how to study a physiology of abdominal organs from a chapter based on digestion
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to write a comprehensive, structured guide. Here it is:
Physiology of Abdominal Organs — Digestion Chapter Study Guide
How to Approach This Chapter
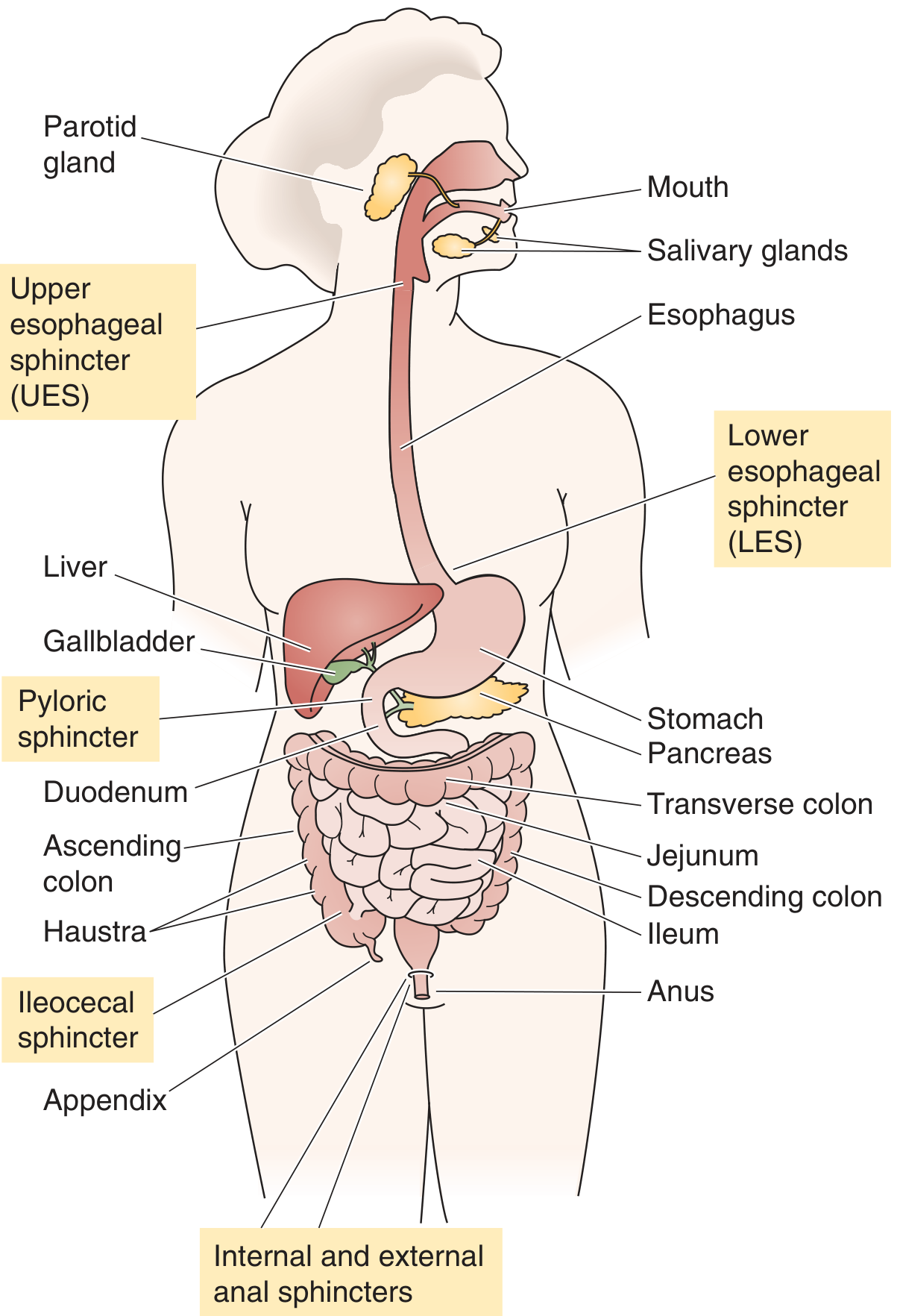
A digestion chapter covers five abdominal organs with distinct but coordinated roles: stomach, small intestine, large intestine, liver/gallbladder, and pancreas. Study them in this logical sequence:
1. Start With the Control Framework (Before Any Organ)
Before diving into individual organs, understand what controls all of them. Three layers govern every GI process:
| Layer | Mechanism | Example |
|---|---|---|
| Neural | Enteric Nervous System (ENS) — myenteric plexus (motility) + submucosal plexus (secretion) | Peristalsis triggered by wall stretch |
| Hormonal | GI hormones released into blood | Gastrin → HCl secretion; CCK → pancreatic enzymes |
| Paracrine | Local cell-to-cell signaling | Histamine → parietal cells |
The ENS acts semi-autonomously. The vagus nerve (parasympathetic) amplifies secretion and motility; sympathetic input inhibits them. Key neurotransmitters: ACh (excitatory motor/secretory), VIP and NO (inhibitory motor). — Medical Physiology, pp. 1278–1279
2. Stomach — The Acid Factory
Two functional roles: mechanical grinding (mixing waves, pyloric pump) and chemical digestion (HCl + pepsin).
Gastric Secretion — learn the cells first:
- Parietal cells → HCl + intrinsic factor
- Chief (peptic) cells → pepsinogen (activated to pepsin by acid)
- G cells (antrum) → gastrin
- D cells → somatostatin (inhibitory)
- Mucous neck cells → mucus + HCO₃⁻ (protective barrier)
Three Phases of Gastric Secretion — a high-yield concept:
- Cephalic phase (~30% of total): smell/taste/thought of food → vagal stimulation via dorsal motor nucleus
- Gastric phase (~60%): food distends stomach → vagovagal reflex + local enteric reflex + gastrin release
- Intestinal phase (~10%): chyme in duodenum releases small amounts of gastrin
