I want to prepare for pathology
exam
Asking for Preferences
with flowchart and diagram - containing pathogenesis Risk course morphology
Asking for Preferences
Which topic did you have in mind? Please type it in (e.g. "atherosclerosis", "tuberculosis", "diabetes mellitus", etc.) and I'll build a detailed flowchart + diagram covering pathogenesis, risk factors, course, and morphology for your MBBS exam.
Heart Chapter from Robbins Important Questions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is your complete Heart Chapter exam guide from Robbins, covering all important questions with pathogenesis, risk factors, course, and morphology in flowchart/diagram format.
❤️ HEART - ROBBINS PATHOLOGY
MBBS Exam Prep | Key Topics with Flowcharts
📌 TOPIC 1: HEART FAILURE (Congestive Heart Failure)
Definition
Heart cannot pump blood to meet metabolic demands of peripheral tissues, OR can do so only at elevated filling pressures.
PATHOGENESIS FLOWCHART
PRECIPITATING CAUSE
(IHD / Hypertension / Valvular disease / Cardiomyopathy)
│
▼
↑ Cardiac workload OR ↓ Contractility
│
▼
┌─────────────────────────────────────┐
│ COMPENSATORY MECHANISMS │
│ 1. Frank-Starling mechanism │
│ (↑ filling → ↑ contraction) │
│ 2. Neurohumoral activation │
│ - ↑ Norepinephrine → ↑HR, ↑CO │
│ - ↑ RAAS → Na+/H₂O retention │
│ - ↑ ANP → counterbalances RAAS │
│ 3. Cardiac hypertrophy │
└─────────────────────────────────────┘
│
▼ (mechanisms overwhelmed)
DECOMPENSATION
│
┌──────┴──────┐
▼ ▼
SYSTOLIC DIASTOLIC
DYSFUNCTION DYSFUNCTION
(↓ EF < 40%) (Impaired filling)
HFrEF HFpEF
TYPES & MORPHOLOGY TABLE
| Feature | Left-Sided CHF | Right-Sided CHF |
|---|---|---|
| Causes | IHD, Hypertension, Mitral/Aortic valve disease | Left CHF (most common!), Cor pulmonale, Pulmonary HTN |
| Heart morphology | LV hypertrophy + dilation; LA dilation | RV hypertrophy + dilation |
| Lungs | Heavy wet lungs, pulmonary edema, heart failure cells (hemosiderin-laden macrophages) | Normal lungs |
| Liver | Mild congestion | Nutmeg liver (centrilobular congestion + necrosis) |
| Kidney | Prerenal azotemia | Peripheral edema |
| Other | Orthopnea, PND, basal rales | Ascites, peripheral edema, JVD |
KEY EXAM FACT: Heart failure cells = hemosiderin-laden macrophages in alveoli = sign of previous pulmonary edema (Left CHF)
📌 TOPIC 2: ISCHEMIC HEART DISEASE (IHD)
OVERVIEW FLOWCHART
RISK FACTORS
├── Non-modifiable: Age, Male sex, Family history
└── Modifiable: Hyperlipidemia, Hypertension, Smoking,
Diabetes, Obesity, Sedentary lifestyle
│
▼
CORONARY ATHEROSCLEROSIS (>90% cases)
(Decades of silent plaque buildup)
│
▼
PLAQUE RUPTURE / EROSION
│
▼
THROMBUS FORMATION
│
┌──────┴───────────────────┐
▼ ▼ ▼
STABLE UNSTABLE COMPLETE
ANGINA ANGINA OCCLUSION
(partial, (50% occlusion (STEMI → MI)
stable) + thrombus)
4 CLINICAL PRESENTATIONS OF IHD
| Presentation | Mechanism | Key Feature |
|---|---|---|
| Stable angina | Fixed stenosis >70%, ischemia on exertion | Relieved by rest/nitrates |
| Unstable angina | Plaque rupture + partial thrombus | Rest pain, no necrosis |
| Myocardial Infarction | Complete occlusion → necrosis | Troponin ↑↑ |
| Sudden Cardiac Death | Lethal arrhythmia (VF) | No prior warning |
MYOCARDIAL INFARCTION - DETAILED FLOWCHART
CORONARY ARTERY OCCLUSION
│
▼
ATP depletion (seconds)
│
Loss of contractility (<2 min)
│
ATP 50% of normal (10 min)
│
ATP 10% of normal (40 min)
│
IRREVERSIBLE CELL INJURY (20-40 min)
│
▼
COAGULATIVE NECROSIS
Begins SUBENDOCARDIAL (most vulnerable zone)
│
▼
"Wavefront of necrosis" moves outward
→ TRANSMURAL INFARCT (after ~6-12 hrs without reperfusion)
TIMELINE OF MI MORPHOLOGY (HIGH-YIELD TABLE)
| Time | Gross | Microscopy |
|---|---|---|
| 0-4 hrs | None visible | None (electron microscopy only) |
| 4-12 hrs | Subtle pallor | Early coagulative necrosis; wavy fibers |
| 12-24 hrs | Pallor / mild hyperemia | Coagulative necrosis; PMN infiltration begins |
