Sma thrombosis explain in full detail and also operative management and post op care and complications
Reading File
Finding Sources
Finding Sources
Searching PubMed
"superior mesenteric artery" AND "thrombosis" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive material from three authoritative textbooks. Let me deliver the full detailed answer.
Superior Mesenteric Artery (SMA) Thrombosis - Complete Review
1. Definition and Overview
SMA thrombosis (also called acute mesenteric arterial occlusive disease) is an acute surgical emergency caused by thrombotic occlusion of the superior mesenteric artery, resulting in ischemia and potentially infarction of the bowel supplied by the SMA. It accounts for more than 50% of all cases of acute mesenteric ischemia, making it the single most common cause.
2. Vascular Anatomy (Relevant to SMA)
The SMA arises from the aorta at approximately L1 and supplies:
- Distal duodenum
- Entire small bowel (jejunum and ileum)
- Cecum, ascending colon, and right half of transverse colon (proximal colon)
Key collateral connections:
- Pancreaticoduodenal arcade - connects celiac axis to SMA (superior PD from celiac + inferior PD from SMA)
- Marginal artery of Drummond - runs along the mesenteric border connecting SMA and IMA
- Arc of Riolan (meandering mesenteric artery) - connects SMA and IMA at the base of mesentery
The splenic flexure and descending colon have limited collaterals, creating "watershed" areas vulnerable during low-flow states. In contrast, the stomach, duodenum, and rectum have rich collaterals and are more resistant.
3. Pathophysiology
Under normal conditions:
- Intestinal blood flow = ~10% of cardiac output at rest
- Increases to 25% postprandially
- The bowel can withstand a 75% reduction in blood flow for up to 12 hours
Sequence of injury in SMA thrombosis:
- Thrombosis on pre-existing atherosclerotic plaque near the SMA origin causes sudden occlusion
- Initial compensatory mechanisms activate (collateral dilation, increased oxygen extraction)
- After several hours: splanchnic vasoconstriction develops, reducing collateral efficacy
- Mucosal sloughing begins within 3 hours of onset
- Full-thickness intestinal infarction by 6 hours
- Reperfusion injury (if revascularization achieved): mediated by oxygen free radicals, reduced nitric oxide synthesis, neutrophil infiltration, endothelial inflammation
- Loss of mucosal barrier integrity allows digestive enzyme penetration (autodigestion) and bacterial translocation
- Eventual bowel necrosis, peritonitis, septic shock, multi-organ failure
Key difference from embolism:
- Embolism lodges distally (at middle colic artery origin), more sudden onset
- Thrombosis occurs proximally near the SMA origin, often on atherosclerotic disease, may have a more gradual onset over hours to days (20-50% have prior chronic mesenteric ischemia symptoms)
4. Etiology and Risk Factors
Primary cause: Atherosclerosis with superimposed acute thrombosis at the proximal SMA
Risk factors (overlap with atherosclerosis):
- Advanced age
- Smoking
- Hypertension
- Diabetes mellitus
- Hyperlipidemia
- History of coronary artery disease, peripheral arterial disease, stroke
- Prior episode of mesenteric ischemia (chronic mesenteric ischemia in 20-50%)
- Post major abdominal surgery (arterial injury)
- Hypercoagulable states (less common than for venous thrombosis)
5. Clinical Features
Symptoms
- Abdominal pain out of proportion to physical findings - the hallmark
- Pain is typically severe, colicky, periumbilical or ill-defined
- In SMA thrombosis specifically: onset may be over hours to days (vs. sudden in embolism)
- Nausea, vomiting
- Diarrhea / urgent bowel movement (forceful evacuation due to initial spastic hypermotility)
- Sitophobia (fear of eating) and weight loss if prior chronic mesenteric ischemia
- Postprandial angina history (intestinal claudication)
Signs - Early
- Abdomen soft with minimal or NO tenderness despite severe pain (characteristic)
- Normal bowel sounds initially
Signs - Late (bowel infarction)
- Abdominal distension
- Peritonitis (guarding, rebound tenderness)
- Absent bowel sounds (ileus)
- Bloody stools / melena
- Fever, tachycardia
- Shock
Special features in elderly
- Altered mental status
- Presenting symptoms may be nonspecific
- Shock and mental changes may progress over hours
6. Laboratory Findings
| Test | Significance |
|---|---|
| Leukocytosis | Infection/infarction |
| Metabolic acidosis | Tissue ischemia |
| Elevated serum lactate | Poor prognosis in NOMI; may be normal early |
| Elevated serum amylase | Can mimic pancreatitis |
| Elevated troponin I | Common; do NOT interpret as MI alone |
| Elevated D-dimer | Thrombus formation |
| Elevated intestinal fatty acid binding protein (I-FABP) | Enterocyte necrosis - most promising biomarker |
| Elevated citrulline | Reduced enterocyte mass |
Important: Normal lactate does NOT exclude diagnosis. High clinical suspicion must drive imaging.
