When to use qSOFA and NEWS or MEWS
Reading File
Searching the Web
qSOFA vs NEWS MEWS when to use clinical scoring comparison 2024
Finding Sources
Finding Sources
Searching PubMed
qSOFA NEWS MEWS sepsis prediction comparison
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have solid textbook and web content to write a thorough answer. Here it is:
qSOFA vs NEWS vs MEWS - When to Use Each
These are three complementary early warning/screening tools, each suited to a different purpose and clinical setting.
qSOFA (Quick SOFA)
Purpose: Bedside screen for sepsis risk specifically - not a general deterioration tool.
Parameters (1 point each):
| Criterion | Threshold |
|---|---|
| Respiratory rate | ≥ 22 breaths/min |
| Altered mental status | GCS < 15 |
| Systolic blood pressure | ≤ 100 mmHg |
Score interpretation: ≥ 2 points = high risk of poor outcome from sepsis (prolonged ICU stay, higher in-hospital mortality).
When to use qSOFA:
- At the bedside in a non-ICU / ED setting when you suspect infection in a patient
- As a rapid, no-equipment screen - no labs required, calculated in seconds
- To flag patients who need urgent workup for a source of infection and possible ICU escalation
- During triage in resource-limited environments where quick decisions are needed
Limitations of qSOFA:
- Low sensitivity - it misses many sepsis cases, especially early on. The Surviving Sepsis Campaign 2021 guidelines explicitly recommend against using qSOFA alone as a single screening tool for sepsis or septic shock, because NEWS and MEWS outperform it as single screens
- Does not account for SpO2, temperature, or heart rate - important physiological signals
- Not validated for the ICU (use full SOFA there)
- Poor performance in elderly patients and those with respiratory infections
NEWS (National Early Warning Score) / NEWS2
Purpose: General physiological deterioration monitoring for any acutely ill patient on the ward, regardless of suspected diagnosis.
Parameters (weighted scoring 0-3 each):
| Parameter | Abnormal range scores higher |
|---|---|
| Respiratory rate | ≤ 8 or ≥ 25 = 3 pts |
| SpO2 (Scale 1 or 2) | ≤ 91% = 3 pts |
| Systolic blood pressure | ≤ 90 or ≥ 220 = 3 pts |
| Pulse | ≤ 40 or ≥ 131 = 3 pts |
| Consciousness (AVPU) | U or new confusion = 3 pts |
| Temperature | ≤ 35.0 or ≥ 39.1 = 2 pts |
| Supplemental oxygen | Any oxygen = 2 pts |
Maximum score: 20. NEWS2 adds a modified SpO2 scale for hypercapnic respiratory failure (e.g. COPD patients).
Score thresholds and response:
| Score | Risk | Action |
|---|---|---|
| 0 | Low | Routine obs (≥12 hourly) |
| 1-4 | Low-medium | Increase monitoring frequency |
| 5-6 or 3 in any single parameter | Medium | Urgent clinical review |
| ≥7 | High | Immediate emergency response |
When to use NEWS/NEWS2:
- Continuous ward monitoring of all admitted patients - not sepsis-specific
- Standard across all NHS hospitals; recommended by the Royal College of Physicians
- Any patient whose condition may be deteriorating, regardless of cause (heart failure, PE, GI bleed, post-op complications, etc.)
- When you need a score with higher sensitivity than qSOFA to catch more cases early
- For sepsis screening, NEWS ≥5 has better sensitivity than qSOFA ≥2, and the Surviving Sepsis Campaign 2021 recommends NEWS or MEWS over qSOFA as a single sepsis screening tool
- Research shows NEWS/NEWS2 and qSOFA have similar AUROC for 28-day mortality prediction, but NEWS has better sensitivity at commonly used thresholds
MEWS (Modified Early Warning Score)
Purpose: Similar to NEWS - a simpler, general early warning score for deteriorating patients.