| 1-3 days | Yellow-tan pallor | PMN infiltration (peak at day 2-3) |
| 3-7 days | Yellow center, hyperemic border | Macrophage infiltration; dead muscle removal |
| 1-2 weeks | Pale, soft, gelatinous | Granulation tissue; fibroblasts + new vessels |
| 2-8 weeks | Gray-white scar | Progressive collagen deposition |
| >2 months | Dense white scar | Dense fibrous scar (complete) |
Mnemonic for PMN peak = Day 1-3; Macrophages = Day 3-7; Granulation tissue = Week 1-2; Scar = >2 months
COMPLICATIONS OF MI (flowchart by timing)
MYOCARDIAL INFARCTION
│
┌──────┴──────────────────────────────────────────┐
▼ EARLY (hours-days) ▼ LATE (weeks-months)
- Arrhythmia (VF) - Dressler syndrome
[most common cause (autoimmune pericarditis,
of death <24 hrs] 2-10 wks post-MI)
- Cardiogenic shock - Ventricular aneurysm
(if >40% LV destroyed) (fibrous wall bulge → thrombus)
- Acute pericarditis - Mural thrombus → embolism
(1-3 days) - Progressive CHF
- Wall rupture (3-7 days) - Papillary muscle fibrosis
→ Cardiac tamponade → chronic MR
- Papillary muscle
rupture → acute MR
📌 TOPIC 3: HYPERTENSIVE HEART DISEASE (HHD)
CHRONIC HYPERTENSION
│
▼
↑ Afterload on LV (Pressure overload)
│
▼
LV CONCENTRIC HYPERTROPHY
(Wall thickness >2cm; Heart weight >500g)
│
▼
DIASTOLIC DYSFUNCTION
(Stiff, non-compliant LV → impaired filling)
│
┌─────┴──────┐
▼ ▼
Compensated Decompensated
(asymptomatic) → LA enlargement → AF
→ IHD (demand ischemia)
→ CHF / SCD
Morphology:
- Gross: Concentric LV hypertrophy, wall >2 cm, heart weight >500 g
- Micro: Enlarged myocyte nuclei ("boxcar nuclei"), interstitial fibrosis
- Right-sided HHD (Cor Pulmonale): Due to pulmonary HTN → RV hypertrophy
📌 TOPIC 4: VALVULAR HEART DISEASE
OVERVIEW
VALVE DISEASE
│
┌──┴──┐
▼ ▼
STENOSIS INSUFFICIENCY (Regurgitation)
(Failure (Failure to close completely
to open) → backflow)
│ │
Pressure Volume overload
overload → dilation
→ hypertrophy
KEY VALVULAR DISEASES TABLE
| Disease | Valve | Cause | Pathogenesis | Morphology | Complication |
|---|---|---|---|---|---|
| Mitral Stenosis | Mitral | Rheumatic heart disease (99%) | Anti-strep antibodies cross-react with cardiac tissue | "Fish mouth" / "Buttonhole" valve; leaflet fusion, calcification | LA dilation → AF → thrombus → embolism; pulmonary HTN |
| Mitral Regurgitation | Mitral | MVP (myxomatous), IHD, RHD | Leaflet prolapse / papillary muscle dysfunction | Floppy, billowing leaflets; LA + LV dilation | Volume overload CHF |
| Aortic Stenosis | Aortic | Calcific degeneration (senile); Bicuspid aortic valve | Calcium deposits on leaflets | "Rock-hard" calcified leaflets | LV pressure overload → syncope, angina, CHF (SAD triad) |
| Aortic Regurgitation | Aortic | Aortic root dilation (HTN, aging, Marfan); RHD | Incomplete leaflet closure | LV dilation (volume overload) | High-output state, wide pulse pressure |
Rheumatic Heart Disease Exam Points:
- Most commonly affects: Mitral > Aortic > Tricuspid > Pulmonary
- Aschoff bodies = pathognomonic granuloma of RHD
- Aschoff cells + Anitschkow cells (caterpillar cells)
- MacCallum plaques = irregular thickening of LA wall (endocardial plaque)
INFECTIVE ENDOCARDITIS COMPARISON
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Organism | S. aureus | S. viridans |
| Valve affected | Normal valves | Previously abnormal valves |
| Vegetation | Large, destructive | Small, less destructive |
| Course | Rapid, fulminant | Indolent |
| Risk | IV drug users | Dental procedures |
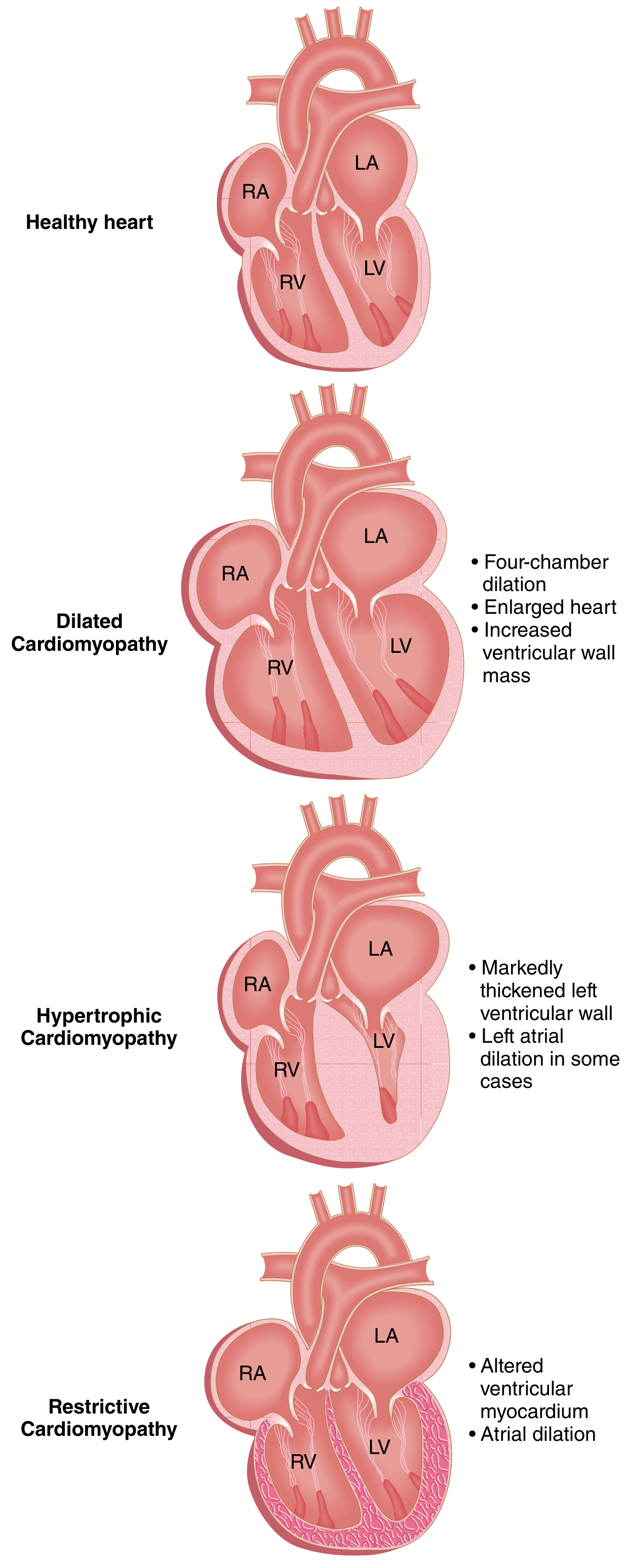
📌 TOPIC 5: CARDIOMYOPATHIES
THREE PATTERNS - COMPARISON DIAGRAM
┌────────────────────────────────────────────────────────────────┐
│ CARDIOMYOPATHY │
├───────────────┬─────────────────┬──────────────────────────────┤
│ DILATED │ HYPERTROPHIC │ RESTRICTIVE │
│ (DCM) │ (HCM) │ (RCM) │
├───────────────┼─────────────────┼──────────────────────────────┤
│ LVEF <40% │ LVEF 50-80% │ LVEF 35-55% │
