Give me an exact sample case outline for pappilary thyroid carcinoma, of course rephrase it using this acute cholecystitis case as an example Part 1 : Model CCP: Acute Cholecystitis Patient Presentation Chief Complaint: A 42-year-old woman presents to the Emergency Department with severe right upper quadrant pain for 18 hours. History of Present Illness: The pain began suddenly after eating fried chicken for dinner. It is constant, severe, and localized to her right upper quadrant, radiating to her right scapula. She has associated nausea and vomiting x3. She reports feeling feverish and has had no appetite since the pain started. The pain is not relieved by position changes or over-the-counter antacids. Similar mild pain 3 months ago treated by GP Past Medical History: Obesity (BMI 34) Diet-controlled hyperlipidaemia Two previous uncomplicated pregnancies Medications: None regularly. Social History: Works as an accountant. Smokes 10 cigarettes/day for 20 years. Drinks 1-2 glasses of wine on weekends. Has been trying to lose weight through a low-carbohydrate diet. Family History: Mother had gallbladder surgery in her 40s. Physical Examination General: Anxious, obese woman lying still on the gurney (movement worsens pain). Vital Signs: Temperature: 38.6°C Heart Rate: 112 bpm Blood Pressure: 145/90 mmHg Respiratory Rate: 22/min SpO₂: 97% on room air Abdomen: Inspection: Obese, non-distended, no scars Palpation: Marked tenderness in the right upper quadrant with voluntary guarding. Positive Murphy's sign (patient arrests inspiration when examiner palpates beneath right costal margin). Percussion: Normal liver span (12 cm), no shifting dullness Auscultation: Hypoactive bowel sounds Other: Sclera is anicteric. No palpable lymphadenopathy. Clinical Summary 42 yr old female patient presented with severe RHC pain for 18hrs.Associated with vomiting and pain radiates to R. shoulder. Milder similar pain 3 months ago Tenderness and guarding RHC Mild fever but no jaundice Diagnoses Acute calculous cholecystitis Cholangitis Acute gastritis PUD Acue pancreatitis Initial Investigations Laboratory Results: WBC: 15.8 × 10⁹/L (85% neutrophils) CRP: 95 mg/L Total Bilirubin: 28 μmol/L (slightly elevated) ALP: 110 U/L (normal) ALT: 65 U/L (slightly elevated) AST: 70 U/L (slightly elevated) Amylase: 60 U/L (normal) Lipase: 45 U/L (normal) Imaging: Abdomen (Right Upper Quadrant) Ultrasound: Multiple gallstones in gallbladder lumen One large stone (15mm) impacted in the gallbladder neck Gallbladder wall thickness: 5mm (>3mm is abnormal) Positive sonographic Murphy's sign (maximal tenderness when transducer presses over gallbladder) Minimal pericholecystic fluid Common bile duct diameter: 4mm (normal <6mm) No intrahepatic biliary dilation Diagnoses/Clinical Course Provisional diagnosis: acute calculous cholecystitis. Differential diagnoses: Acute gastritis PUD Cholangitis Acue pancreatitis Initial Management: Made NPO (Nil Per Os) IV hydration with crystalloids IV analgesia (ketorolac) IV antibiotics (ceftriaxone 1g daily + metronidazole 500mg q8h) Definitive Management: After 12 hours of medical management with improvement in fever and pain, she underwent laparoscopic cholecystectomy. Surgery revealed an inflamed, distended gallbladder with the stone impacted in the neck. The cystic duct and artery were clearly identified and ligated. No bile duct injury occurred. Post-operative Course: She recovered well, was advanced to a clear liquid diet on post-operative day 1, and discharged
Model CCP: Papillary Thyroid Carcinoma
Patient Presentation
- No prior thyroid disease
- Childhood head/neck irradiation (for tinea capitis)
- No other chronic illnesses
Physical Examination
- Temperature: 36.8°C
- Heart Rate: 78 bpm
- Blood Pressure: 118/74 mmHg
- Respiratory Rate: 16/min
- SpO₂: 99% on room air
- BMI: 23
- Inspection: A visible midline/right-sided anterior neck swelling that moves upward with swallowing — consistent with thyroid origin.
- Palpation: A firm, non-tender, 2.5 cm nodule in the right lobe of the thyroid gland. The nodule is not freely mobile; there is subtle fixation to surrounding tissue. No palpable contralateral lobe nodules.
- Cervical lymph nodes: A 1.5 cm firm, non-tender node palpable in the right level III cervical chain.
- No tracheal deviation. No stridor.
