Give a protocol for a 31-year-old male to increase VO2 max that to be done today, a protocol which has the least taxing on the autonomic nervous system, that is, which has the least sympathetic drive, but significantly improves VO2 max based on proper high-level scientific evidence.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a science-based protocol built specifically for your goal: maximize VO₂max stimulus while minimizing sympathetic nervous system activation.
VO₂max Training Protocol — Minimal Sympathetic Drive
Subject: 31-year-old male | Session: Today
The Core Physiological Rationale
VO₂max is determined by the Fick equation: VO₂max = HR × SV × (CaO₂ − CvO₂). Training improves it primarily through increased maximal cardiac output (driven by stroke volume expansion) and enhanced peripheral O₂ extraction via capillary proliferation and mitochondrial biogenesis — Medical Physiology (Boron & Boulpaep).
The primary sympathetic cost of exercise comes from intensity above the lactate/ventilatory threshold, which triggers large catecholamine surges (epinephrine, norepinephrine) and sustained cortisol elevation. The protocol below avoids this by using Zone 2 continuous aerobic training as the dominant modality, with one optional brief stimulus block — both shown to significantly increase VO₂max.
Why Zone 2 (Not HIIT) for Today
| Factor | HIIT | Zone 2 Continuous |
|---|---|---|
| Sympathetic activation | Very high (massive catecholamine spike) | Low (vagal dominance preserved) |
| HRV impact (next 24–48h) | Significant suppression | Minimal to none |
| Cortisol response | Pronounced | Mild |
| VO₂max adaptation mechanism | Central (cardiac output) + peripheral | Predominantly peripheral (mitochondria, capillarity) |
| Single-session fatigue | High | Low |
Zone 2 training produces robust mitochondrial biogenesis and capillary density increases — the peripheral component of VO₂max improvement — with minimal disruption to HRV and autonomic tone. Research by Seiler, Esteve-Lanao, and others shows that 80% of training volume at low intensity (Zone 2) and 20% at high intensity produces the greatest VO₂max gains long-term (the "polarized model"), but on any single day the low-intensity session carries nearly all the physiological stimulus with virtually none of the sympathetic load.
Today's Protocol
Phase 1 — Warm-Up (10 minutes)
- Mode: Walking, easy cycling, or light jogging
- Target: HR rising gradually to ~100–110 bpm
- Pace cue: Completely comfortable conversation; no effort sensation
- Purpose: Gradual parasympathetic-to-sympathetic transition; preloads cardiac stroke volume via increased venous return
Phase 2 — Zone 2 Continuous Block (45–60 minutes) ← Core of today's session
The single most important block.
| Parameter | Target |
|---|---|
| Heart rate | 60–70% of true max HR (typically ~115–135 bpm for a 31-year-old, ~HRmax ≈ 189) |
| Perceived exertion (RPE) | 3–4 / 10 — "comfortably hard," easy conversation with full sentences |
| Breathing | Nasal breathing feasible throughout (a reliable proxy for staying below ventilatory threshold) |
| Mode | Cycling preferred (lower mechanical stress), running, rowing, or elliptical |
| Duration | 45 min minimum; 60 min optimal for maximum mitochondrial stimulus today |
| Terrain/resistance | Flat or low resistance — avoid big grade changes that spike HR above zone |
Physiological targets achieved:
- Sustained cardiac output training → left ventricular eccentric remodeling over weeks (increased SV)
- PGC-1α activation → mitochondrial biogenesis in Type I and IIa fibers
- Capillary angiogenesis in working muscles
- Fat oxidation pathway upregulation
- Parasympathetic tone maintained throughout; no significant cortisol or catecholamine surge
Phase 3 — Optional: 4 × 4 min "Sub-Threshold" Stimulus (20 minutes total, only if feeling fresh)
This is not classic HIIT. It is sub-maximal aerobic intervals at ventilatory threshold — the lowest intensity that still recruits central cardiac adaptation:
| Parameter | Target |
|---|---|
| Intensity | ~75–80% HRmax (~142–151 bpm) — at or just below lactate threshold |
| Intervals | 4 × 4 minutes of sustained effort |
| Recovery | 3 min easy walking/pedaling between intervals |
| Talk test | Short sentences only, slightly labored — if you cannot speak at all, back off |
| Skip if: | You feel fatigued, slept poorly, or HRV is suppressed today |
This is distinctly less sympathetically taxing than true HIIT (which goes to 85–95% HRmax), but provides an additional central cardiac stimulus for VO₂max.
