Testicular torsion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough answer.
Testicular Torsion
Epidemiology & Pathophysiology
Testicular torsion has an incidence of approximately 1 in 4,000 males under age 25. It has a bimodal age distribution: a peak in the first year of life and a second peak at puberty (during rapid testicular growth). — Rosen's Emergency Medicine, p. 1401
The condition occurs when the spermatic cord twists, initially causing venous outflow obstruction, followed by compromised arterial flow and progressive testicular ischemia. Without reversal, irreversible ischemic damage begins as early as 4 hours and is complete by 8–12 hours of ischemia. — Sabiston Textbook of Surgery, p. 2832
Two anatomical types:
| Type | Age Group | Mechanism |
|---|---|---|
| Extravaginal torsion | Neonates | Twisting of entire cord including tunica vaginalis |
| Intravaginal torsion | Older children & adults | Twisting of cord within the tunica vaginalis |
The most common predisposing anomaly for intravaginal torsion is the bell-clapper deformity — a congenitally abnormal fixation of the tunica vaginalis to the testicle that results in increased testicular mobility within the scrotum. — Rosen's Emergency Medicine, p. 1401
Salvage Rates by Time to Detorsion
| Time from onset | Salvage rate |
|---|---|
| < 6 hours | > 90% |
| 6–24 hours | Rapidly declining |
| > 24 hours | Poor viability; orchiectomy likely |
— Rosen's Emergency Medicine, p. 1401–1402
Clinical Features
History:
- Sudden onset of intense unilateral scrotal pain, often awakening the patient from sleep
- May radiate to the lower abdomen or inguinal region
- Associated nausea and vomiting (classic)
- Pain can begin after physical activity but usually has no specific precipitant
- History of similar prior episodes (intermittent torsion) may be elicited
- Because torsion can present with abdominal pain and no scrotal pain, the scrotum must be examined in all patients with abdominal pain
Physical examination:
- High-riding testicle — shortening of the twisted spermatic cord elevates the testicle
- Transverse (horizontal) lie of the testis
- Exquisite testicular tenderness; firm on palpation
- Epididymis displaced from its posterior position
- Absent cremasteric reflex (ipsilateral testicle fails to elevate when the medial thigh is stroked) — most consistent finding, though its presence does not rule out torsion
— Rosen's Emergency Medicine, p. 1402; Sabiston Textbook of Surgery, p. 2832
Differential Diagnosis
The classic acute scrotum differential includes:
| Feature | Testicular Torsion | Appendix Torsion | Epididymitis |
|---|---|---|---|
| Age | <1 year, puberty | 7–14 years | Adult |
| Onset | Hours | 1–2 days | Days to weeks |
| Pain location | Entire testicle | Upper pole | Epididymis |
| Testicle position | High-riding, transverse | Normal, vertical | Normal, vertical |
| Systemic sx | Nausea, vomiting | None | Possibly fever |
| Cremasteric reflex | Absent | Intact | Intact |
| Pyuria | Rare | No | Yes |
| Ultrasound | Diffusely hypoechoic, ↓/absent flow, cord twist | Focally hypoechoic, normal flow | Hypoechoic epididymis, ↑ flow |
| Treatment | Surgery | Supportive | Antibiotics |
No single finding reliably differentiates torsion — when it is a diagnostic possibility, prompt urology consultation is mandatory. — Rosen's Emergency Medicine, Table 85.9
Diagnostic Testing
When to image: If history and physical strongly suggest torsion → emergent surgical consultation without delay for imaging. Imaging is for equivocal cases only.
Color Doppler ultrasound is the diagnostic modality of choice:
- Sensitivity: 96–100%; Specificity: 84–95%
- Findings: hypoechoic enlarged testis, absent or decreased arterial flow, visible spermatic cord twist ("whirlpool sign")
- False negatives occur early in the course (when some flow persists) or with intermittent torsion
- A negative ultrasound does not rule out torsion — urologic evaluation is still required if clinical suspicion is high
Urinalysis: May show pyuria in epididymitis; can occasionally be positive in torsion with concurrent UTI — not helpful for exclusion.
— Rosen's Emergency Medicine, p. 1402
Management
Immediate action
In patients with strong clinical suspicion: do not delay surgical exploration to obtain imaging or labs. — Sabiston Textbook of Surgery, p. 2832
Manual detorsion (temporizing measure)
Can be attempted at bedside while awaiting the OR. The testicle typically rotates inward (medially), so detorsion is performed by rotating it outward (laterally) — described as "opening a book." Success is indicated by pain relief. Even if successful, surgical orchiopexy is still required.