Parameters:
| Parameter | Measured |
|---|---|
| Respiratory rate | ≥ 30 = 3 pts |
| SBP | ≤ 70 = 3 pts |
| Heart rate | ≥ 130 = 3 pts |
| AVPU consciousness | U = 3 pts |
| Temperature | ≤ 35.0 = 2 pts |
When to use MEWS:
- Low-resource or district hospital settings where full NEWS implementation is not feasible
- Recommended by the WHO for hospitals in resource-limited settings
- Post-operative monitoring for early warning of complications
- MEWS ≥5 is commonly used as a trigger threshold
- Simpler than NEWS (fewer parameters, no SpO2 required) - better suited where pulse oximetry is unavailable
- Performance is comparable to NEWS in some datasets (no statistically significant difference in AUROC, p=0.563 per recent ED studies)
Head-to-Head Summary
| Feature | qSOFA | NEWS/NEWS2 | MEWS |
|---|---|---|---|
| Parameters | 3 (RR, SBP, AMS) | 7 (includes SpO2, temp, HR, O2) | 5 (RR, SBP, HR, AVPU, temp) |
| Purpose | Sepsis screening only | Any deterioration + sepsis | Any deterioration + sepsis |
| Setting | ED / non-ICU | All ward settings | Low-resource / wards |
| Speed | Fastest (no equipment) | Moderate (needs SpO2) | Fast |
| Sensitivity for sepsis | Lower | Higher | Moderate |
| Specificity | Higher | Lower | Moderate |
| Guideline recommendation | Not sole screen (SSC 2021) | Preferred over qSOFA alone | Alternative to NEWS |
Practical Clinical Guidance
-
On the general ward: Use NEWS/NEWS2 routinely for all patients. It is your primary safety net for any deterioration.
-
When you suspect infection (ED or ward): Use qSOFA as a rapid 3-second bedside check. A score ≥2 should heighten your concern and prompt sepsis workup. But do not use it alone to rule out sepsis - a negative qSOFA does not exclude it.
-
Per Surviving Sepsis Campaign 2021: If you can only use one tool to screen for sepsis, choose NEWS or MEWS over qSOFA - they have better sensitivity.
-
In resource-limited or rural settings: MEWS is a pragmatic alternative when SpO2 monitoring is unavailable.
-
In the ICU: Neither qSOFA nor NEWS applies - use the full SOFA score (which requires labs: bilirubin, creatinine, PaO2/FiO2, platelets, vasopressor doses) to track organ dysfunction.
-
In pregnant patients: Standard qSOFA and NEWS thresholds are unreliable - normal pregnancy physiology includes tachycardia and mild hypotension; the Sepsis-3 criteria have not been modified for obstetric patients.
Sources:
- Sabiston Textbook of Surgery, 21st ed. - Septic Shock chapter, noting the SSC 2021 recommendation against qSOFA as sole screen
- Harrison's Principles of Internal Medicine 22E (2025) - SOFA Scoring and Recognizing Sepsis sections
- Rosen's Emergency Medicine - Sepsis Background
- Bailey and Love's Short Practice of Surgery, 28th ed. - NEWS2 chart and postoperative monitoring
- Recent ED study (2024): Validation of MEWS, NEWS, NEWS2, and qSOFA for different infection foci - no significant difference between NEWS2 and MEWS (p=0.563) or NEWS2 and qSOFA (p=0.314) for ICU stay prediction
- Systematic review (White Rose): qSOFA vs NEWS/MEWS for sepsis prediction - NEWS trended higher AUROC than qSOFA at common thresholds due to more variables
Use of NEWS/MEWS as per surviving sepsis campaign 2026
Searching the Web
Surviving Sepsis Campaign 2026 guidelines NEWS MEWS screening
Searching the Web
Surviving Sepsis Campaign guidelines 2025 2026 update sepsis screening tools
Searching PubMed
surviving sepsis campaign guidelines 2025
Reading Web Page
NEWS MEWS qSOFA screening sepsis recommendation
I have everything needed from the official SSC 2026 source. Here is a focused, guideline-accurate answer:
NEWS/MEWS as per the Surviving Sepsis Campaign 2026
The SSC 2026 guidelines were published on March 23, 2026 in Critical Care Medicine and Intensive Care Medicine, developed by a 69-member international panel. They contain 129 recommendations (46 new or revised). The screening section is directly relevant here.
Recommendation 4 - Screening for Sepsis in Hospital
"For acutely ill patients in hospital, we RECOMMEND using NEWS, NEWS2, MEWS, or SIRS over qSOFA as a single tool to screen for sepsis." - Strong recommendation, moderate certainty evidence (Revisited from SSC 2021)
This is the core statement. It upgrades from the 2021 "suggest against qSOFA alone" to an explicit strong recommendation in favor of NEWS/NEWS2/MEWS/SIRS over qSOFA.
