A patient came with epigastric pain for 3 hours. ECG shows normal pattern, troponin I sent ... Inj esomeprazole 40 mg and emistat 8 mg given stat ... What should I do now ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Based on the clinical picture and textbook guidance, here is a structured approach for this patient:
Clinical Assessment: Epigastric Pain — Rule Out ACS First
This presentation is a cardiac emergency until proven otherwise. Epigastric pain lasting 3 hours can be the presenting complaint of inferior/posterior STEMI or NSTEMI, especially in diabetics, elderly, and women. The normal ECG does not exclude ACS — up to 50% of NSTEMIs can have a normal or non-diagnostic initial ECG.
Immediate Next Steps
1. Repeat & Extend the ECG
- Look carefully at leads II, III, aVF (inferior MI) and V1–V4 (anterior/posterior)
- Do posterior leads (V7–V9) — posterior STEMI is frequently missed on standard 12-lead
- Do right-sided leads (V3R, V4R) to rule out right ventricular MI
- Repeat ECG at 15–30 minutes if the first was normal — dynamic changes are diagnostic
2. Await Troponin I Result + Plan Serial Troponins
- A single negative troponin does not rule out NSTEMI — it takes 3–6 hours from symptom onset to rise
- Since pain started 3 hours ago, the first troponin may still be in the early window
- Plan serial troponin at 3 hours (or at 6 hours from symptom onset) — two negatives with a non-diagnostic ECG are needed before ACS can be reasonably excluded
- Use high-sensitivity troponin (hs-TnI) 0/1h or 0/2h protocol if available
3. Full Vitals + Monitoring
- Continuous cardiac monitoring (SpO₂, BP, HR, rhythm)
- IV access (already presumably done for injection)
- Pulse oximetry + supplemental O₂ only if SpO₂ < 94%
4. Bedside Assessment
- Pain character: radiation to jaw/left arm/back? Diaphoresis? Nausea?
- Risk factors: DM, HTN, dyslipidemia, smoking, prior CAD?
- Associated symptoms: vomiting, belching (can suggest GI cause but also inferior MI)
- Examine for epigastric tenderness (deep guarding → GI), pallor, diaphoresis (→ ACS)
5. Urgent Bloods (if not already done)
| Test | Reason |
|---|---|
| Serial Troponin I (at 3h) | Rule out NSTEMI |
| CBC | Anaemia, infection |
| RFT / electrolytes | Baseline before medications |
| Blood glucose / HbA1c | DM workup |
| LFT, lipase/amylase | Pancreatitis, hepatobiliary cause |
| Coagulation | If intervention anticipated |
6. Bedside Ultrasound (POCUS) — if available
- Assess for wall motion abnormalities (LV regional dysfunction = strongly suggests ischaemia)
- Assess for pericardial effusion, gallstones, free fluid
- IVC collapsibility for fluid status
7. Antiplatelet Therapy — Hold Until ACS Confirmed/Excluded
- Do not give aspirin/clopidogrel empirically before ACS is confirmed — if the cause is peptic ulcer disease or GI bleed, this causes harm
- Once troponin returns positive OR ECG changes appear → activate your ACS protocol immediately (aspirin 325 mg loading + clopidogrel/ticagrelor, anticoagulation, cardiology referral/PCI pathway)
8. Current Medications Given
- Esomeprazole 40 mg IV — appropriate empiric gastroprotection; also recommended pre-emptively if ACS is confirmed and dual antiplatelet therapy will be started
- Ondansetron (Emistat) 8 mg — appropriate for nausea/vomiting
Red Flag: When to Activate Cardiac Catheterization Lab NOW
Even before troponin returns, escalate immediately if:
- ECG shows new ST changes, new LBBB, or deep T-wave inversions
- Patient develops haemodynamic instability (hypotension, shock)
- Persistent or worsening pain despite initial management
- Diaphoresis, pallor, new arrhythmia
Summary Algorithm
Epigastric pain 3h + Normal ECG + Troponin pending
↓
Repeat ECG (posterior + RV leads) + Vitals + Monitor
↓
Serial Troponin at 3h from symptom onset
↓
Troponin POSITIVE or ECG changes → ACS protocol (antiplatelet, anticoagulation, cardiology)
Troponin NEGATIVE at 6h + 2 normal ECGs → Consider GI workup (PUD, GERD, pancreatitis)
The key principle here: esomeprazole and ondansetron treat the GI symptoms, but you cannot safely assume a GI cause until ACS is serially excluded. Treat as ACS until proven otherwise. — Goldman-Cecil Medicine; Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22E.
