Lung anatomy and physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have comprehensive, high-quality content from multiple authoritative sources. Let me compile the full answer.
Lung Anatomy and Physiology
Overview
The lung has two essential, interdependent functions: ventilation-perfusion matching to deliver O₂ to the body and remove CO₂, and host defense against airborne pathogens, chemicals, and particulates. Secondary functions include surfactant synthesis and recycling, mucociliary clearance, neuroendocrine signaling, and synthesis of myriad molecules by epithelial and endothelial cells.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 32
Part 1: Gross Anatomy
Overall Dimensions and Weight
In life, the human lungs weigh 900-1000 g, of which nearly 40-50% is blood. At end-expiration (FRC), the gas volume is about 2.5 L; at maximal inspiration it may reach 6 L. Overall lung density varies from 0.30 g/mL at FRC to 0.14 g/mL at total lung capacity (TLC). Lung density is non-uniform: approximately 1 g/mL near the hilum and 0.1 g/mL peripherally. More than 50% of all alveoli are located in the outer 30% of the lung radius (from hilum to chest wall).
The height of the lungs at FRC on a chest X-ray is approximately 24 cm, with the bifurcation of the pulmonary artery about halfway up.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 33
Lobar and Segmental Organization
| Side | Lobes | Key Features |
|---|---|---|
| Right | 3 (upper, middle, lower) | Separated by oblique and horizontal fissures |
| Left | 2 (upper, lower) | Separated by oblique fissure only; lingula = equivalent of right middle lobe |
The right lung has three secondary bronchi (upper, middle, lower lobar bronchi), and the left has two, directly foreshadowing the lobar count on each side. Each lobe is further divided into bronchopulmonary segments - each supplied by its own segmental bronchus and pulmonary artery branch, making them resectable units.
- Langman's Medical Embryology, p. 658
The Tissue Compartments (Composition)
The lung is composed of:
- Airspace: ~80% of total lung volume at FRC
- Alveolar walls: remarkably thin (minimizing diffusion distance for O₂)
- Vasculature and interstitium: collagen, elastin, and proteoglycans/glycosaminoglycans form the extracellular matrix scaffold; the matrix also regulates epithelial phenotype and cytokine signaling
The interstitial space contains collagen (tensile strength), elastin (elastic recoil), and proteoglycans whose glycosaminoglycan side chains create a gel-like structure.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 35
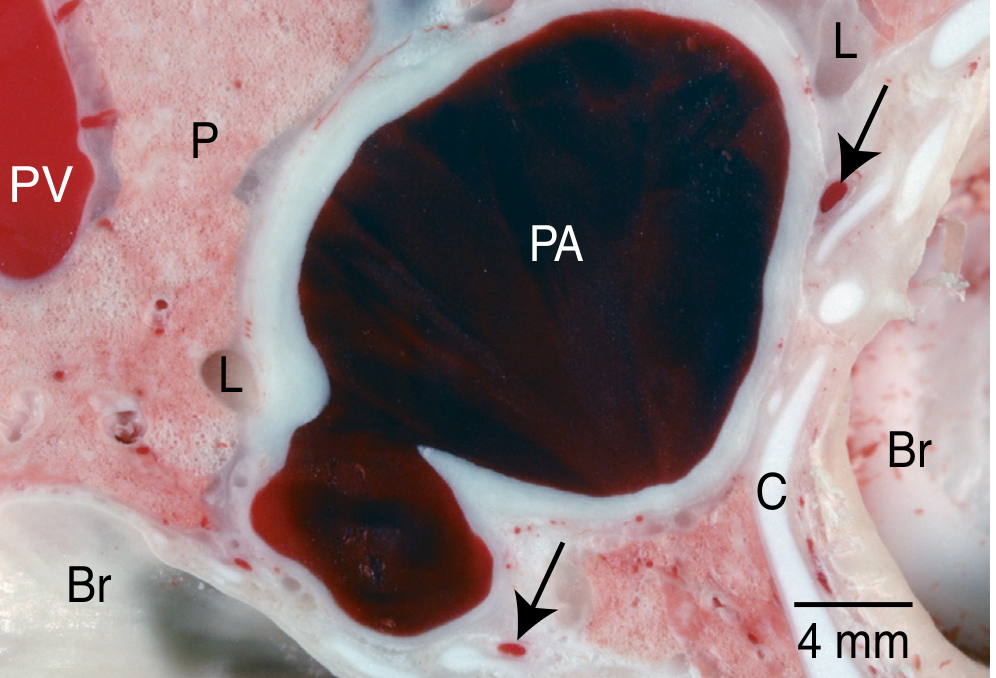
Figure: Frozen block of lung tissue. Pulmonary arterial (PA) blood is dark purple (deoxygenated); pulmonary venous (PV) blood is crimson (oxygenated). Bronchus (Br), parenchyma (P), lymphatics (L), and cartilage (C) are also labeled. (Murray & Nadel's)
Part 2: The Airways
Conducting Airways (Generations 0-16)
The trachea (generation 0) divides at the carina into right and left main bronchi. The right main bronchus is shorter, wider, and more vertical - the reason inhaled foreign bodies preferentially enter the right lung.