— Guyton & Hall, p. 804
Gastric Emptying Control — equally important:
- Stomach wall stretch → accelerates emptying (pyloric pump)
- Duodenal feedback inhibits emptying via enterogastric reflex (triggered by acidity, osmolality, fat/protein breakdown products, distension)
- Hormones: CCK, secretin, GIP slow emptying
- Mnemonic: FADE — Fat, Acid, Distension, Excess osmolality in duodenum → all inhibit gastric emptying
— Guyton & Hall, pp. 11–21
3. Small Intestine — The Absorption Powerhouse
Motor patterns — two types:
- Segmentation (churning): nonpropulsive circular muscle contractions; mixes chyme with enzymes, reduces the unstirred water layer, enhances absorption. Dominant in the fed state.
- Peristalsis (propulsion): progressive wave — upstream circular muscle contracts + longitudinal relaxes; downstream circular relaxes + longitudinal contracts.
- Migrating Motor Complex (MMC): occurs in the fasting state every 90–120 min; sweeps bacteria and debris toward colon. Hormone: motilin. Four phases (quiescence → increasing activity → peak → decline).
— Medical Physiology, pp. 1285–1286
Digestion in the lumen — substrate by substrate:
| Substrate | Where starts | Enzymes | Final products absorbed |
|---|---|---|---|
| Carbohydrates | Mouth (salivary amylase) | Pancreatic amylase → brush-border disaccharidases | Monosaccharides (glucose, fructose, galactose) |
| Proteins | Stomach (pepsin) | Pancreatic: trypsin, chymotrypsin, elastase, carboxypeptidases → brush-border dipeptidases | Amino acids + dipeptides/tripeptides |
| Lipids | Mouth (lingual lipase) | Gastric lipase, pancreatic lipase + colipase, bile salts (emulsification) | Monoglycerides + fatty acids → micelles → absorbed |
Brush-border enzymes complete digestion — this is called membrane digestion. — Medical Physiology, p. 1276
Fluid load perspective: Dietary intake ≈ 1.5–2.5 L/day, but the small intestine receives 8–9 L/day (includes salivary, gastric, biliary, pancreatic, and intestinal secretions). Nearly all is reabsorbed.