Sudden chest pain for 3 hours , ECG Normal , trop I sent ... What should I do now ?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Here is the full structured approach, backed by Rosen's Emergency Medicine and Harrison's Principles of Internal Medicine:
Sudden Chest Pain × 3h | Normal ECG | Troponin I Pending
The ED evaluation follows three sequential phases:
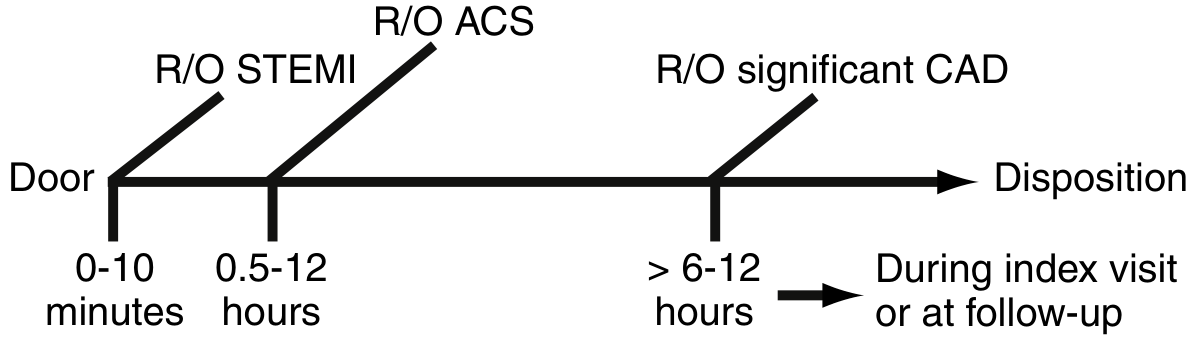
Phase 1 — Do RIGHT NOW (0–10 min)
✅ Already Done
- ECG obtained → No STEMI. Good.
- Troponin I sent. Good.
❗ Still Must Do Immediately
1. Repeat & Extend the ECG
- Standard 12-lead alone is insufficient — add:
- Right-sided leads (V3R, V4R) → Right ventricular infarct
- Posterior leads (V7, V8, V9) → Posterior STEMI (tall R in V1/V2, ST depression V1–V3 is the only clue)
- Repeat ECG every 15–30 min while symptomatic — dynamic changes are diagnostic
2. Continuous Monitoring
- Cardiac monitor + pulse oximetry on immediately
- IV access (large bore)
- Supplemental O₂ only if SpO₂ < 94%
3. Targeted History — The Three Killers You Cannot Miss
| Condition | Red Flag Clue |
|---|---|
| NSTEMI/UA | Crushing, pressure, radiation to arm/jaw, diaphoresis, prior CAD |
| Aortic Dissection | Tearing/ripping pain, maximal at onset, radiates to back, BP difference between arms |
| Pulmonary Embolism | Pleuritic, sudden onset, recent travel/surgery/immobility, leg swelling, tachycardia |
4. Vitals — Both Arms
Unequal BP (>20 mmHg difference) → aortic dissection until proven otherwise
5. Chest X-Ray (stat)
- Widened mediastinum → aortic dissection
- Hampton's hump / Westermark sign → PE
- Pneumothorax line
- Pulmonary oedema → LVF/ACS
Phase 2 — ACS Rule-Out (0.5–12 hours)
Calculate the HEART Score (do this now)
| Variable | 0 | 1 | 2 |
|---|---|---|---|