Recommendation 3 - Prehospital Screening (NEW in 2026)
"In acutely ill adults en route to hospital by ambulance or flight, we SUGGEST using a standard sepsis screening tool over not using a screening tool." - Conditional recommendation, very low certainty evidence (New)
This is a brand-new recommendation - the 2021 guidelines did not address prehospital screening. The panel stopped short of specifying which tool to use in the prehospital setting (because NEWS2's difficulty of use in that environment led them to withhold a specific tool endorsement there), but they validated the concept of systematic screening before hospital arrival.
Why NEWS/NEWS2 and MEWS are Preferred Over qSOFA - The Evidence Base
The SSC 2026 rationale cites four systematic reviews and meta-analyses, plus a landmark cohort study:
| Evidence | Finding |
|---|---|
| Large cohort (n > 221,000) | NEWS2 had the best absolute test performance for sepsis: sensitivity 73.1% (95% CI 71.8-74.4%), AUC 0.77 (95% CI 0.71-0.83) |
| vs MEWS | NEWS2 > MEWS for sensitivity and AUC |
| vs SIRS | NEWS2 > SIRS |
| vs qSOFA | All EWS (NEWS, NEWS2, MEWS, SIRS) were more sensitive for diagnosing sepsis than qSOFA across 4 systematic reviews/meta-analyses |
| SCREEN Trial (JAMA 333:763) | Electronic qSOFA-based alerting (not manual qSOFA alone) with nurse/physician response improved 90-day in-hospital mortality - showing it's the system, not just the score, that matters |
Key acknowledged limitation of NEWS2: Lower specificity (81.6%), high false-positive rate (PPV only 6.5%) - which means many patients flagged will not have sepsis. This is acceptable for a screening tool (you want high sensitivity), but clinicians must not act on a high NEWS2 score alone without clinical judgment.
What This Means Practically
| Setting | SSC 2026 Guidance |
|---|---|
| Acutely ill patients in hospital wards | Use NEWS, NEWS2, MEWS, or SIRS - strong recommendation |
| Emergency department | Same - NEWS/MEWS preferred over qSOFA alone |
| Prehospital (ambulance/flight) | Use any standard sepsis screening tool (conditional) - specific tool not mandated |
| qSOFA | Still useful to alert clinicians to the possibility of sepsis in any resource setting, but not recommended as the sole tool due to poor sensitivity |
| Electronic alert systems (e.g. e-qSOFA) | Supported - the SCREEN Trial showed mortality benefit from systematic electronic screening + triggered response |
2021 vs 2026 - What Changed on Screening
| Aspect | SSC 2021 | SSC 2026 |
|---|---|---|
| qSOFA as sole screen | "Suggest against" (weak) | "Recommend against" (strong) |
| NEWS/MEWS preferred | Suggested | Strongly recommended |
| Prehospital screening | Not addressed | New conditional recommendation added |
| Electronic screening systems | Not addressed | Supported (SCREEN Trial evidence) |
Important Caveat from the Panel
The SSC 2026 explicitly states: "There is no ideal tool to screen for sepsis that has both high sensitivity and specificity." The guidance is to use a structured tool systematically - the choice between NEWS2, MEWS, and SIRS should be guided by:
- Local availability of parameters (NEWS2 requires SpO2 and temperature monitoring)
- Resource setting (MEWS is more feasible in low/middle-income countries or where pulse oximetry is unavailable)
- Institution's existing workflows and alert systems
Sources:
- SSC 2026 - Intensive Care Medicine (Springer), published March 23, 2026 - Recommendation 4 (strong, moderate evidence)
- Epocrates SSC 2026 Summary, April 2026
- SCREEN Trial: electronic sepsis screening with qSOFA alert - JAMA 333:763-773
What is GDMT
Finding Sources
Searching the Web
GDMT guideline directed medical therapy heart failure 2024 2025 four pillars
Reading File
Reading File
Loading Image
Here is a complete answer on GDMT:
GDMT - Guideline-Directed Medical Therapy
GDMT refers to the combination of evidence-based medications - and sometimes devices - proven to reduce morbidity and mortality in heart failure, prescribed and optimized according to major society guidelines (primarily the 2022 AHA/ACC/HFSA Heart Failure Guidelines). The term is most commonly applied to HFrEF (Heart Failure with Reduced Ejection Fraction, EF < 40%), where it has the strongest mortality benefit.