Clinical Summary
Differential Diagnoses
- Papillary thyroid carcinoma (primary concern)
- Follicular thyroid carcinoma
- Benign colloid/simple thyroid nodule
- Hashimoto's thyroiditis with nodularity
- Medullary thyroid carcinoma
Initial Investigations
| Test | Result | Reference |
|---|---|---|
| TSH | 1.4 mIU/L | Normal (0.4–4.0) |
| Free T4 | 14.2 pmol/L | Normal |
| Free T3 | 4.8 pmol/L | Normal |
| Serum Calcium | 2.28 mmol/L | Normal |
| Calcitonin | 4 pg/mL | Normal (<10) |
| Anti-TPO antibodies | Negative | — |
| CEA | Mildly elevated | — |
| FBC/CRP | Normal | — |
- Right thyroid lobe: 2.5 cm solid, hypoechoic nodule with irregular/spiculated margins and microcalcifications (psammoma body pattern) — TIRADS 5 (highly suspicious)
- No halo sign
- Increased intranodular vascularity on Doppler
- Right level III: 1.5 cm cervical lymph node with loss of fatty hilum and microcalcifications — suspicious for metastatic involvement
- Left lobe: normal, no nodules
- No retrosternal extension
- Right thyroid nodule with subtle extrathyroidal extension at the posterior capsule
- Right cervical lymphadenopathy (levels III–IV)
- No distant pulmonary metastases
- Bethesda Category VI: Malignant
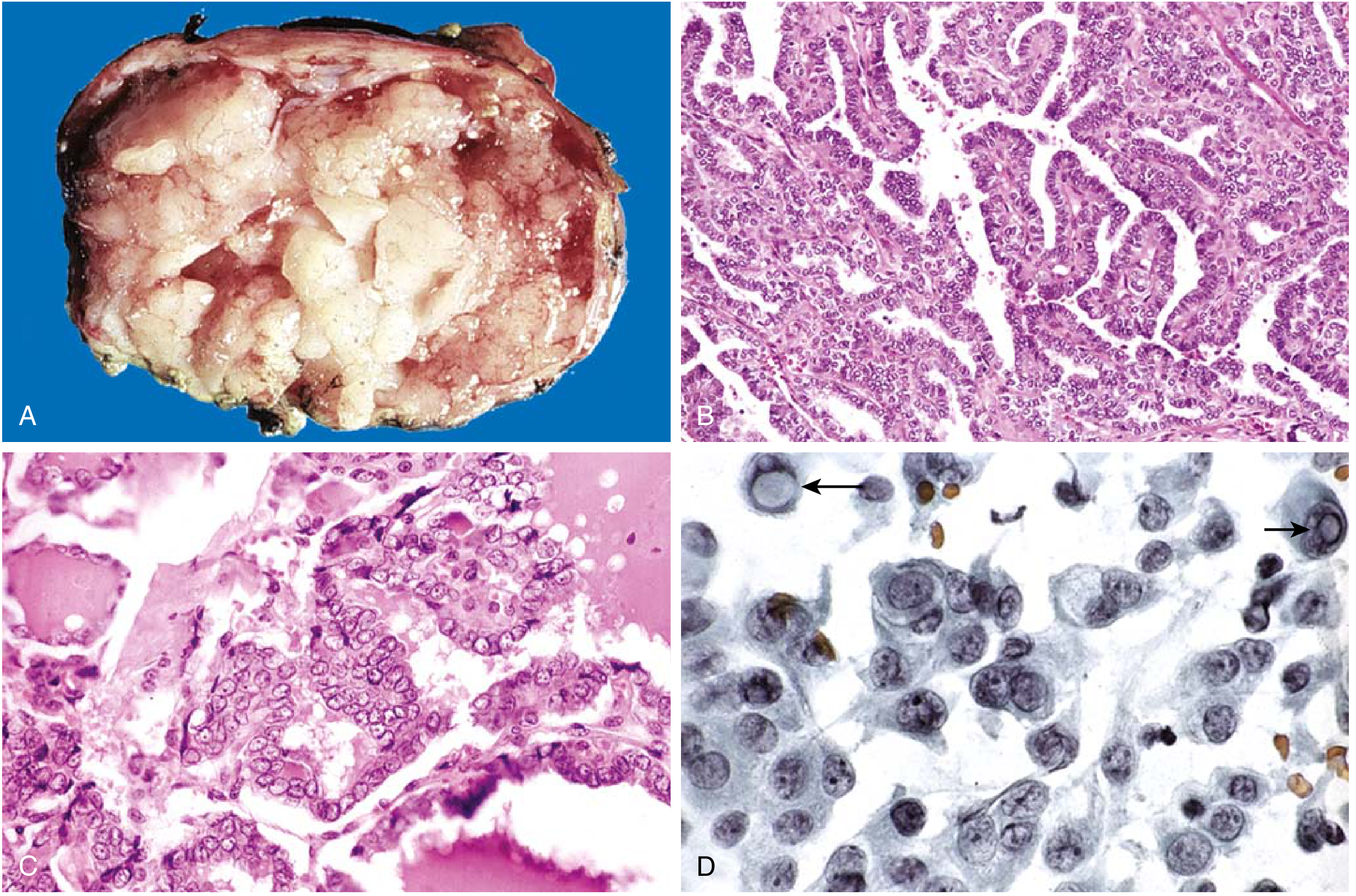
- Cytology: Papillary architecture with cells showing ground-glass "Orphan Annie eye" nuclei, nuclear grooves, intranuclear pseudoinclusions, and psammoma bodies
- Consistent with Papillary Thyroid Carcinoma
- BRAF V600E mutation analysis: Positive (BRAF mutation is the most common genetic event in PTC, accounting for ~50% of cases, and is associated with higher risk of extrathyroidal invasion, lymph node metastasis, and recurrence — K.J. Lee's Essential Otolaryngology)
Diagnosis / Clinical Course
- T2 (2.5 cm, possible extrathyroidal extension → T3a)
- N1a/N1b (ipsilateral cervical nodes)
- M0 (no distant metastases)
- Stage I (all PTC patients < 55 years are Stage I or II regardless of nodal status)
Initial Management
- Referred to Endocrine Surgery
- Reassurance and education regarding excellent prognosis (10-year survival >95%)
- Pre-operative vocal cord assessment (laryngoscopy) to document RLN function
- Pre-operative neck ultrasound mapping of all suspicious lymph nodes
- Routine pre-operative bloods, ECG, and anaesthetic assessment
Definitive Management
- Total thyroidectomy indicated given: tumour >1 cm, BRAF mutation positivity, extrathyroidal extension, and regional lymph node involvement — making post-operative RAI therapy mandatory
- Central neck dissection (Level VI): performed given known lymph node involvement (systematic resection of Delphian, pretracheal, perithyroidal, and paratracheal nodes)
- Intraoperative nerve monitoring of the recurrent laryngeal nerve (RLN)
- Parathyroid glands identified and preserved (or autotransplanted if devascularised)
- 2.5 cm firm, whitish, infiltrative right thyroid nodule with focal capsular breach
- Three matted right level VI lymph nodes
- Both recurrent laryngeal nerves preserved