7. Diagnosis
Imaging
Multiphasic CT Angiography (CTA) - Gold Standard
- Biphasic (arterial + venous phase) MDCT is the current gold standard
- 64-slice or higher preferred
- Sensitivity and specificity are high; early findings may be subtle
CT findings of SMA thrombosis:
- Thrombus at or near SMA origin (proximal, unlike embolism which is distal)
- Absent or diminished contrast in SMA lumen
- Bowel wall changes:
- Early: thinning, decreased mural enhancement
- Collapsed spastic loops without intraluminal gas
- Later: bowel wall thickening (edema)
- Dilated thin bowel
- Mesenteric fat stranding
- Pneumatosis intestinalis (intramural gas) - advanced ischemia, poor sign
- Portomesenteric venous gas - very poor prognosis
- Absent bowel wall enhancement - highly specific (but low sensitivity)
Conventional Angiography
- Still used, especially when therapeutic intervention is planned
- Directly guides catheter-directed therapy (thrombolysis, papaverine)
- Can diagnose AND treat in the same setting
Other imaging:
- Plain AXR: nonspecific (distended bowel, air-fluid levels, pneumatosis); normal in ~25%
- Duplex ultrasound: can detect major arterial occlusion but limited by bowel gas
- MR angiography: alternative but impractical in critically ill
- Barium studies: CONTRAINDICATED (impairs subsequent angiography)
8. Management Algorithm
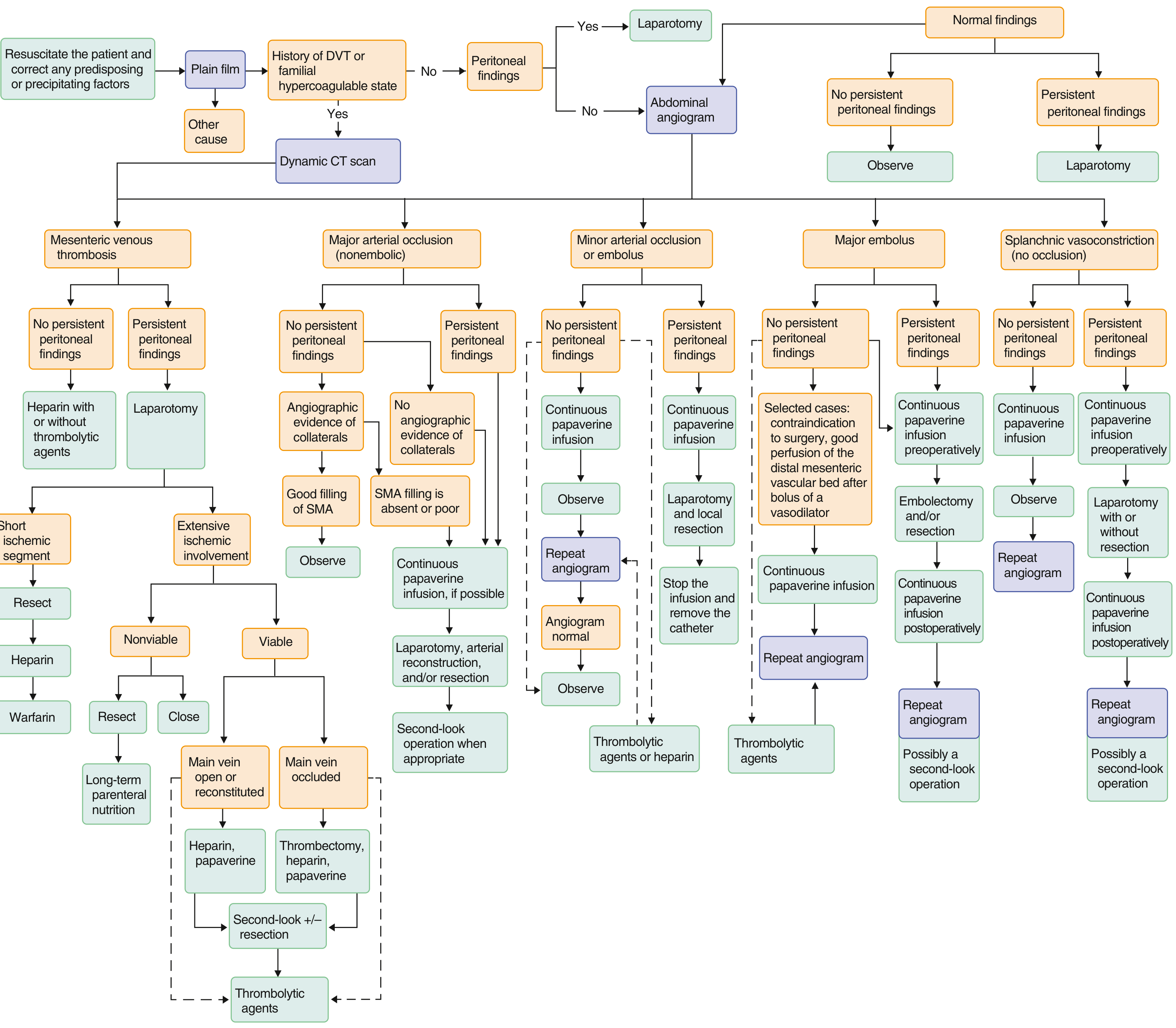
Step 1: Initial Resuscitation (IMMEDIATE)
- IV fluid resuscitation and correction of electrolyte imbalances