│ Systolic │ Diastolic │ Diastolic │
│ dysfunction │ dysfunction │ dysfunction │
├───────────────┼─────────────────┼──────────────────────────────┤
│ Causes: │ Causes: │ Causes: │
│ - Genetic │ - Genetic │ - Amyloidosis │
│ - Alcohol │ (sarcomere │ - Radiation fibrosis │
│ - Peripartum │ mutations, │ - Idiopathic │
│ - Myocarditis │ MYH7, MYBPC3)│ │
│ - Hemochromatosis│ - Friedreich │ │
│ - Anthracyclines│ ataxia │ │
├───────────────┼─────────────────┼──────────────────────────────┤
│ MORPHOLOGY: │ MORPHOLOGY: │ MORPHOLOGY: │
│ - Dilated, │ - Asymmetric │ - Normal/slightly │
│ flabby heart│ septal hyper- │ enlarged heart │
│ - All 4 │ trophy (ASH) │ - Stiff, non- │
│ chambers │ - Banana-shaped │ compliant wall │
│ enlarged │ LV cavity │ - Biatrial dilation │
│ - Mural │ - Systolic │ │
│ thrombi │ anterior │ │
│ │ motion (SAM) │ │
│ │ of mitral │ │
│ │ valve │ │
├───────────────┼─────────────────┼──────────────────────────────┤
│ MICROSCOPY: │ MICROSCOPY: │ MICROSCOPY: │
│ - Myocyte │ - Myocyte │ - Amyloid deposits │
│ hypertrophy │ disarray │ (Congo red +) │
│ - Interstitial│ (pathognomonic│ - Diffuse interstitial │
│ fibrosis │ for HCM) │ fibrosis │
└───────────────┴─────────────────┴──────────────────────────────┘
HCM High-Yield: Myocyte disarray = pathognomonic; LVOT obstruction; cause of SCD in young athletes; autosomal dominant (MYH7/MYBPC3 mutations)
📌 TOPIC 6: CONGENITAL HEART DISEASE (CHD)
CLASSIFICATION FLOWCHART
CONGENITAL HEART DISEASE
│
┌──────┴──────┐
▼ ▼
LEFT-TO-RIGHT RIGHT-TO-LEFT OBSTRUCTIVE
SHUNTS SHUNTS LESIONS
(Acyanotic) (Cyanotic)
│ │ │
ASD Tetralogy of Aortic coarctation
VSD Fallot (TOF) Pulmonary stenosis
PDA TGA (Transposition) Aortic stenosis
Truncus arteriosus
Tricuspid atresia
LEFT-TO-RIGHT SHUNTS (Acyanotic - "Late cyanosis")
L→R shunt (ASD/VSD/PDA)
│
▼
↑ Pulmonary blood flow
│
▼
Pulmonary vascular remodeling
│
▼
↑ Pulmonary vascular resistance
│
▼
Pulmonary Hypertension
│
▼
RV Pressure > LV Pressure
│
▼
REVERSAL OF SHUNT → R→L shunt
│
▼
EISENMENGER SYNDROME
(Late cyanosis, polycythemia, paradoxical emboli)
TETRALOGY OF FALLOT (TOF) - The Classic "Blue Baby"
4 Components:
1. VSD (large)
2. Overriding Aorta (sits over VSD)
3. Pulmonary stenosis (RVOT obstruction)
4. RV hypertrophy (secondary to PS)
Pathophysiology:
Pulmonary stenosis → ↑RV pressure
│
▼
R→L shunt through VSD
│
▼
Deoxygenated blood → systemic circulation
│
▼
Cyanosis + Clubbing + Polycythemia
"Tet spells" (hypercyanotic episodes) → Squatting relieves symptoms
(↑systemic resistance → ↓R→L shunt)
📌 SUMMARY: HIGH-YIELD EXAM QUICK REFERENCE
| Topic | Most Important Exam Point |
|---|---|
| CHF | Heart failure cells = hemosiderin macrophages in lung |
| MI Timeline | Irreversible injury at 20-40 min; PMN peak day 1-3; Scar >2 months |
| MI Complication | Rupture day 3-7; Dressler syndrome 2-10 wks; VF = most common death |
| HHD | Concentric LV hypertrophy; heart >500g; wall >2cm |
| Mitral Stenosis | Rheumatic (99%); "Fish mouth" valve; AF → thrombus |
| Aortic Stenosis | Calcific / bicuspid; SAD = Syncope, Angina, Dyspnea |
| IE Acute | S. aureus; normal valve; destructive |
| IE Subacute | S. viridans; abnormal valve; indolent |
| RHD | Aschoff bodies; Anitschkow (caterpillar) cells; MacCallum plaques |
| DCM | Dilated flabby heart; systolic failure; alcohol/peripartum |
| HCM | Myocyte disarray; ASH; SCD in young athletes; AD genetic |
| RCM | Amyloidosis #1; diastolic failure; Congo red staining |
| TOF | 4 components; R→L shunt; cyanosis; squatting relief |
| Eisenmenger | Late cyanosis from L→R reversal; polycythemia |
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 12 (Heart)
with morphology changes and diagrams pls
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Here is the complete Heart Chapter morphology guide from Robbins, with all textbook diagrams and detailed gross + microscopic changes.