- Bronchi (generations 1-4): Supported by C-shaped cartilaginous rings or cartilaginous plates; lined by pseudostratified columnar epithelium with cilia and goblet cells; wall layers = mucosa, lamina propria, smooth muscle, submucosa with seromucous glands, and cartilage
- Bronchioles (generations 5-16): No cartilage; smooth muscle increases in relative proportion; epithelium transitions from ciliated columnar to cuboidal
- Terminal bronchioles (generation ~16): The last purely conducting airway; lined predominantly by ciliated epithelium (CE) and non-ciliated club cells (formerly Clara cells), which have secretory ultrastructure (rough ER, Golgi, membrane-bound granules) and produce club cell secretory protein (CC16)
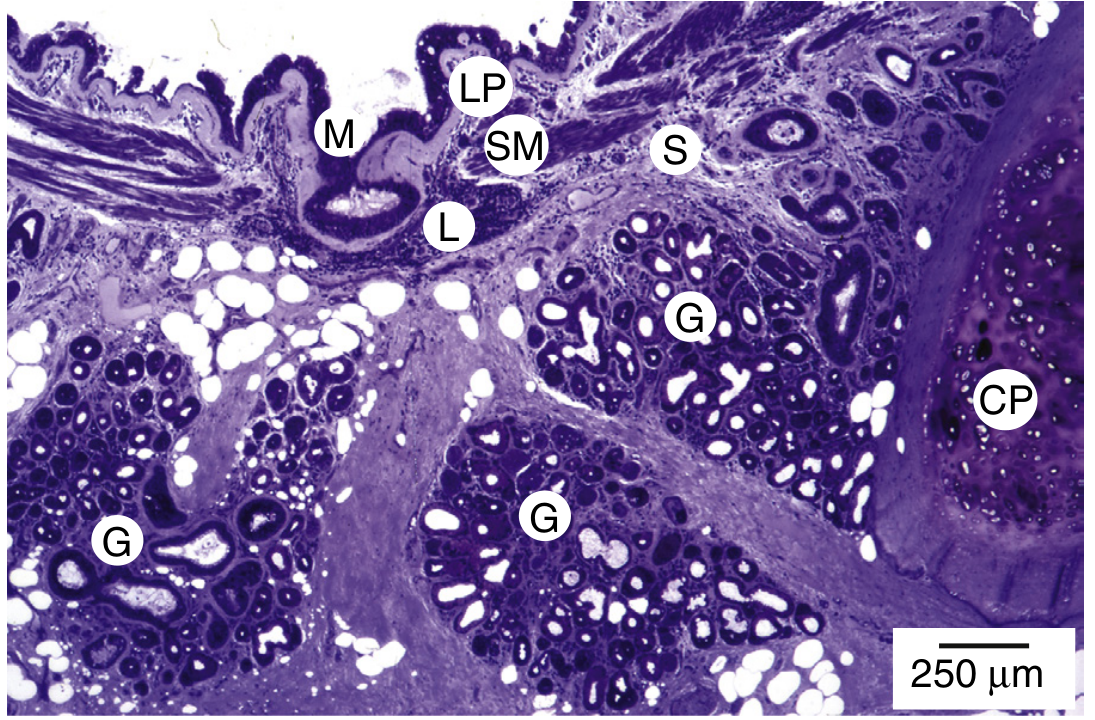
Figure: Bronchial wall histology showing all structural layers. Note the prominent seromucous glands (G) and cartilaginous plates (CP). (Murray & Nadel's, right middle lobar bronchus)
Mucociliary Escalator
Each ciliated cell bears ~200 cilia with a ciliary crown (clawlike cap making the distal portion stiff). Cilia beat in coordinated, directional strokes at 8-15 Hz, propelling the mucus blanket centripetally toward the pharynx. As airways taper, the total perimeter decreases, and much of the liquid lining layer is reabsorbed during its ascent.