- Correct underlying problems: cardiopulmonary compromise, shock, renal impairment, metabolic acidosis
- Broad-spectrum IV antibiotics - bacterial translocation across ischemic bowel wall is common
- Nasogastric tube decompression
- Urinary catheter (monitor urine output)
- IV anticoagulation with heparin to prevent thrombus propagation
- Optimize cardiac output
Step 2: Diagnosis
- Urgent MDCT angiography
- If CT unavailable or indeterminate: mesenteric angiography
Step 3: Decision point - Peritoneal signs?
If peritoneal signs present → Emergency laparotomy (no delay for angiography)
If no peritoneal signs → Proceed to angiography and catheter-directed therapy first
9. Operative Management
Indications for Surgery
- Peritoneal signs at presentation (mandatory)
- Failed or not suitable for endovascular therapy
- Evidence of bowel infarction or necrosis
- Persistent or worsening symptoms despite medical/endovascular therapy
- Most patients with SMA thrombosis ultimately require surgery
Pre-operative Preparation
- Resuscitate and stabilize (correct coagulopathy, metabolic acidosis)
- IV heparin (unless contraindicated)
- Broad-spectrum antibiotics (e.g., piperacillin-tazobactam or cefuroxime + metronidazole)
- Papaverine infusion via angiographic catheter if available pre-op (reduces splanchnic vasoconstriction)
- ICU-level monitoring
Surgical Approach
Midline laparotomy provides full access to the abdominal contents.