❤️ HEART PATHOLOGY - ROBBINS
Complete Morphology Guide with Diagrams
1. ISCHEMIC HEART DISEASE (IHD) & MYOCARDIAL INFARCTION
Progression of Necrosis - Textbook Diagram
From coronary occlusion to completed infarct (0 hr → 2 hr → 24 hr):
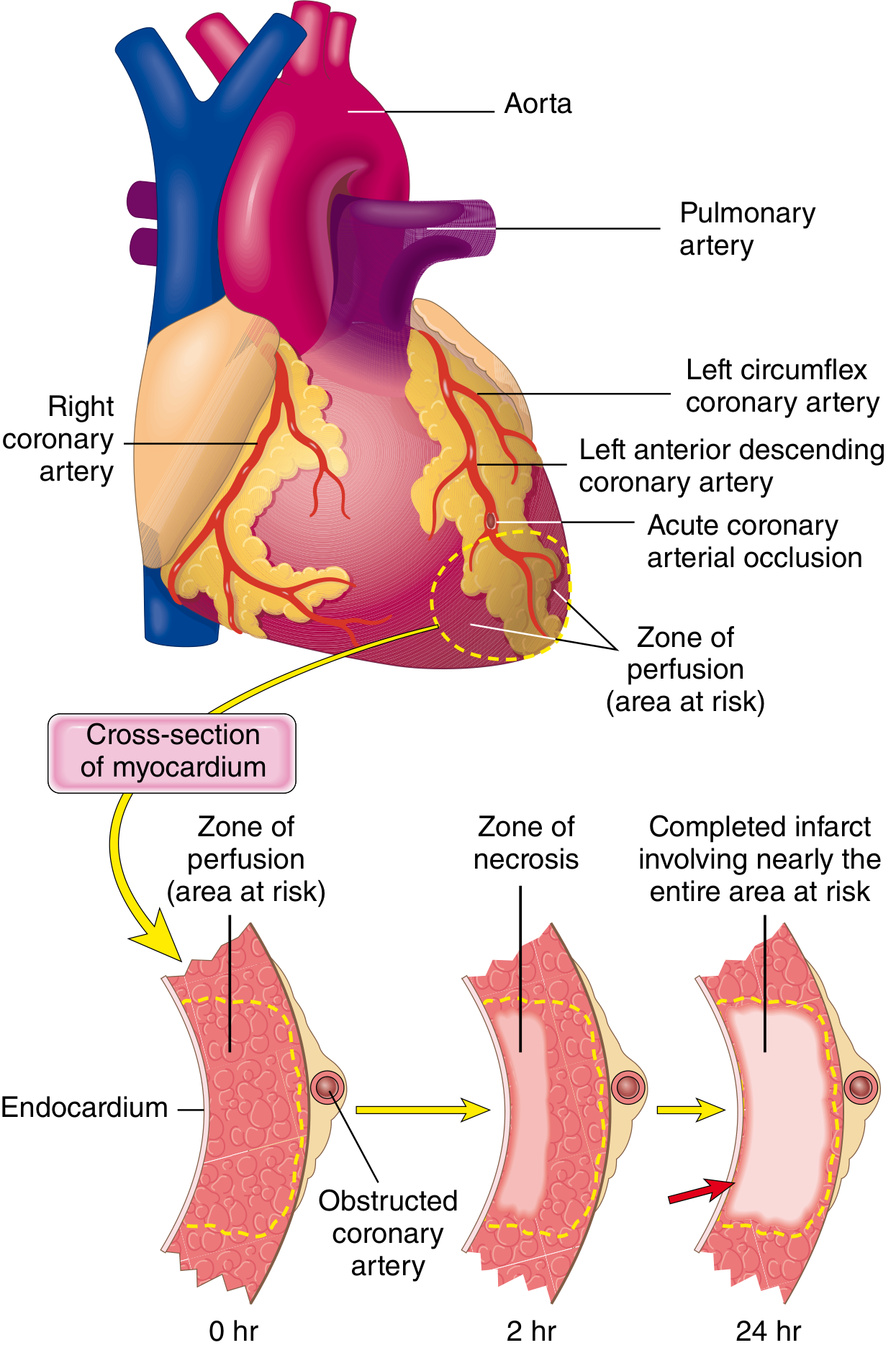
Key point: Necrosis begins SUBENDOCARDIAL (most vulnerable - last to receive blood, highest intramural pressure). With prolonged ischemia the wavefront moves centripetally outward → Transmural infarct by 6-12 hrs.
Infarct Distribution by Artery - Textbook Diagram

| Artery Occluded | Area of Infarct |
|---|---|
| LAD (Left Anterior Descending) | Anterior LV wall + anterior 2/3 of septum + apex |
| LCX (Left Circumflex) | Lateral LV wall |
| RCA (Right Coronary) | Right ventricle + posterior LV + posterior 1/3 septum |
MI Morphology - Sequential Changes
GROSS MORPHOLOGY TIMELINE
TIME GROSS APPEARANCE
─────────────────────────────────────────────────────────
0-4 hrs → Nothing visible (normal gross)
4-12 hrs → Subtle dark mottling / early pallor
12-24 hrs → Pale, tan-yellow infarct center
1-3 days → Yellow-tan pallor (well defined)
3-7 days → Yellow-soft center + HYPEREMIC (red) rim
(most vulnerable to RUPTURE - day 3-7!)