| History | Slightly suspicious | Moderately suspicious | Highly suspicious |
| ECG | Normal | Non-specific repolarisation | Significant ST deviation |
| Age | < 45 | 45–64 | ≥ 65 |
| Risk factors | No known risk factors | 1–2 risk factors | Known CAD / ≥3 risk factors |
| Troponin | ≤ normal limit | 1–3× normal | > 3× normal |
Use the HEART Pathway with serial troponin at 3 hours:
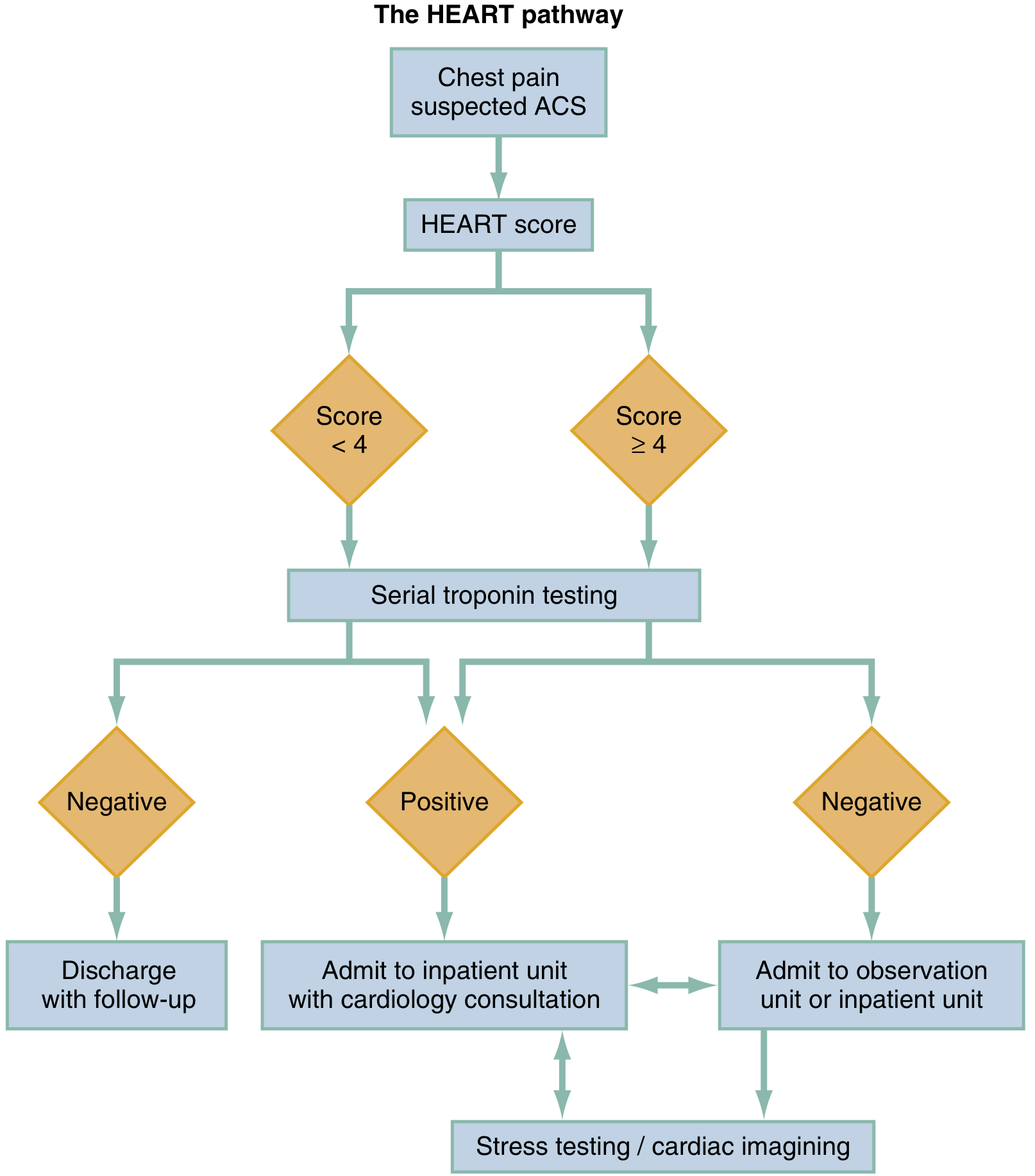
| HEART Score | Serial Troponin | Action |
|---|---|---|
| 0–3 | Both negative | Safe for discharge with short-term outpatient follow-up |
| 0–3 | Any positive | Observation unit or admission |
| 4–6 | Negative | Observation + stress testing / cardiac imaging |
| 4–6 | Positive | Admit + cardiology consult |
| 7–10 | Any | Admit + immediate cardiology (50–65% MACE rate) |
Serial Troponin Timing
- Conventional TnI: measure at presentation → repeat at 3–6 hours from symptom onset
- High-sensitivity TnI (hs-TnI): 0h/1h or 0h/2h protocol
- Since pain started 3h ago, your first troponin may still be within the early window — a single negative does not rule out NSTEMI
- Two negative troponins with a non-diagnostic ECG are needed
Additional Bloods (order now)
- CBC, BMP/electrolytes, creatinine
- D-dimer — if PE probability is intermediate/high (Wells score)
- BNP — if dyspnoea/heart failure features
- Lipase/amylase — if epigastric component
- Coagulation — if intervention anticipated
Phase 3 — Rule-Out Significant CAD (>6–12h)
If serial troponins negative + HEART 4–6 → stress testing or CT coronary angiography during this visit or close follow-up
When to Escalate Before Troponin Returns
Activate the ACS/cath lab team immediately if:
- New ST changes or LBBB on repeat ECG
- Haemodynamic instability (hypotension, shock, new arrhythmia)
- Persistent severe pain despite analgesia