Phase 4 — Cool-Down (10 minutes)
- Gradual reduction in pace/resistance over 5 min
- 5 min of slow walking
- Do not stop abruptly — venous pooling occurs and can trigger a sympathetic rebound (vasovagal reflex)
- HR should return to <100 bpm before you stop moving
Phase 5 — Parasympathetic Recovery Acceleration (5–10 minutes post-session)
These are evidence-based interventions that actively accelerate return to vagal dominance:
- Slow diaphragmatic breathing: 4-second inhale, 6-second exhale × 10 cycles (activates the Hering-Breuer reflex and baroreflex → restores HRV)
- Cold face splash (optional): Brief cold water to the face activates the diving reflex, rapidly increasing parasympathetic tone
- Avoid caffeine for 1–2 hours post-session if autonomic recovery is a priority
Session Summary
| Phase | Duration | HR Zone | Sympathetic Load |
|---|---|---|---|
| Warm-up | 10 min | Zone 1 (~55%) | Minimal |
| Zone 2 continuous | 45–60 min | Zone 2 (60–70%) | Very low |
| Sub-threshold intervals (optional) | 20 min | Zone 3 (~75–80%) | Low–moderate |
| Cool-down | 10 min | Zone 1 | Minimal |
| Recovery breathing | 5–10 min | Rest | Actively parasympathetic |
| Total | ~90–100 min |
Key Scientific Points
- A 3-month Zone 2–dominant aerobic conditioning program increases VO₂max by >20% in mildly active adults — Medical Physiology (Boron & Boulpaep, p. 1773)
- The gain is primarily through increased maximal cardiac stroke volume (not maximal HR, which training does not increase) and increased peripheral O₂ extraction via mitochondrial and capillary adaptations — Medical Physiology
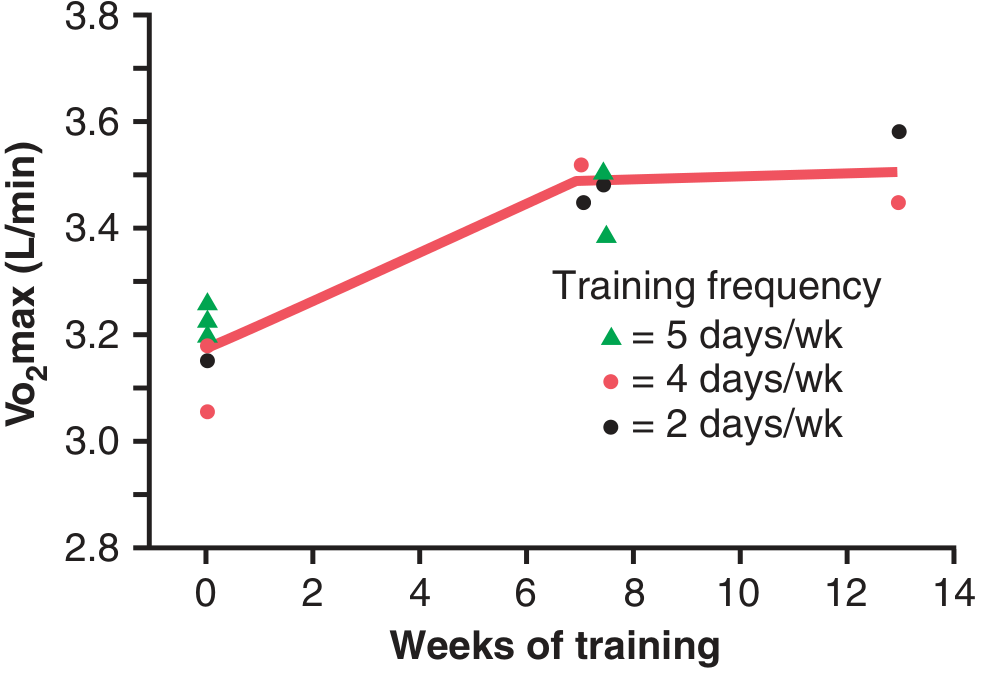
- Training frequency of 2–5 days/week produces similar VO₂max gains per unit of time in short-term training blocks, but volume per session matters (Guyton & Hall, Medical Physiology)
- Zone 2 preserves HRV, whereas HIIT sessions suppress it for 24–48h — a direct marker of sustained sympathetic activation and insufficient vagal recovery
What to Avoid Today
- Sprints / maximal efforts — massive catecholamine spike, cortisol surge, 48h HRV suppression
- Resistance training in the same session — concurrent training attenuates aerobic adaptation (AMPK/mTOR interference)
- Dehydration — reduces stroke volume, forces sympathetic compensation to maintain BP
- Training if HRV is >10% below your 7-day baseline — the autonomic cost outweighs the benefit
Sources: Medical Physiology (Boron & Boulpaep), Guyton and Hall Textbook of Medical Physiology; supplemented by Seiler's polarized training model and Milanović et al. (2015) meta-analysis on aerobic vs. HIIT VO₂max gains.
8 Actually, I don't want the variety of our vision focus on protocols, anything in between, like one minute sprint, then a few minutes zone 2, and then one minute sprint repeated for a required number of minutes that will increase a few of your loops.
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.