Ileocecal valve: prevents backflow; controlled by gastroileal reflex (meal → intensifies ileal peristalsis → opens valve) and cecal distension (reflex closes valve). — Guyton & Hall, pp. 116–119
4. Pancreas — The Enzyme Arsenal
Study pancreatic secretion in two compartments:
- Acinar cells → digestive enzymes (secreted as zymogens — trypsinogen, chymotrypsinogen, proelastase, procarboxypeptidases, pancreatic lipase, amylase)
- Stimulus: CCK (released by fat + protein in duodenum)
- Ductal cells → large volume of HCO₃⁻-rich fluid
- Stimulus: Secretin (released by acid in duodenum)
Key protection mechanism: Enzymes are secreted as inactive zymogens. Enterokinase (brush border) activates trypsinogen → trypsin, which then activates all others. Pancreatic juice HCO₃⁻ neutralizes gastric acid, creating the alkaline pH needed for enzyme function.
5. Liver & Gallbladder — Bile and Metabolism
Bile is the key product for digestion:
- Components: bile salts (conjugated cholesterol), bilirubin, phospholipids, cholesterol, HCO₃⁻
- Function: emulsification of fat → micelle formation → fat absorption
- Enterohepatic circulation: bile salts absorbed in terminal ileum → portal vein → liver → re-secreted into bile (~95% recycled)
Bilirubin metabolism (classic exam topic):
- Heme → bilirubin (unconjugated, lipophilic, albumin-bound) → liver uptake → conjugation with glucuronic acid → secreted in bile → gut bacteria convert to urobilinogen → stercobilin (feces, brown color) or urobilin (urine, yellow color)
— Medical Physiology, pp. 1409–1410
Gallbladder: stores and concentrates bile. CCK (from fat/protein in duodenum) → contracts gallbladder + relaxes sphincter of Oddi → bile enters duodenum.
6. Large Intestine — Absorption and Reservoir
Four functions:
- Absorption of water and electrolytes (converts ~1500 mL liquid chyme → ~100–200 g solid feces)
- Reservoir function (haustra, internal/external anal sphincters)
- Propulsion via haustral shuttling and mass movements (1–3×/day)
- Microbiome activity — fermentation of undigested fiber
Motility pattern: haustrations mix content slowly; mass peristalsis (gastrocolic reflex, triggered by eating) propels content toward rectum.
Study Strategy: Organ-by-Organ Workflow
For each organ, answer these 5 questions:
- What does it receive? (input substrate/fluid)
- What does it secrete? (enzymes, hormones, fluids)
- What controls its secretion? (neural/hormonal stimuli)
- How does it move content? (motor activity)
- What gets absorbed here?
This framework prevents rote memorization and builds mechanistic understanding.
Key Hormones to Master
| Hormone | Source | Stimulus | Main Action |
|---|---|---|---|
| Gastrin | G cells (antrum) | Protein, distension, vagus | ↑ HCl, ↑ pepsinogen |
| Secretin | S cells (duodenum) | Acid in duodenum | ↑ HCO₃⁻ from pancreas/bile ducts; ↓ gastrin |
| CCK | I cells (duodenum/jejunum) | Fat + protein in duodenum | ↑ Pancreatic enzymes, ↑ bile release, ↓ gastric emptying |
| GIP | K cells (duodenum/jejunum) | Fat + glucose | ↓ Gastric secretion; ↑ insulin release |
| Motilin | Mo cells (duodenum) | Fasting | Initiates MMC (phase 3) |
| Somatostatin | D cells (throughout GI) | Acid, fat | Inhibits all GI secretion |
Sources
- Guyton and Hall Textbook of Medical Physiology, pp. 792–895 (Block 8 — GI motility, secretion, digestion)
- Medical Physiology (Boron & Boulpaep), pp. 1275–1543 (Blocks 10–11 — Digestion, absorption, liver)
This is a shared conversation. Sign in to Orris to start your own chat.