- Clinical picture is highly suspicious (diaphoresis, known CAD, multiple risk factors)
Bottom line: A normal ECG and a single negative troponin do NOT exclude ACS. The patient is in the ACS rule-out window. Calculate the HEART score, monitor continuously, repeat ECG with posterior/right leads, and send a serial troponin at 3 hours. Simultaneously screen for aortic dissection and PE based on the history and vitals. — Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22E
Can we give this patient inj. ALGIN 5 mg
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Inj. Algin (Morphine) 5 mg — In This Patient?
ALGIN is a brand name for Morphine Sulphate. The answer is: use with caution and only if truly necessary, with important caveats.
The Core Problem: ACS Not Yet Ruled Out
This patient is still in the ACS rule-out window. Morphine in suspected ACS — particularly NSTEMI/UA — carries a significant concern that has shifted clinical practice:
⚠️ Morphine in ACS — The Evidence
- Morphine is NOT recommended as routine analgesia in NSTEMI/unstable angina
- Multiple studies (including the CRUSADE registry and the CHAMPION trials) have shown that morphine in NSTEMI is associated with worse outcomes — higher mortality, more reinfarction, longer hospital stays
- The mechanism: morphine delays and reduces the absorption/effect of oral antiplatelet agents (aspirin, clopidogrel, ticagrelor) by slowing gastric motility → less platelet inhibition at a critical time
- The ESC 2020 NSTEMI guidelines downgraded morphine: it is acceptable only for refractory pain not controlled by nitrates, with awareness of this interaction
- STEMI guidelines still permit morphine for pain relief, but with the same caution about antiplatelet delay
What Should You Use First for Pain?