Step 1: Bowel Assessment
- Identify the extent of ischemia/infarction
- Assess viability by:
- Color (pink vs. grey/black)
- Peristalsis
- Bleeding at cut edge
- Doppler of mesenteric vessels
- Do NOT resect bowel initially if viability is uncertain - first revascularize
Step 2: Revascularization (SMA Thrombectomy and/or Bypass)
A. Surgical Thrombectomy
- Access to SMA: retract transverse colon superiorly, incise retroperitoneum at the base of transverse mesocolon
- Expose SMA at its origin (below the pancreatic neck)
- Heparinize systemically
- Apply vascular clamps proximally and distally
- Transverse or longitudinal arteriotomy at the thrombosis site
- Fogarty balloon catheter passed proximally and distally to extract thrombus
- Back-bleeding and antegrade flow assessed
- Arteriotomy closed primarily or with patch (vein or PTFE)
B. Bypass Grafting (when thrombectomy alone insufficient or primary lesion not amenable)
- Aorto-mesenteric bypass: most durable option
- Retrograde (more common in emergency - from infrarenal aorta to SMA)
- Anterograde (from supraceliac aorta to SMA - better hemodynamics but more complex)
- Conduit: saphenous vein (preferred) or prosthetic (PTFE/Dacron)
- SMA exposed at base of transverse mesocolon, proximal aorta exposed via retroperitoneal dissection
- End-to-side anastomosis to SMA distally, end-to-side or end-to-end to aorta proximally
C. Endovascular Options (selected patients without peritonitis)
- Catheter-directed thrombolysis: tPA at 0.5-1 mg/hr via catheter in vicinity of thrombus
- Aspiration thrombectomy (mechanical)
- Percutaneous transluminal angioplasty (PTA) and stenting of underlying stenosis
- Papaverine infusion: 60mg bolus then 30-60 mg/hr for 12-48 hours to relieve splanchnic vasoconstriction (adjunct, not definitive)
Step 3: Bowel Resection
- After revascularization, reassess bowel viability (allow 15-30 minutes of reperfusion)
- Resect clearly non-viable (frankly necrotic) bowel
- Leave questionably viable bowel for second-look operation
- If extensive resection required: consider damage control approach
- Resect necrotic bowel
- Delay anastomosis - perform ostomies or staple ends closed to prevent dehiscence in a severely ill, edematous patient
- Early anastomosis in ischemic bowel carries very high mortality from dehiscence
Step 4: Second-Look Laparotomy
- Planned re-exploration at 24-72 hours after initial surgery
- Indications:
- Any questionably viable bowel left at first operation
- Need to reassess anastomoses
- Ongoing clinical deterioration
- At second look: resect bowel that has progressed to necrosis; restore bowel continuity if safe
- Multiple second-look operations may be required
10. Post-Operative Care
ICU Management
- Continue monitoring in ICU (invasive arterial line, CVP/PA catheter if needed)
- Vasopressors if hemodynamically unstable (but avoid vasoconstrictors that worsen splanchnic flow - prefer norepinephrine over vasopressin when possible)
- Optimize cardiac output
- Aggressive fluid resuscitation; monitor for abdominal compartment syndrome
Anticoagulation
- IV heparin postoperatively - started as soon as surgically safe (usually within 12-24 hours)
- Transition to warfarin (target INR 2-3) for long-term anticoagulation
- Duration: typically lifelong given underlying atherosclerotic/thrombotic tendency
- Consider low-molecular-weight heparin as bridge
Antibiotics
- Continue broad-spectrum antibiotics covering Gram-negative and anaerobic organisms
- Duration guided by clinical response (typically 5-7 days minimum)
- Adjust based on culture results
Nutritional Support
- Enteral nutrition via nasojejunal tube as soon as bowel function resumes - preferred