- All four parathyroids identified and preserved
- Indicated post-total thyroidectomy to ablate residual thyroid tissue, facilitate surveillance with thyroglobulin, and treat potential microscopic metastases
- Low iodine diet for 2 weeks prior to RAI
- TSH stimulation achieved (via levothyroxine withdrawal or recombinant TSH/Thyrogen)
- Initiated post-operatively; target TSH 0.1–0.5 mIU/L (mild suppression, given Stage I, low-risk)
- Prevents TSH-driven tumour recurrence
Post-operative Course
- Post-operative serum calcium monitored (risk of hypoparathyroidism)
- Serum thyroglobulin (Tg) measured as a tumour marker — should be undetectable after total thyroidectomy + RAI if no residual disease
- Anti-thyroglobulin antibodies (anti-Tg Ab) checked (can interfere with Tg assay)
- Voice assessed on post-operative day 1 — normal, no RLN injury
- Discharged on day 2 on levothyroxine with outpatient endocrinology follow-up
- Long-term surveillance: 6–12 monthly neck ultrasound + serum Tg monitoring
Shorten it, not too long
Model CCP: Papillary Thyroid Carcinoma
Patient Presentation
Physical Examination
- Temperature: 36.8°C | HR: 78 bpm | BP: 118/74 mmHg | SpO₂: 99%
- Firm, non-tender 2.5 cm right thyroid nodule, moves on swallowing, mildly fixed to surrounding tissue
- 1.5 cm firm right level III cervical lymph node — non-tender, loss of fatty hilum
- No tracheal deviation, no stridor
Clinical Summary
Differential Diagnoses
- Papillary thyroid carcinoma
- Follicular thyroid carcinoma
- Benign colloid nodule
- Hashimoto's thyroiditis with nodularity
- Medullary thyroid carcinoma
Initial Investigations
| Test | Result |
|---|---|
| TSH | 1.4 mIU/L (normal) |
| Free T4 | 14.2 pmol/L (normal) |
| Calcitonin | 4 pg/mL (normal) |
| Serum Calcium | 2.28 mmol/L (normal) |
| Anti-TPO antibodies | Negative |
- 2.5 cm solid, hypoechoic right nodule with spiculated margins and microcalcifications — TIRADS 5
- Right level III lymph node: loss of hilum, microcalcifications — suspicious for metastasis
- Left lobe: normal
- Papillary architecture, "Orphan Annie eye" nuclei, nuclear grooves, intranuclear pseudoinclusions, psammoma bodies
- Consistent with Papillary Thyroid Carcinoma
Diagnosis & Clinical Course
- Follicular carcinoma
- Medullary carcinoma
- Benign nodule with reactive lymphadenopathy
Management
- Referred to Endocrine Surgery
- Pre-operative laryngoscopy (RLN baseline assessment)
- CT neck/chest to assess extrathyroidal extension and distant metastases
- Total thyroidectomy + right central neck dissection (Level VI)
- Intraoperative RLN monitoring; parathyroids identified and preserved
- Radioactive iodine (RAI ¹³¹I) ablation post-operatively
- Levothyroxine TSH suppression therapy (target TSH 0.1–0.5 mIU/L)
Post-operative Course
- Calcium and PTH monitored (hypoparathyroidism risk)
- Serum thyroglobulin (Tg) as ongoing tumour marker — should be undetectable post-RAI
- Voice normal; no RLN injury
- Discharged day 2; outpatient endocrinology follow-up
- Surveillance: 6–12 monthly neck ultrasound + Tg levels