1-2 weeks → Depressed, pale, gelatinous border
2-8 weeks → Gray-white scar forming
>2 months → Dense white-gray SCAR (complete)
MICROSCOPIC TIMELINE - Textbook Photomicrographs
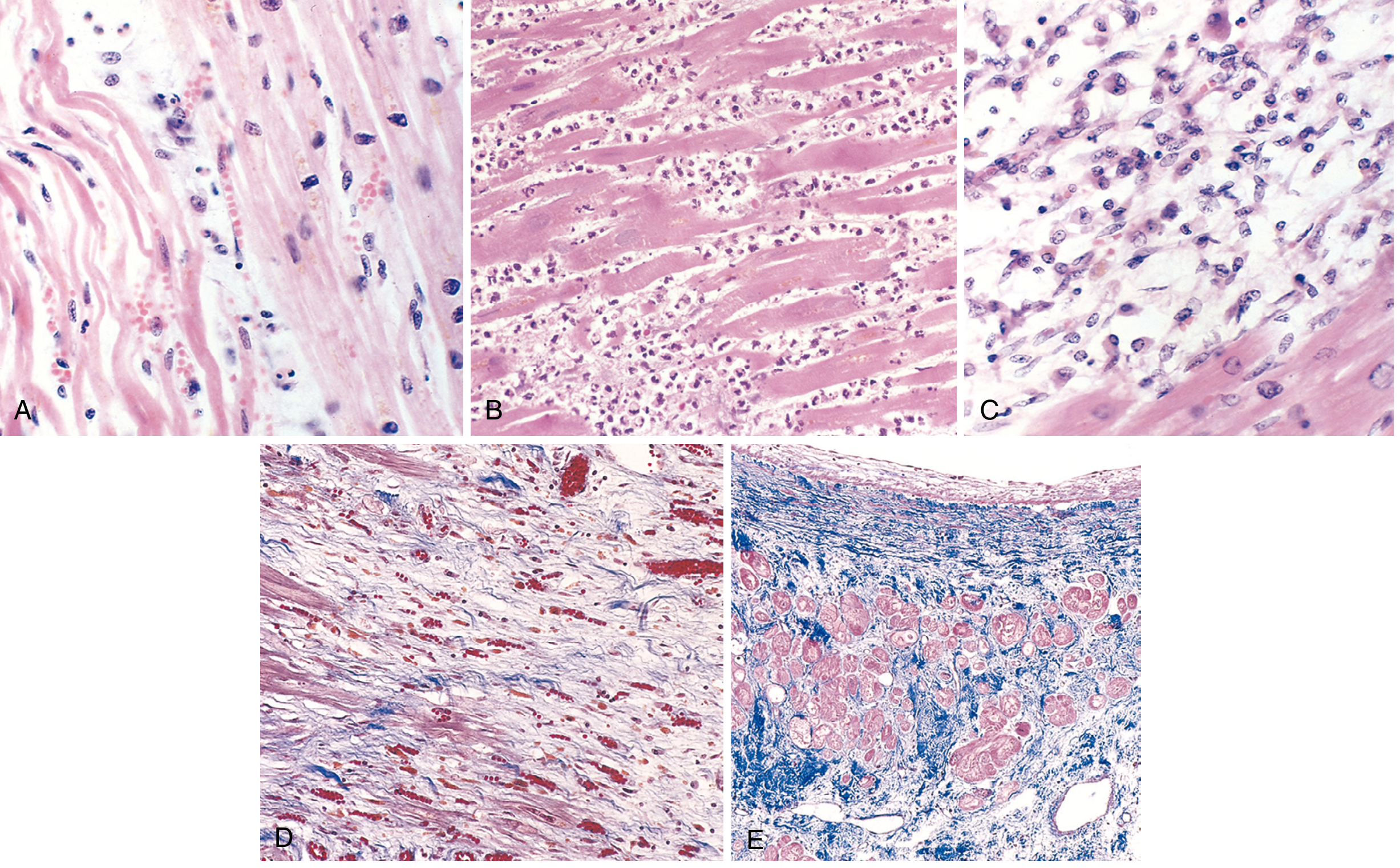
| Stage | Key Microscopic Finding |
|---|---|
| A - Day 1 | Coagulative necrosis + wavy fibers (elongated, narrow) + early PMNs + edema |
| B - Day 3-4 | Dense PMN infiltrate (peak neutrophils) |
| C - Day 7-10 | Macrophage phagocytosis of dead myocytes (removal phase) |
| D - Week 1-2 | Granulation tissue - loose collagen + abundant new capillaries |
| E - Month 2+ | Dense collagenous scar (blue on Masson trichrome), residual myocyte hypertrophy |
Exam tip: Wavy fibers = earliest microscopic sign (day 1). PMNs peak day 2-3. Macrophages day 3-7. Granulation tissue week 1-2. Scar = month 2+.
Morphology Flow: Transmural vs Subendocardial
COMPLETE EPICARDIAL OCCLUSION PARTIAL / TRANSIENT OCCLUSION
(no reperfusion) or GLOBAL HYPOTENSION
│ │
▼ ▼
TRANSMURAL INFARCT SUBENDOCARDIAL INFARCT
- Full-thickness necrosis - Only inner 1/3 of wall
- ST elevation (STEMI) - Circumferential (if shock)
- Single coronary territory - Not limited to one artery
2. HEART FAILURE - MORPHOLOGY
Left-Sided CHF Morphology
LEFT HEART FAILURE
│
┌──────┴────────────────────────┐
▼ HEART ▼ LUNGS
- LV hypertrophy + dilation - Heavy, wet, boggy lungs
- LA dilation (→ AF risk) - Pulmonary edema
- Mural thrombus (in LA) - Hemosiderin-laden macrophages
- Interstitial fibrosis = "HEART FAILURE CELLS"
- Myocyte hypertrophy - Pleural effusion (serous)
- "Brown induration" (chronic)
Heart failure cells = macrophages stuffed with hemosiderin (from phagocytosed RBCs that leaked into alveoli). Pathognomonic of LEFT heart failure.
Right-Sided CHF Morphology
RIGHT HEART FAILURE
│
┌──────┴──────────────────────────────────┐
▼ LIVER ▼ OTHER ORGANS
- "NUTMEG LIVER" - Splenomegaly (congestion)
(centrilobular - Peripheral edema
congestion = dark) - Ascites
(periportal = pale) - Pleural effusion
- Cardiac cirrhosis - Jugular venous distension
(chronic)
Nutmeg liver = alternating dark (congested centrilobular zone) + pale (normal periportal zone) = classic of RIGHT CHF
3. HYPERTENSIVE HEART DISEASE (HHD) - MORPHOLOGY
SYSTEMIC HTN
│
▼
PRESSURE OVERLOAD on LV
│
▼ GROSS:
- LV wall thickness >2 cm (normal ~1 cm)