The Four Pillars of GDMT for HFrEF
These are all Class I (strong) recommendations:
| Pillar | Drug Class | Key Agents | Landmark Trial(s) |
|---|---|---|---|
| 1 | ARNI (preferred) or ACE-I or ARB | Sacubitril/valsartan (ARNI); Enalapril, lisinopril (ACEi); Valsartan, candesartan (ARB) | PARADIGM-HF (ARNI), CONSENSUS, SOLVD (ACEi) |
| 2 | Beta-blocker (evidence-based only) | Metoprolol succinate, carvedilol, bisoprolol | MERIT-HF, COPERNICUS, CIBIS-II |
| 3 | MRA (Mineralocorticoid Receptor Antagonist) | Spironolactone, eplerenone | RALES, EMPHASIS-HF |
| 4 | SGLT2 inhibitor | Dapagliflozin, empagliflozin | DAPA-HF, EMPEROR-Reduced |
A meta-analysis of 95,444 HFrEF patients showed that a 70-year-old receiving all four pillars (ARNI + beta-blocker + MRA + SGLT2i) gains an estimated 5 additional life-years compared to placebo - CFR Journal, 2025.
Why These Four? The Pathophysiological Rationale
Heart failure activates several maladaptive compensatory mechanisms. GDMT targets each one:
| Mechanism activated in HF | GDMT targeting it |
|---|---|
| RAAS activation (angiotensin II, aldosterone) | ACEi / ARB / ARNI / MRA |
| Sympathetic nervous system overactivation | Beta-blockers |
| Natriuretic peptide degradation | ARNI (neprilysin inhibitor component) |
| Ventricular remodeling and fibrosis | All four classes |
| Cardiorenal syndrome, inflammation, metabolic stress | SGLT2 inhibitors |
Where GDMT Fits in the ACC/AHA Heart Failure Staging System
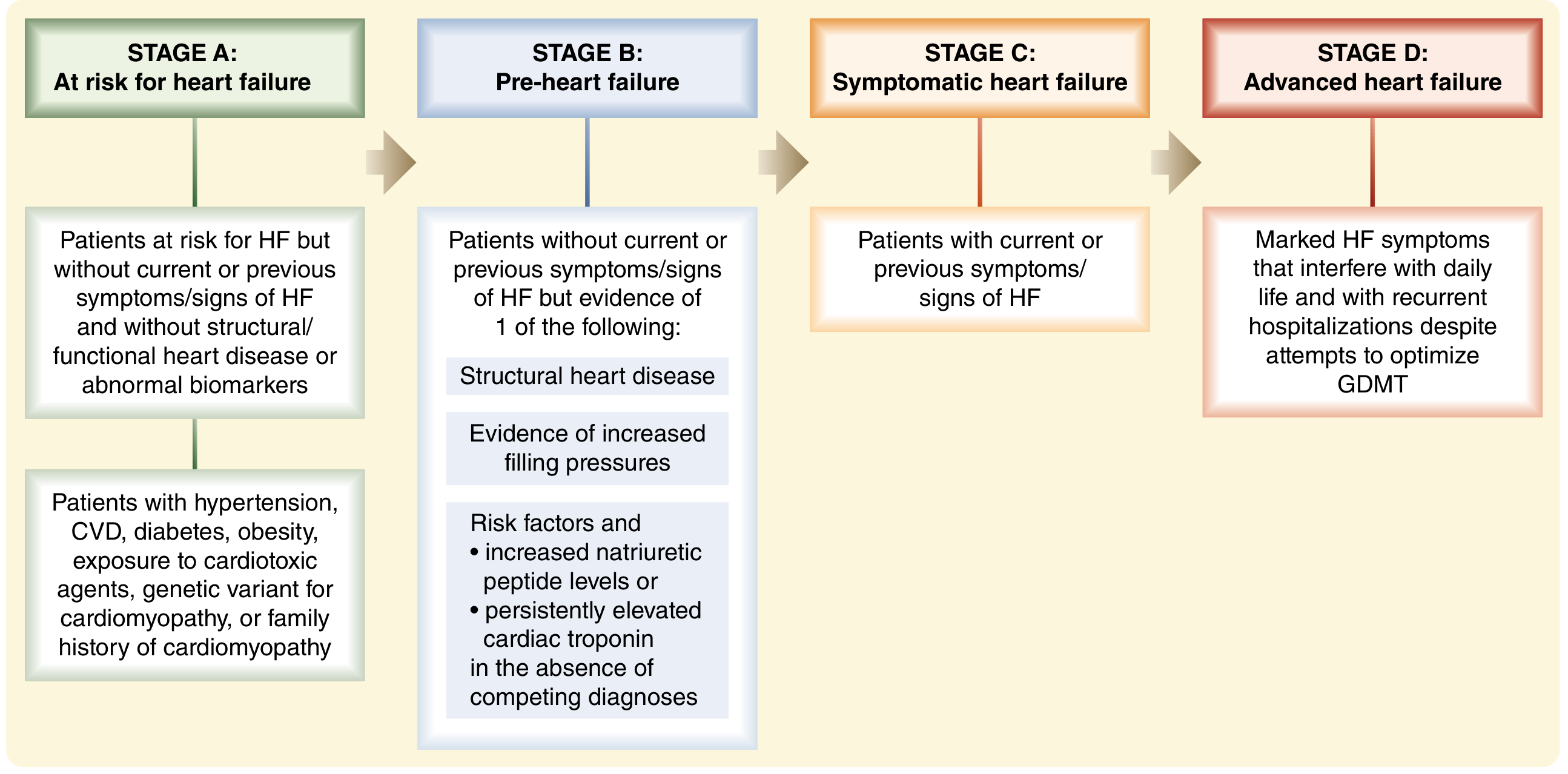
- Stage A (at risk): Risk factor modification, no GDMT yet
- Stage B (pre-HF, structural disease but no symptoms): Some GDMT agents (ACEi/beta-blocker in post-MI with reduced EF)
- Stage C (symptomatic HFrEF): Full four-pillar GDMT is the cornerstone of treatment
- Stage D (advanced HF, refractory to GDMT): Consider durable LVAD or heart transplantation
Stage D is defined as HF that is refractory to optimized GDMT, with marked symptoms interfering with daily life and recurrent hospitalizations. - Sabiston Textbook of Surgery, 21st ed.
Additional Therapies (Used After Optimizing GDMT)