The preferred stepwise approach for ischaemic chest pain:
| Step | Drug | Notes |
|---|---|---|
| 1st | Sublingual GTN (nitroglycerin) 0.4 mg SL, repeat every 5 min × 3 | Relieves ischaemic pain, reduces preload; avoid if BP < 90 mmHg or suspected RV infarct |
| 2nd | IV GTN infusion | If pain persists after 3 SL doses |
| 3rd | Morphine IV (2–4 mg, titrated) | Only if pain refractory to nitrates; use the lowest effective dose |
Additional Considerations Before Giving Morphine
| Concern | Why It Matters |
|---|---|
| BP | Morphine causes vasodilation + hypotension — check BP first; avoid if systolic < 90 mmHg |
| Aortic dissection not excluded | If dissection is possible, morphine may be acceptable for pain, but do NOT give nitrates until BP control is established |
| Pulmonary embolism not excluded | Morphine can depress respiration; use with caution if SpO₂ is borderline |
| Respiratory depression | Have naloxone ready; monitor SpO₂ |
| Nausea/vomiting | Common side effect — you've already given ondansetron (emistat), which provides some cover |
| Antiplatelet timing | If you do give morphine and ACS is confirmed, consider IV antiplatelet loading (cangrelor) or crushed/chewed P2Y12 agents to overcome the delayed absorption effect |
Bottom Line
Do not give morphine as the first analgesic for chest pain in this patient.Try sublingual/IV GTN first. If pain is refractory after adequate nitrate therapy, then morphine 2–4 mg IV (titrated slowly) is acceptable — but keep the dose minimal and monitor closely.If ACS is later confirmed and dual antiplatelet therapy is started, be aware that morphine will blunt ticagrelor/clopidogrel absorption — consider crushed oral agents or IV options.
— Swanson's Family Medicine Review; Goodman & Gilman's Pharmacological Basis of Therapeutics; ESC NSTEMI Guidelines 2020
Can we give inj Visceralgin 5 mg now ?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Inj. Visceralgin (Hyoscine Butylbromide / Buscopan) 5 mg — In This Patient?
Short answer: NO — Do not give it while ACS has not been ruled out.
What Is Visceralgin?
Visceralgin = Hyoscine-N-Butylbromide (Buscopan) — a quaternary anticholinergic antispasmodic that relaxes smooth muscle of the GI tract (and urinary/biliary tract).
It is used for abdominal colic, ureteric colic, biliary colic, IBS spasm.
Why It Is Dangerous in This Patient
1. ⚠️ Anticholinergic → Tachycardia
Hyoscine butylbromide blocks muscarinic receptors, including cardiac M2 receptors, causing reflex or direct tachycardia. In a patient with suspected ACS:
- Tachycardia increases myocardial oxygen demand
- Tachycardia reduces diastolic filling time → less coronary perfusion
- This can worsen ischaemia and precipitate infarct extension
2. ⚠️ Masks the Clinical Picture
The pain of an inferior MI or NSTEMI can perfectly mimic visceral/GI colic. Giving an antispasmodic may:
- Partially relieve the pain (smooth muscle relaxation effect) → false reassurance
- Lead you to label the patient as "GI cause" and delay ACS workup
- This is a known diagnostic pitfall, particularly in inferior MI, diabetics, and women
3. ⚠️ Does Not Treat Ischaemic Pain
Even if the pain does settle, it does not mean the diagnosis was GI. Inferior MI pain frequently has a visceral/epigastric character and can respond non-specifically to various agents.
4. No Benefit if the Cause IS Cardiac
It has zero therapeutic role in ACS and adds only risk.