- Total parenteral nutrition (TPN) if bowel rest required, extensive resection, or delayed anastomosis
- Short bowel syndrome is a major concern after extensive resection - requires specialist nutritional management
Papaverine / Vasodilator Infusion
- Continue intraarterial papaverine infusion postoperatively (30-60 mg/hr) to prevent/treat residual splanchnic vasoconstriction
- Maintained for 12-48 hours postoperatively in some protocols
Monitoring
- Serial abdominal examination (for peritonitis, distension)
- Monitor lactate, WBC, CRP trends
- Serial renal function (acute kidney injury common)
- Watch for abdominal compartment syndrome (measure bladder pressures)
Wound Care and Ostomy Management
- If stoma created: stoma nurse involvement
- Monitor stoma viability and function
- Plan for reversal at 3-6 months if patient stable and adequate bowel length
11. Complications
Early Complications
| Complication | Notes |
|---|---|
| Bowel infarction / re-infarction | Most feared; requires re-exploration |
| Bowel anastomotic leak | High risk due to ischemia, edema, malnutrition - reason to delay anastomosis |
| Short bowel syndrome | Massive resection (>70% small bowel loss) leads to malabsorption, diarrhea, nutritional failure |
| Reperfusion injury | After revascularization: oxygen radical-mediated injury, SIRS, multi-organ dysfunction |
| Intra-abdominal sepsis / peritonitis | From translocation or anastomotic leak |
| Multi-organ dysfunction syndrome (MODS) | From sepsis, reperfusion injury |
| Acute kidney injury | From hypoperfusion and contrast nephropathy |
| Respiratory failure / ARDS | From systemic inflammatory response |
| Coagulopathy / DIC | From massive infarction and sepsis |
| Abdominal compartment syndrome | From bowel edema post-reperfusion |
| Graft thrombosis | Early bypass failure |
| Bleeding | Anastomotic, retroperitoneal |
Late Complications
| Complication | Notes |
|---|---|
| Short bowel syndrome | Long-term TPN dependence; may require intestinal transplantation |
| Recurrent mesenteric ischemia | If underlying atherosclerosis not adequately treated |
| Anastomotic stricture | Requires endoscopic or surgical dilation |
| Adhesive small bowel obstruction | Common after any major abdominal surgery |
| Graft stenosis/occlusion | Late bypass failure; requires surveillance |
| Nutritional deficiencies | B12 (if terminal ileum resected), fat-soluble vitamins, iron |
| Incisional hernia | After midline laparotomy, especially in malnourished patients |
12. Prognosis
- Overall mortality remains high (27-60%) despite advances
- Prognosis is worse for SMA thrombosis than for embolism
- Key determinants:
- Time to diagnosis and revascularization (most critical factor)
- Extent of bowel infarction at presentation
- Patient's underlying comorbidities
- In-hospital 30-day morbidity after bowel resection: 56.6%, mortality: 27.9%
- Elderly patients have particularly poor outcomes
- Early recognition before infarction develops dramatically improves survival
13. Long-Term Prevention
- Long-term anticoagulation: warfarin (INR 2-3) or novel anticoagulants
- Antiplatelet therapy: aspirin for atherosclerosis prevention
- Control atherosclerotic risk factors aggressively (statins, antihypertensives, smoking cessation, glycemic control)
- Surveillance imaging of bypass graft (duplex ultrasound)
- Nutritional follow-up if significant bowel resected
Key Sources:
- Goldman-Cecil Medicine, 2-Volume Set (International Edition) - Chapter 129: Acute Mesenteric Ischemia
- Schwartz's Principles of Surgery, 11th Edition - Chapter 14: Mesenteric Ischemia
- Yamada's Textbook of Gastroenterology, 7th Edition - Chapter 114: Mesenteric Ischemia
This is a shared conversation. Sign in to Orris to start your own chat.