is not a barrier - epiphyseal and joint infection occur readily
Sequestrum and Involucrum
These are the two defining pathological structures of established (subacute to chronic) pyogenic osteomyelitis:
Sequestrum
- Definition: A fragment of dead, necrotic bone that has become separated from the living bone
- Mechanism: Formed as the devascularised (avascular) cortical bone undergoes necrosis; osteocytes die, the lacunae become empty, and the bone is incapable of repair
- Appearance: Dense, whitish-yellow bone fragment surrounded by pus and granulation tissue
- Significance: Acts as a persistent nidus of infection - antibiotics cannot penetrate avascular bone; this is the main reason acute osteomyelitis becomes chronic
- Histology: Necrotic bone with empty osteocyte lacunae, surrounded by neutrophils
Involucrum
- Definition: A sheath of new reactive bone formed by the elevated periosteum around the sequestrum
- Mechanism: Periosteal stripping is a potent stimulus for osteoblastic new bone formation. The stripped periosteum deposits a cuff of woven bone (the involucrum) around the infected, necrotic segment
- Appearance: Thick, irregular shell of new bone encasing the sequestrum
- Cloaca: Perforations in the involucrum through which pus and sequestrum fragments are extruded via sinus tracts
- Significance: The involucrum represents the body's attempt to wall off infection; together with the sequestrum it creates the classic radiographic "bone-within-a-bone" appearance
Visual summary:
Investigations
- Blood: Leucocytosis, raised ESR and CRP; blood cultures (positive in ~50%)
- Plain X-ray: Often normal in first 10-14 days; later shows lytic destruction, periosteal reaction, reactive sclerosis
- MRI: Most sensitive and specific; detects marrow oedema early; imaging of choice
- CT: Excellent for defining sequestrum, involucrum, and cortical destruction in established disease
- Bone scan (Tc-99m): Sensitive; useful when MRI is unavailable
- Biopsy + culture: Gold standard for identifying the organism
3. Chronic Osteomyelitis - Clinicopathological Features
Definition
Chronic osteomyelitis is a persistent, longstanding bone infection that develops when acute osteomyelitis fails to resolve - occurring in 5-25% of acute cases. It is characterised by the triad of: sequestrum, involucrum, and draining sinus.
Predisposing Factors for Chronicity
- Delayed diagnosis or inadequate initial treatment
- Extensive bone necrosis (large sequestrum)
- Poor host immunity (diabetes, malnutrition, sickle cell disease, immunosuppression)
- Inadequate surgical debridement
- Antibiotic-resistant organisms (e.g., MRSA with Panton-Valentine leukocidin gene)
Clinicopathological Features
Symptoms and Signs
| Feature | Description |
|---|---|
| Pain | Dull, persistent aching in the affected limb; may flare acutely |
| Swelling | Chronic oedema and periosteal thickening; limb may appear enlarged |
| Discharging sinus | Chronic purulent or seropurulent discharge; may close and re-open |
| Systemic features | Usually low-grade or absent; fever during acute exacerbations |
| Muscle wasting | Disuse atrophy of surrounding muscles |
| Pathological fracture | Due to cortical destruction and weakening |
| Limb deformity | If physis damaged in childhood |
Clinical Course
- Typically punctuated by episodes of acute flare after periods of relative quiescence, sometimes after years of dormancy
- Acute exacerbations triggered by: immunosuppression, trauma, or minor illness
Pathological Features
Macroscopic:
- Sequestrum: Devitalised bone, may be large or fragmented; surrounded by pus
- Involucrum: Thick shell of new woven/lamellar bone encasing the sequestrum
- Cloaca: Multiple holes in the involucrum
- Sinus tract(s): Chronic, epithelium-lined tracts draining to the skin surface
- Surrounding soft tissue scarring and fibrosis
Microscopic/Histological:
- Marrow space replaced by fibrosis
- Chronic inflammatory infiltrate: lymphocytes, plasma cells, macrophages
- Necrotic bone (sequestrum) with empty osteocyte lacunae
- Reactive woven bone formation (involucrum)
- Granulation tissue
- Absence of the neutrophilic infiltrate that dominates the acute phase
- Occasionally, Brodie's abscess: a well-circumscribed subacute abscess in the metaphysis, surrounded by sclerotic bone - a contained form seen most often with S. aureus in children
Radiological Features
- Dense, sclerotic bone surrounding the sequestrum
- Cortical thickening (periosteal new bone = involucrum)
- Intraosseous cavity containing sequestrum ("bone within bone")
- Draining sinus tract may be visible on fistulography
- MRI: low signal on T1, high on T2/STIR (oedema and active infection); enhancement with contrast
- CT: superior for quantifying extent of sequestrum
Complications of Chronic Osteomyelitis
- Pathological fracture - cortical erosion weakens the bone
- Squamous cell carcinoma (Marjolin's ulcer) - malignant transformation of the sinus tract epithelium after decades of chronic irritation
- Secondary (AA) amyloidosis - longstanding chronic infection drives sustained amyloid A protein deposition in kidney, liver, spleen; causes nephrotic syndrome and renal failure
- Sepsis / bacteraemia - haematogenous seeding from the bone focus
- Endocarditis - seeding of heart valves
- Sarcoma - very rare osteosarcoma or fibrosarcoma in the infected bone
- Joint destruction / ankylosis - spread to adjacent joint
- Growth disturbance in children - physeal damage causing shortening or angular deformity
Quick Reference Summary
| Feature | Acute Osteomyelitis | Chronic Osteomyelitis |
|---|---|---|
| Onset | Sudden | Insidious |
| Symptoms | Fever, chills, systemic illness | Low-grade, recurrent exacerbations |
| Dominant cell | Neutrophils | Lymphocytes, plasma cells |
| Bone | Necrosis beginning | Sequestrum present |
| New bone | Absent | Involucrum formed |
| Sinus | May develop | Usually present |
| Key complication | Septic arthritis | SCC in sinus, amyloidosis |
| Treatment | Antibiotics ± drainage | Antibiotics + surgical debridement (sequestrectomy) |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), Chapter 26
- Robbins & Kumar Basic Pathology (11th ed.), Chapter 19
- Bailey & Love's Short Practice of Surgery (28th ed.), Chapter 44
This is a shared conversation. Sign in to Orris to start your own chat.