Surgical treatment
Scrotal exploration via midline or transverse scrotal incision:
- Detorsion of the spermatic cord
- Assess viability — warm the testis, observe for return of color over 5–10 minutes
- Viable testis → orchiopexy: fixation of the tunica albuginea to the inner scrotal wall with non-absorbable sutures (prevents recurrence)
- Non-viable testis → orchiectomy
- Contralateral orchiopexy is always performed at the same sitting — bell-clapper deformity is bilateral in ~80%, putting the contralateral testis at risk for asynchronous torsion
Even with suspected late-presenting torsion (days of swelling and firmness), urgent exploration is still indicated given medicolegal considerations and uncertainty about the exact duration of complete ischemia. — Sabiston Textbook of Surgery, p. 2832
Intraoperative Appearance
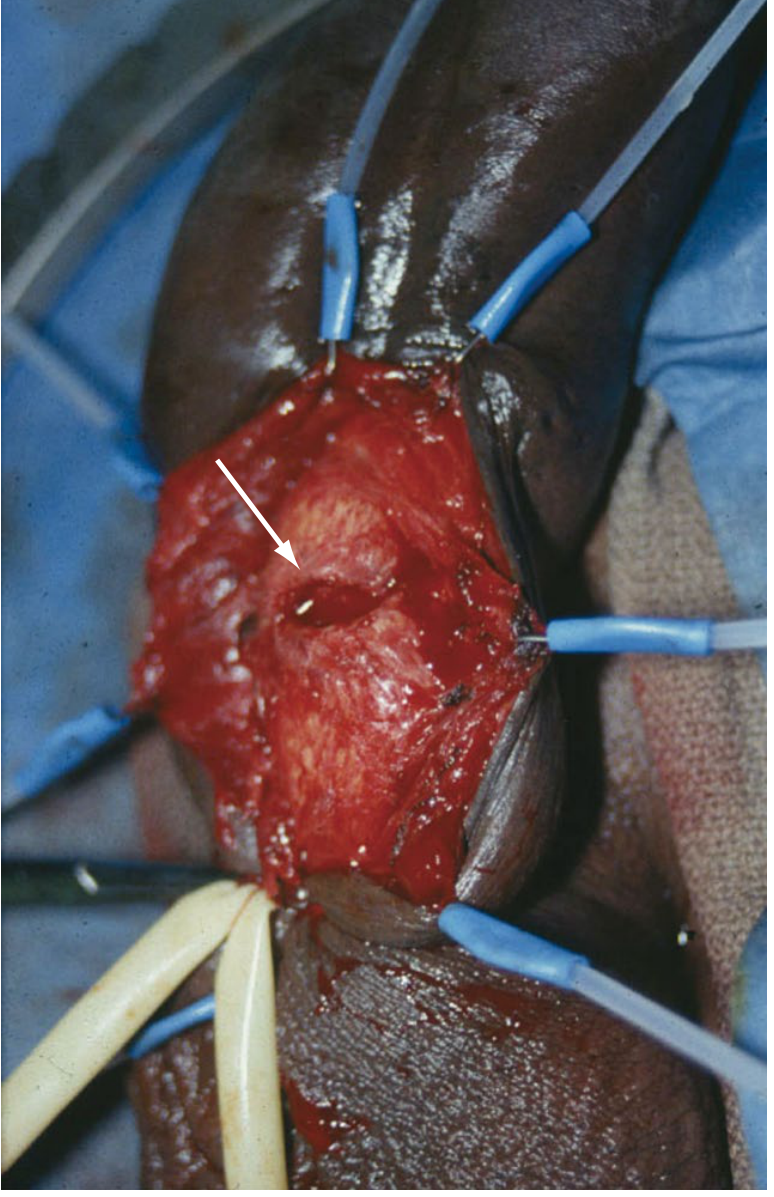
Testicular torsion — exploration through a transverse scrotal incision demonstrating the twisted cord (arrow). Note the edema, erythema, and ecchymosis after several hours of torsion. — Sabiston Textbook of Surgery, Fig. 121.11
Special Considerations: Neonatal Torsion
In neonates, torsion is almost always extravaginal. It is further divided into:
- Prenatal (in utero) torsion: Presents with a firm, non-tender, discolored, avascular testis fixed to the scrotal wall. Salvage rate is nearly zero. Contralateral orchidopexy on an urgent basis is the primary goal.
- Postnatal torsion (within first 30 days of life): Presents with acute scrotal erythema and tenderness. Salvage rate up to 44%. Treat as a surgical emergency.
— Campbell Walsh Wein Urology, p. 1696–1704
Key Teaching Points
- Testicular torsion is a surgical emergency — time to detorsion is the most critical determinant of outcome
- The bell-clapper deformity is the classic anatomical predisposition
- Always perform bilateral orchiopexy at the time of surgical exploration
- Clinical suspicion alone is sufficient to take a patient to the operating room — do not wait for ultrasound if the diagnosis is clinically apparent
- The cremasteric reflex, while useful, is neither perfectly sensitive nor specific
This is a shared conversation. Sign in to Orris to start your own chat.