- Heart weight >500 g (normal ~300-350 g)
- CONCENTRIC hypertrophy (wall thick, cavity small)
- Left atrial enlargement (from diastolic dysfunction)
│
▼ MICROSCOPY:
- ↑ Myocyte transverse diameter
- "BOXCAR NUCLEI" (enlarged, rectangular)
- Perivascular + interstitial fibrosis
Comparison - Concentric vs Eccentric Hypertrophy:
CONCENTRIC (Pressure overload - HTN, AS)
┌─────────────────────┐
│ ████████████████ │ ← Thick wall
│ ██ ██ │ ← Small cavity
│ ████████████████ │
└─────────────────────┘
ECCENTRIC (Volume overload - MR, AR, DCM)
┌─────────────────────┐
│ ██ ██ │ ← Thin wall
│ ██ ██│ ← Large cavity
│ ██ ██ │
└─────────────────────┘
4. VALVULAR HEART DISEASE - MORPHOLOGY
Rheumatic Heart Disease - Textbook Image
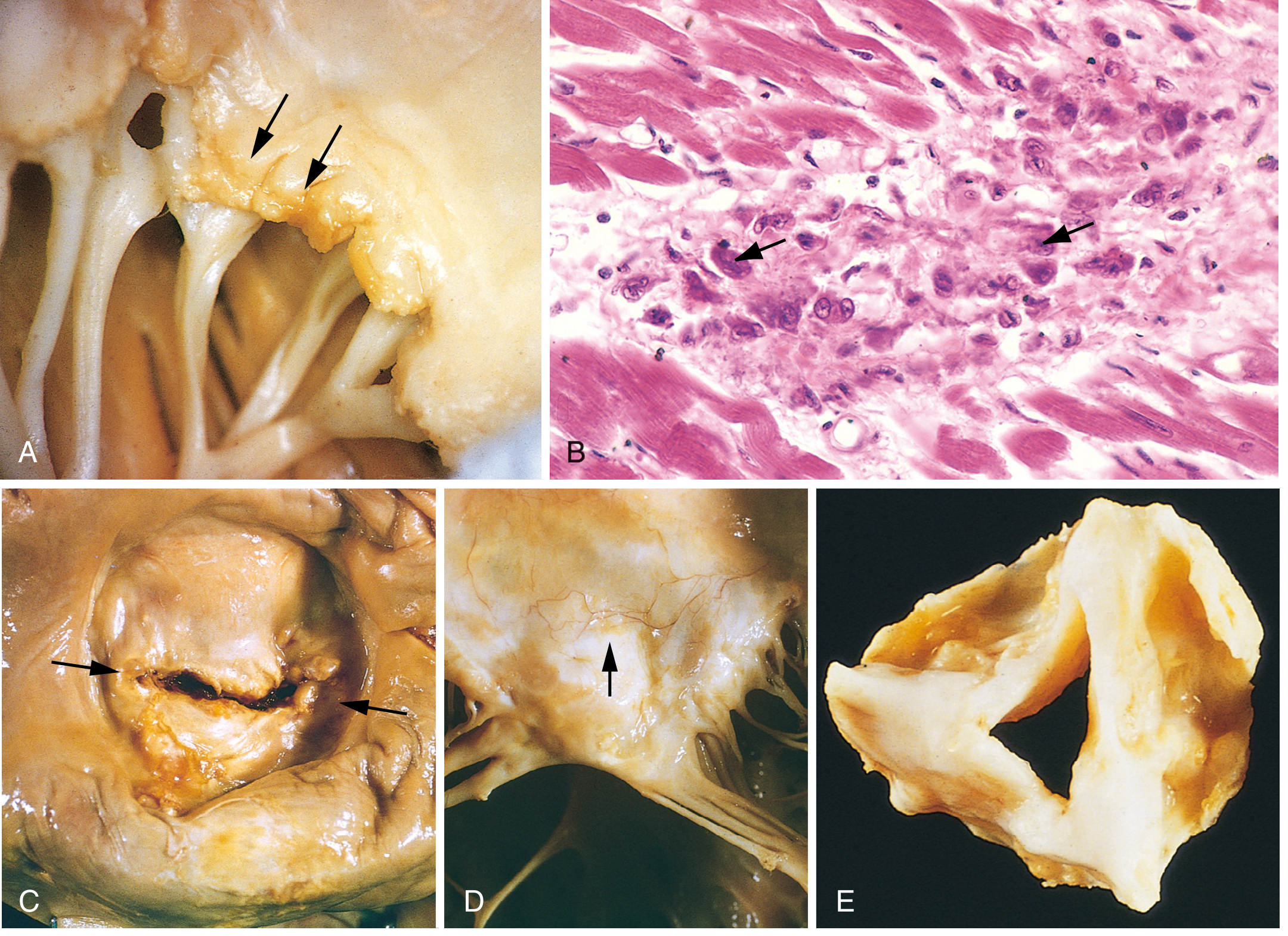
RHD Morphology Flowchart
GROUP A STREP PHARYNGITIS
│
▼ (2-3 week delay)
MOLECULAR MIMICRY
Anti-strep antibodies cross-react with cardiac proteins
│
▼
ACUTE RHEUMATIC FEVER (PANCARDITIS)
│
┌─────┴──────────────────────────────┐
▼ PERICARDITIS ▼ MYOCARDITIS ▼ ENDOCARDITIS
Fibrinous ASCHOFF BODIES Small (1-2mm) verrucae
pericarditis (granulomas with along lines of valve
Anitschkow cells) closure
"Caterpillar cells"
MacCallum plaques
(LA wall)
│
▼ CHRONIC (years of scarring)
MITRAL STENOSIS ("Fish mouth" / "Buttonhole")
- Leaflet thickening + fusion
- Commissural fusion
- Short, thick, fused chordae tendineae
- Calcification
Aschoff body (Pathognomonic of RHD):
Aschoff Body = Granuloma
├── Central fibrinoid necrosis
├── T lymphocytes
├── Plasma cells
└── ANITSCHKOW CELLS (macrophages)
= "Caterpillar cells"
= Elongated wavy chromatin in nuclei
= Pathognomonic of RHD
Mitral Valve Prolapse (MVP) - Myxomatous Degeneration
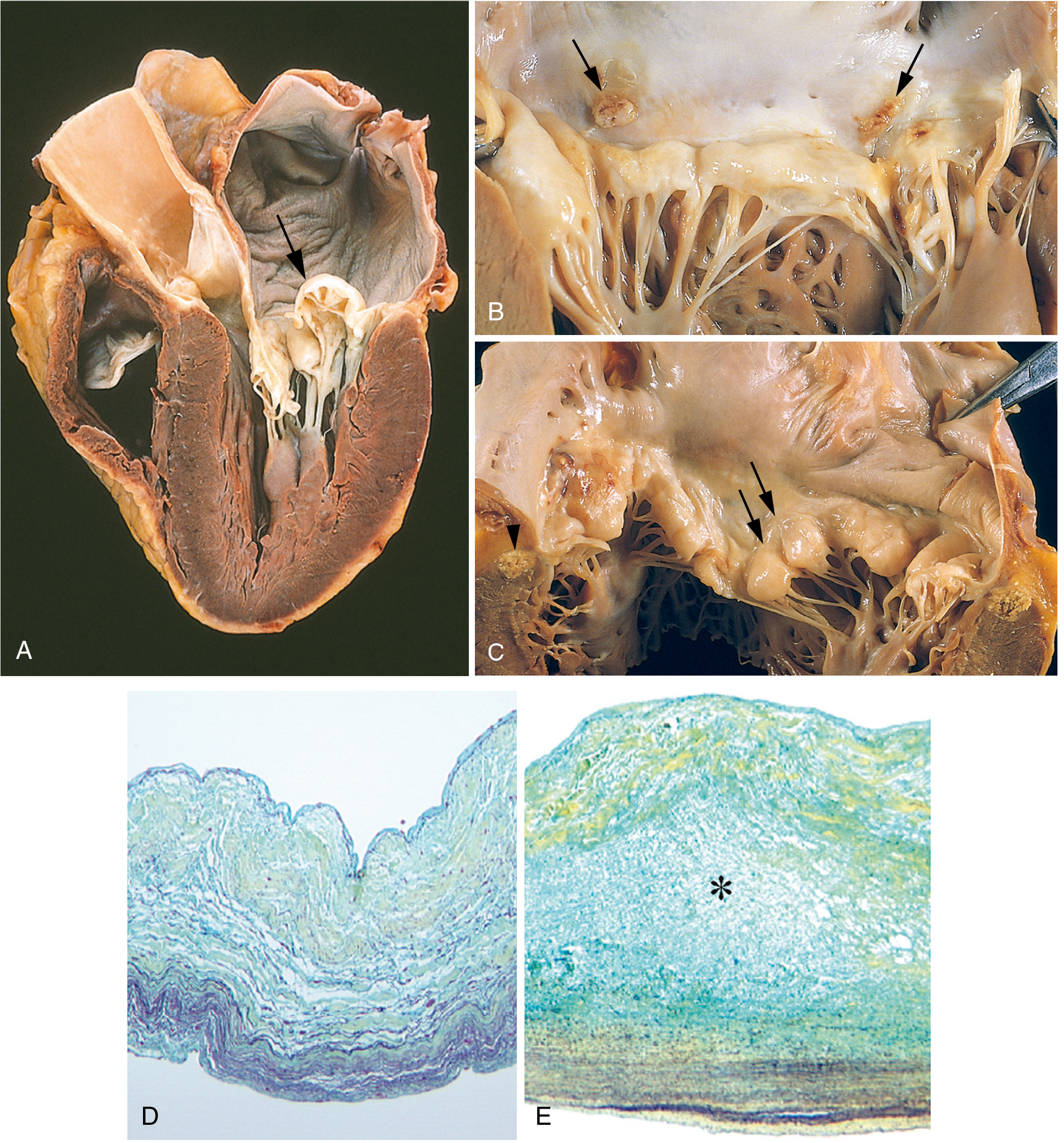
Morphology of MVP:
- Gross: "Hooding/billowing" of posterior (sometimes both) leaflets into LA
- Microscopy: Expansion of spongiosa layer (proteoglycans - blue on Movat stain); disrupted fibrosa (loose, disorganized collagen)
- Sound: Mid-systolic click ± late systolic murmur
Calcific Aortic Stenosis - Morphology
CALCIFIC (DEGENERATIVE) AORTIC STENOSIS
│
GROSS:
- Heaped-up calcified masses on OUTFLOW surface of cusps
- Free edges of cusps NOT involved (unlike RHD)
- "Rock-hard" nodular calcium deposits
- Restricted cusp opening
MICROSCOPY:
- Preserved layered valve architecture
- Calcium deposition in fibrosa layer
- Osteoblast-like cells (bone matrix proteins)
- Does NOT resemble atherosclerosis histologically
Infective Endocarditis - Morphology
INFECTIVE ENDOCARDITIS
│
┌────┴────────┐
ACUTE IE SUBACUTE IE
(S. aureus) (S. viridans)
│ │
LARGE, BULKY, SMALL, FLAT
DESTRUCTIVE VEGETATIONS
VEGETATIONS (less destruction)
- Destroy normal - On damaged valves
valves (bicuspid, MVP, RHD)
- Ring abscesses - Indolent course
- Perforation
│
▼ BOTH TYPES CAUSE:
Emboli (septic infarcts - brain, kidney, spleen)
Osler nodes (painful, fingertips)
Janeway lesions (painless, palms/soles)
Roth spots (retinal hemorrhages)
Splinter hemorrhages (under nails)
5. CARDIOMYOPATHIES - MORPHOLOGY
Visual Comparison - Textbook Diagram
DCM vs HCM - Causes, Pathology, Clinical Features
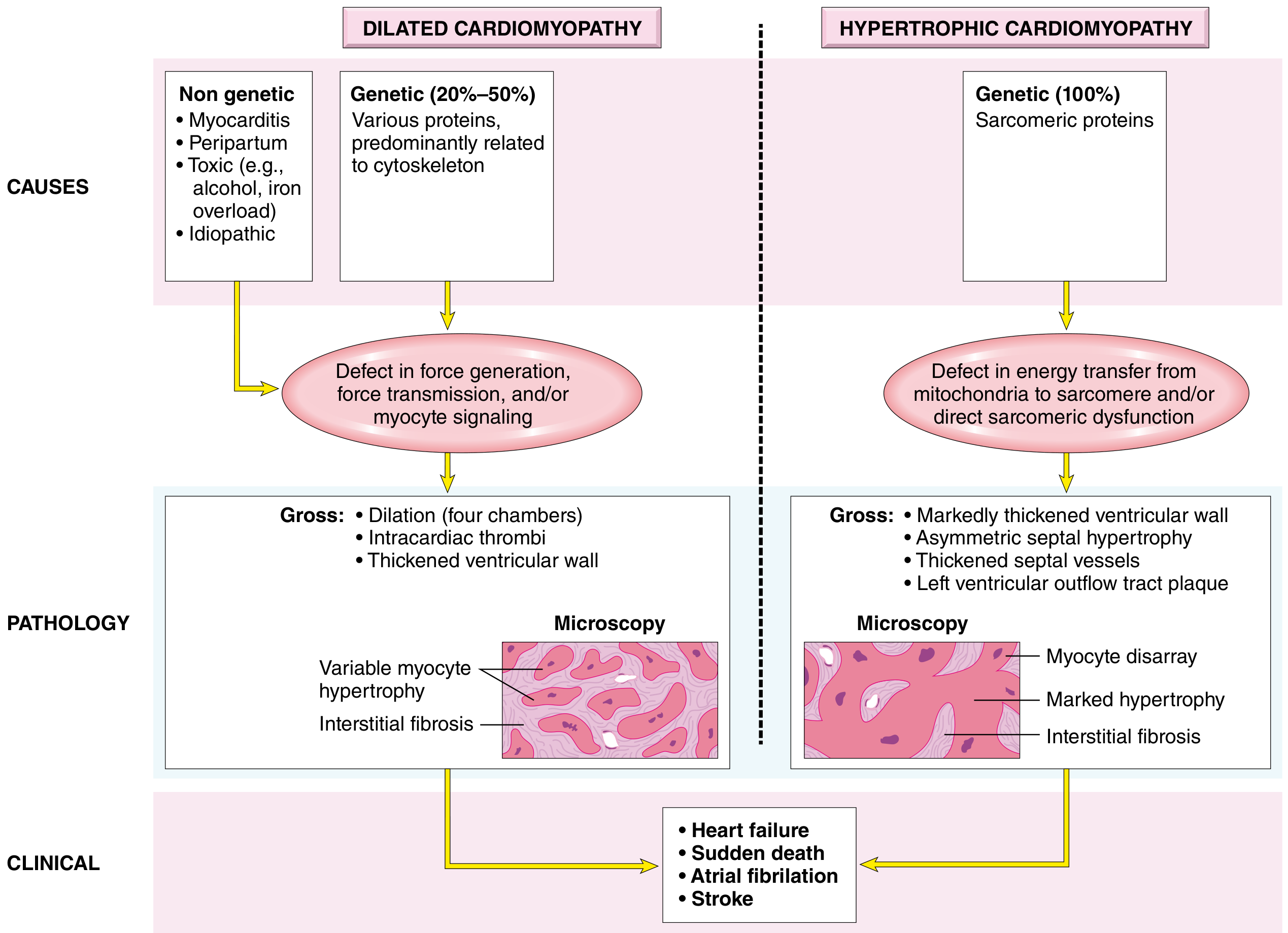
Dilated Cardiomyopathy (DCM) - Detailed Morphology
DILATED CARDIOMYOPATHY
│
GROSS:
- Heart 2-3x normal weight ("flabby, heavy heart")
- ALL FOUR CHAMBERS dilated
- Flabby, hypocontracting walls
- Mural thrombi (common in atrial appendages / apex)
- No primary valve pathology
MICROSCOPY:
- Myocyte hypertrophy (variable)
- Attenuated, stretched myocytes
- Interstitial + endocardial fibrosis
- Small subendocardial scars
- "Ninja star nuclei" in titin mutation DCM
(hyperchromatic, distorted nuclei)
Hypertrophic Cardiomyopathy (HCM) - Detailed Morphology
HYPERTROPHIC CARDIOMYOPATHY
│
GROSS:
- Massive hypertrophy WITHOUT dilation
- ASYMMETRIC SEPTAL HYPERTROPHY (ASH) = classic
(septum:free wall ratio >1.3)
- "Banana-shaped" LV cavity
- LV outflow tract plaque (endocardial thickening
from contact with anterior mitral leaflet)
- Normal or small LV cavity
MICROSCOPY (4 key features):
1. Massive myocyte hypertrophy (diameter >40μm; normal ~15μm)
2. MYOFIBER DISARRAY = pathognomonic!
(haphazard arrangement of bundles + sarcomeres)
3. Fibrotic narrowing of small intramural arteries
4. Interstitial and replacement fibrosis
MYOFIBER DISARRAY = Pathognomonic of HCM - myocytes arranged in chaotic, pinwheel-like patterns instead of parallel rows.
Restrictive Cardiomyopathy (RCM) - Morphology
RESTRICTIVE CARDIOMYOPATHY
│
GROSS:
- Normal or slightly enlarged ventricles
- NO ventricular dilation
- BIATRIAL DILATION (from impaired filling → backup)
