Hey can you give me note of normal labour for university exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have sufficient content to write a thorough, well-structured exam note. Let me now compile it.
Normal Labour - University Exam Notes
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Morgan & Mikhail's Clinical Anesthesiology; Textbook of Family Medicine
Definition
Labour is the presence of sufficient uterine contractions in frequency, intensity, and duration to bring about effacement and dilation of the cervix, ending with delivery of the baby and placenta.
- Begins at 40 ± 2 weeks from the last menstrual period
- Clinically defined as the onset of painful, regular uterine contractions associated with cervical effacement and dilation
Prerequisites / Prodromal Events (2-4 weeks before)
| Event | Description |
|---|---|
| Lightening | Fetal presenting part settles into the pelvis; fundal height drops; patient feels pelvic pressure |
| Braxton Hicks contractions | Irregular, painless "practice" contractions increase in frequency |
| Cervical effacement | Cervix softens, shortens, and thins ("ripens") |
| Bloody show | Cervical mucous plug dislodges; blood-tinged mucus passed 1 hour to 1 week before labour. Most women go into true labour within 3 days |
Initiation of Labour - Mechanism
Exact mechanism is not fully understood. Contributing factors include:
- Uterine distension - stretch triggers prostaglandin release
- Prostaglandins (PGE2 and PGF2α) - key mediators of cervical ripening and myometrial contractions
- Oxytocin receptors - myometrial oxytocin receptor numbers increase rapidly (circulating oxytocin levels may not rise initially)
- Decline in progesterone effect - late in pregnancy, progesterone's inhibitory effect on the uterus wanes
True Labour vs. False Labour
| Feature | True Labour | False Labour |
|---|---|---|
| Contractions | Regular, increasing in frequency/intensity | Irregular, no progression |
| Cervical change | Effacement and dilation occur | No cervical change |
| Pain location | Starts in back, radiates to front | Usually only in front |
| Effect of sedation | Not relieved | Often relieved |
| Contractions | Every 2-3 min, ~1 min duration, ~40 mmHg | Variable |
Stages of Labour
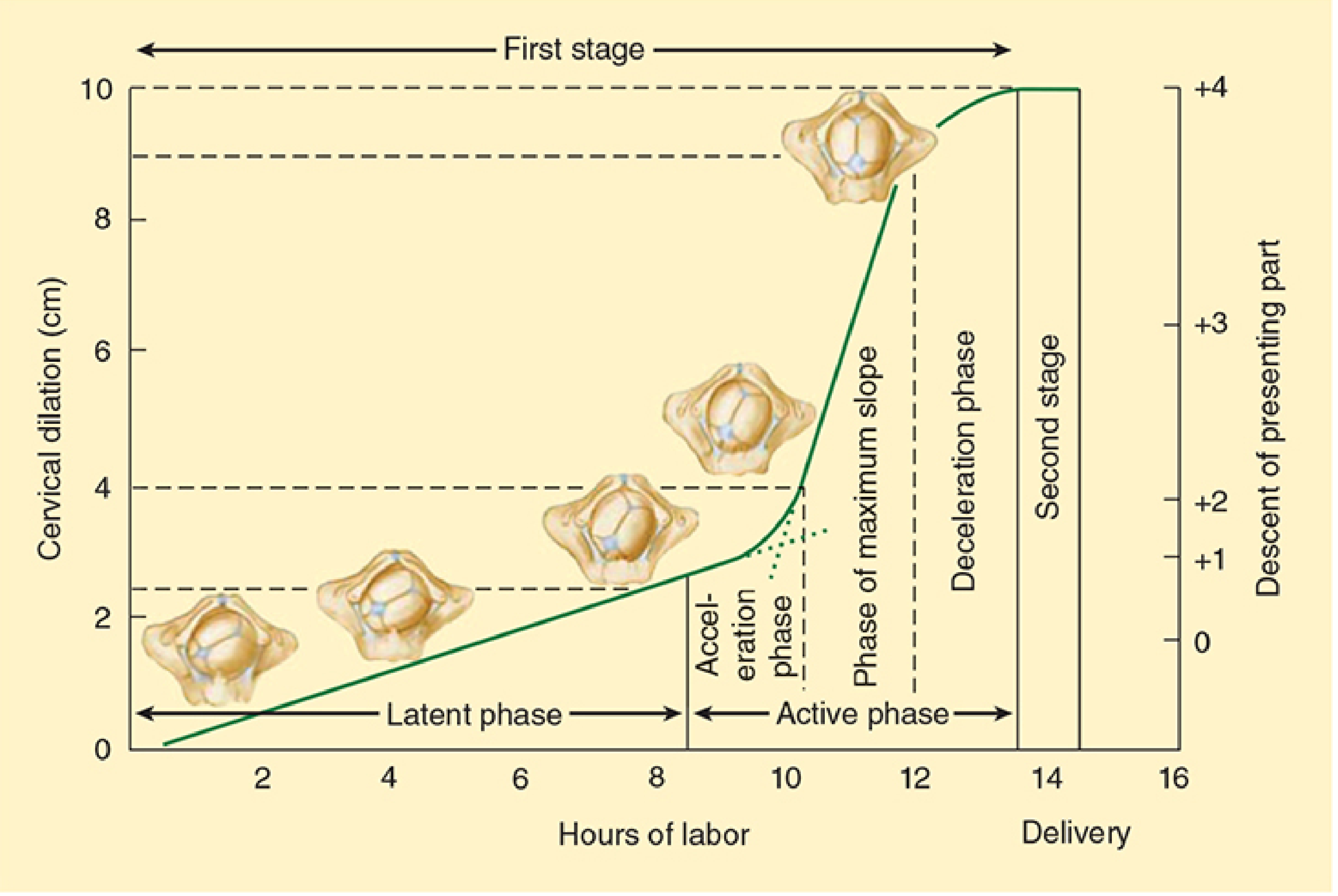
First Stage - Onset of Labour to Full Cervical Dilation (10 cm)
Divided into two phases (Friedman's classification):
a) Latent Phase
- Onset of regular contractions → 3-4 cm dilation
- Progressive cervical effacement + minor dilation (2-4 cm)
- Contractions every 15-20 min
- Duration: up to 20 hours in nulliparas, up to 14 hours in multiparas (upper limits)
- Mean duration: ~6.4 hr (nulliparas), ~4.8 hr (multiparas)
b) Active Phase
- 3-4 cm → 10 cm (full dilation)
- Three sub-phases: Acceleration → Phase of Maximum Slope → Deceleration phase
- Contractions every 3-5 min
- Normal dilation rate: ≥1.2 cm/hr in nulliparas, ≥1.5 cm/hr in multiparas
- Arrest of active phase = no dilation for ≥2 hours
- Duration: ~4.6 hr (nulliparas), ~2.4 hr (multiparas)
Total First Stage: 8-12 hours in nulliparas; 5-8 hours in multiparas
Second Stage - Full Dilation to Delivery of Baby
- Begins at complete cervical dilation (10 cm); ends with delivery of baby
- Fetal descent is the hallmark
- Contractions every 1.5-2 min, lasting 1-1.5 min
- Mother begins bearing down (voluntary expulsive effort)
- Duration: 15-120 min in nulliparas, 15-60 min in multiparas
Third Stage - Delivery of Baby to Delivery of Placenta
- Placental separation and expulsion
- Signs of placental separation:
- Gush of blood