These have mortality/morbidity benefit in select subgroups but are add-ons, not the core pillars:
| Agent/Device | When to Consider |
|---|---|
| Hydralazine + isosorbide dinitrate | ACEi/ARB/ARNI intolerant patients (especially self-identified Black patients - A-HeFT trial) |
| Ivabradine | HR ≥70 bpm on max beta-blocker, EF ≤35%, sinus rhythm |
| Vericiguat | Worsening HF despite GDMT (VICTORIA trial) |
| ICD (implantable defibrillator) | EF ≤35%, NYHA II-III, ≥3 months GDMT - reduces sudden cardiac death |
| CRT (cardiac resynchronization therapy) | EF ≤35%, LBBB, QRS ≥150 ms - improves function and mortality |
| TEER (MitraClip) | Secondary MR with advanced HF despite GDMT |
GDMT in HFpEF (EF ≥ 50%) - Evolving Evidence
Until recently, only diuretics for symptom relief had good evidence in HFpEF. The picture has changed:
- SGLT2 inhibitors (empagliflozin - EMPEROR-Preserved; dapagliflozin - DELIVER): Now have Class IIa/IIb recommendation in HFpEF - reduce HF hospitalizations
- MRAs (spironolactone - TOPCAT): Post-hoc data suggests benefit in certain subgroups
- ARBs/ARNIs: Some benefit in HFmrEF (EF 41-49%); less clear in HFpEF
Key Clinical Points
- All four pillars should be started together (or in rapid succession) - there is strong evidence that early initiation of all four, rather than sequential titration over months, is preferred per current guidelines
- Optimize doses - underdosing is a major real-world problem; the mortality benefit is dose-related
- ARNI is preferred over ACEi/ARB when tolerated - do not combine with ACEi; wait 36 hours when switching from ACEi to ARNI
- GDMT takes priority over device therapy - devices (ICD, CRT) should only be considered after ≥3 months of optimized GDMT, as EF may recover
- qSOFA vs GDMT note: In the surgical context, patients with functional/secondary mitral regurgitation should receive GDMT (ACEi, diuretics, cardiac resynchronization) before considering valve intervention - Sabiston Textbook of Surgery
Sources:
This is a shared conversation. Sign in to Orris to start your own chat.