- Stiff, non-compliant walls
MICROSCOPY:
- Patchy or diffuse interstitial fibrosis
- Amyloidosis (#1 cause):
- Deposits in myocardial interstitium
- CONGO RED stain → apple-green birefringence
- "Sparkling" appearance on echo
6. CONGENITAL HEART DISEASE - MORPHOLOGY SUMMARY
LEFT-TO-RIGHT SHUNTS RIGHT-TO-LEFT SHUNTS
(Acyanotic early) (Cyanotic from birth)
ASD: TOF (4 components):
- Secundum type most common 1. Large VSD
- LA + RA dilation 2. Overriding aorta
- RV hypertrophy (late) 3. Pulmonary stenosis
4. RV hypertrophy
VSD: Gross finding: "Boot-shaped heart"
- Membranous most common (RV hypertrophy = coeur en sabot)
- RV pressure overload
- Eisenmenger if large TGA:
- Aorta from RV (anterior)
PDA: - PA from LV (posterior)
- Continuous "machinery" - Two parallel circuits
murmur - Not compatible with life
- LA + LV dilation without mixing (VSD/ASD/PDA)
MASTER MORPHOLOGY QUICK-REFERENCE TABLE
| Condition | Gross Finding | Microscopy | Pathognomonic Feature |
|---|---|---|---|
| MI Day 1-3 | Pale, yellow-tan | Coagulative necrosis, wavy fibers, PMNs | Wavy fibers (earliest sign) |
| MI Day 3-7 | Yellow center + red rim | Macrophages, removal of debris | Rupture risk peak |
| MI Healed | White-gray scar | Dense collagen (blue-Masson trichrome) | Dense fibrous scar |
| Left CHF | Dilated LV, wet lungs | Hemosiderin macrophages in alveoli | Heart failure cells |
| Right CHF | RV hypertrophy | Centrilobular congestion | Nutmeg liver |
| HHD | Concentric LV hypertrophy | Boxcar nuclei, perivascular fibrosis | LV wall >2 cm, heart >500g |
| RHD (Acute) | 1-2mm verrucae at line of closure | Aschoff bodies + Anitschkow cells | Aschoff bodies |
| RHD (Chronic) | Fish-mouth mitral valve | Leaflet thickening + fibrosis | Commissural fusion |
| DCM | Flabby, ALL chambers dilated | Variable hypertrophy, interstitial fibrosis | Mural thrombi |
| HCM | Asymmetric septal hypertrophy | Myofiber disarray | Disarray = pathognomonic |
| RCM | Biatrial dilation | Interstitial fibrosis/amyloid | Congo red + (amyloid) |
| MVP | Billowing/hooding leaflets | Expanded spongiosa (proteoglycans) | Mid-systolic click |
All content sourced from: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 12 (Heart)
This is a shared conversation. Sign in to Orris to start your own chat.