What Is Safe to Give for Pain Right Now?
| Drug | Appropriate? | Why |
|---|---|---|
| SL/IV Glyceryl Trinitrate (GTN) | ✅ Yes — first choice | Relieves ischaemic pain, vasodilates coronaries; also relaxes oesophageal/biliary smooth muscle |
| Paracetamol IV | ✅ Acceptable | Safe, no cardiac risk |
| Morphine IV (low dose, titrated) | ⚠️ Only if refractory to GTN | As discussed — use sparingly |
| Hyoscine butylbromide (Visceralgin) | ❌ Avoid | Tachycardia risk + diagnostic masking |
| NSAIDs (e.g., ketorolac, diclofenac) | ❌ Avoid | Increase cardiovascular risk, promote platelet aggregation, risk GI bleed if anticoagulation needed |
Once ACS Is Excluded
If serial troponins are negative, ECGs remain normal, and the pain is clearly GI/biliary/ureteric in origin — then Visceralgin (hyoscine butylbromide) 20 mg IV/IM is appropriate and effective. But that decision comes after the cardiac workup is complete.
Bottom line: Visceralgin is contraindicated in this setting — it can cause tachycardia that worsens myocardial ischaemia, and it may falsely reassure you that the pain is non-cardiac. Rule out ACS first. — Maudsley Prescribing Guidelines; pharmacological principles of anticholinergic agents (Goodman & Gilman)
Is inj Tymonium methyl sulphate can be given now ?
Finding Sources
Finding Sources
Tiemonium methylsulphate is not found in the available textbooks. I'll answer from pharmacological principles, clearly flagged.
Inj. Tiemonium Methylsulphate — Can It Be Given Now?
Short answer: Same concern as Visceralgin — avoid until ACS is ruled out.
What Is Tiemonium Methylsulphate?
Tiemonium methylsulphate (brand names: Visceralgine, Tymolin, Spasmotyme) is a quaternary ammonium anticholinergic antispasmodic — pharmacologically in the same class as hyoscine butylbromide (Buscopan/Visceralgin).
It acts by:
- Blocking muscarinic receptors on smooth muscle of the GI, biliary, and urinary tracts
- Reducing visceral spasm and pain
- As a quaternary compound, it has poor CNS penetration (so less sedation than tertiary anticholinergics like atropine) — but cardiac muscarinic blockade still occurs
The Problem in This Patient
The concerns are identical to hyoscine butylbromide:
| Risk | Mechanism |
|---|---|
| Tachycardia | Blocks cardiac M2 receptors → increased heart rate → ↑ myocardial O₂ demand, ↓ diastolic filling time → worsens ischaemia |
| Diagnostic masking | Inferior/posterior MI pain is visceral in character — antispasmodics may partially relieve it, creating false reassurance of a GI cause |
| No cardiac benefit | Zero therapeutic role in ACS; adds only risk |
While tiemonium is considered to have slightly less tachycardic effect than atropine due to its quaternary nature and preferential peripheral action, it is not cardio-neutral — tachycardia is a recognised side effect in its prescribing information.
The Hierarchy of Concern
| Drug class | ACS risk | Action |
|---|---|---|
| GTN (nitrates) | Beneficial | ✅ Give first |
| Paracetamol | Neutral | ✅ Safe |
| Tiemonium / Hyoscine butylbromide | Tachycardia + masking | ❌ Avoid until ACS excluded |
| Morphine | Antiplatelet interaction | ⚠️ Only if GTN fails |
| NSAIDs / COX-2 inhibitors | Pro-thrombotic, ↑ BP | ❌ Avoid |
When Can You Give It?
Once two serial troponins are negative and ECGs remain normal → ACS is reasonably excluded → if the cause is confirmed biliary colic, ureteric colic, or GI spasm → tiemonium methylsulphate 5 mg IV/IM is then appropriate and effective.
Bottom line: Do not give tiemonium methylsulphate now. It is an anticholinergic antispasmodic — same class as Buscopan — and carries a real risk of tachycardia in a patient where ACS has not yet been excluded. Treat pain with GTN first. Revisit once the cardiac workup is complete.
This is a shared conversation. Sign in to Orris to start your own chat.