- Lengthening of the umbilical cord
- Uterus rises and becomes globular
- Fundus firms up (Calkin's sign)
- Duration: 15-30 minutes (normal upper limit: 30 min)
Fourth Stage (Pritchard & MacDonald)
- First 1 hour after placental delivery
- Period of uterine contraction, hemostasis, and maternal physiological stabilization
- Vital signs and uterine tone monitored closely
Cardinal Movements of Labour (Mechanism of Normal Vaginal Delivery - Vertex Presentation)
There are 7 cardinal movements in a vertex (occiput anterior) presentation:
| # | Movement | Description |
|---|---|---|
| 1 | Engagement | Biparietal diameter passes through the pelvic inlet |
| 2 | Descent | Continuous process throughout labour |
| 3 | Flexion | Chin-to-chest; presents smallest diameter (suboccipitobregmatic ~9.5 cm) |
| 4 | Internal rotation | Occiput rotates to face the pubic symphysis (OA position) |
| 5 | Extension | Head extends under the pubic symphysis; delivery of the head |
| 6 | Restitution / External rotation | Head rotates back to align with fetal shoulders |
| 7 | Expulsion | Delivery of anterior then posterior shoulder, then body |
Monitoring During Labour
| Parameter | Method |
|---|---|
| Uterine activity | CTG (cardiotocography) or tocodynamometer externally; or intrauterine pressure catheter directly |
| Cervical dilation & effacement | Vaginal examination |
| Fetal descent | Vaginal examination - fetal station (cm above/below ischial spines, -5 to +5) |
| Fetal heart rate | CTG or intermittent auscultation |
Partogram
- Graphical plot of cervical dilation vs. time (WHO recommended tool)
- Helps identify abnormal labour early
- WHO trial showed partogram use reduced: prolonged labours, emergency caesareans, and oxytocin use
Duration of Labour Summary Table
| Stage | Nulliparas | Multiparas |
|---|---|---|
| Latent phase (1st stage) | ~6.4 hr (max 20 hr) | ~4.8 hr (max 14 hr) |
| Active phase (1st stage) | ~4.6 hr | ~2.4 hr |
| Total 1st stage | 8-12 hr | 5-8 hr |
| 2nd stage | 15-120 min | 15-60 min |
| 3rd stage | 15-30 min | 15-30 min |
Abnormal Labour - Quick Reference (Friedman's Criteria)
| Abnormality | Definition |
|---|---|
| Prolonged latent phase | >20 hr nulliparas; >14 hr multiparas |
| Protracted active phase | <1.2 cm/hr dilation in nulliparas; <1.5 cm/hr in multiparas |
| Arrest of active phase | No dilation for ≥2 hours in active phase |
| Protracted descent | <1 cm/hr descent in nulliparas; <2 cm/hr in multiparas |
| Arrest of descent | No descent for ≥1 hour in second stage |
Key Exam Points to Remember
- Labour is defined by cervical change (effacement + dilation), not just contractions
- Friedman's sigmoid curve - latent phase is slow; active phase is fast
- Minimum rate of active phase dilation: 1.2 cm/hr (nullip) vs 1.5 cm/hr (multip)
- Arrest = no change for 2 hours in active phase
- Third stage upper limit = 30 minutes; after this, manual removal of placenta is considered
- The partogram is the WHO-recommended tool for monitoring labour progress
- Cardinal movements = 7 steps for vertex presentation: E-D-F-IR-E-R-E (Engage, Descend, Flex, Internal rotate, Extend, Restitute/External rotate, Expel)
- "Bloody show" = passage of cervical mucous plug; labour within 3 days in most women
- PGE2 and PGF2α are key prostaglandins in labour initiation and cervical ripening
- Fourth stage (first 1 hr post-delivery) = most critical for PPH monitoring
Sources: Creasy & Resnik's Maternal-Fetal Medicine, Principles and Practice | Morgan & Mikhail's Clinical Anesthesiology, 7e | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.