Goblet cells produce mucus stored in ~800 nm granules. Mucus provides the viscoelastic gel layer that traps inhaled particles, which are then swept by cilia toward the pharynx for swallowing or expectoration.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 44
Respiratory Airways (Generations 17-23)
Beyond the terminal bronchiole lie:
| Structure | Feature |
|---|---|
| Respiratory bronchioles (gen. 17-19) | First airways with alveoli in their walls |
| Alveolar ducts (gen. 20-22) | Walls almost entirely alveoli |
| Alveolar sacs (gen. 23) | Blind-ending clusters of alveoli |
Part 3: The Terminal Respiratory Unit (TRU) and Alveoli
Terminal Respiratory Unit
The TRU (also called the physiologist's acinus) consists of a respiratory bronchiole plus all subsequent alveolar ducts and alveoli. Key facts:
- Each TRU contains ~100 alveolar ducts and ~2,000 alveoli
- At FRC, one TRU is approximately 5 mm in diameter, volume ≈ 0.02 mL
- There are ~150,000 TRUs in normal adult human lungs
- Gas-phase diffusion within the TRU is so rapid that partial pressures of O₂ and CO₂ are uniform throughout the unit - this defines its functional boundary
The total alveolar surface area is approximately 70-80 m² (the size of a tennis court), with an alveolar-capillary barrier only ~0.5 µm thick on its thin side.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 265
Air-Blood Barrier (Gas Exchange)
The barrier from alveolar air to red blood cell (RBC) cytoplasm consists of:
- Type I alveolar epithelium (squamous, covers 97% of alveolar surface)
- Epithelial basement membrane
- Fused basal laminae (interstitium, in the thin side)
- Capillary endothelium
- Plasma
- RBC membrane and cytoplasm
The thin side of the barrier has fused basal laminae - minimizing diffusion distance. The thick side has accumulated elastin, collagen, and matrix separating epithelium from endothelium - providing structural support and containing interstitial fluid.
CO₂ is 20 times more soluble in water than O₂, so it diffuses rapidly across the barrier even though the driving pressure (CO₂ gradient) is only ~1/10 that for O₂.
Part 4: Cellular Anatomy
Alveolar Lining Cells
| Cell Type | Proportion | Function |
|---|---|---|
| Type I pneumocytes | Cover 97% of surface area | Gas exchange (thin, squamous); structurally vulnerable |
| Type II pneumocytes | Only 3-5% of surface, but 60% of cells by number | Produce surfactant (lecithin/dipalmitoyl phosphatidylcholine); repair type I cells after injury; ion transport |
Surfactant reduces alveolar surface tension, preventing alveolar collapse at end-expiration. It works because surface tension decreases as alveolar radius shrinks (surfactant molecules pack closer together), counteracting the tendency of small alveoli to collapse per the Laplace relationship (P = 2T/r).
Alveolar Macrophages
Resident phagocytes derived from blood monocytes, these are the primary defense cells of the alveolar space. They ingest inhaled particles, bacteria, and cellular debris, and can modulate inflammatory responses.
Airway Lining Cells
- Ciliated cells: Mucociliary clearance
- Goblet cells: Mucus secretion
- Club cells: Bronchiolar secretion (CC16 protein), metabolism of inhaled toxicants
- Basal cells: Stem cells for airway epithelial renewal
- Neuroendocrine cells: Dense-cored vesicles; signaling functions; organized into neuroepithelial bodies at airway bifurcations
Part 5: Circulation
Pulmonary Circulation
The pulmonary circulation is a low-pressure, high-flow, low-resistance circuit:
- Normal mean pulmonary artery pressure: ~15 mmHg (vs. ~95 mmHg systemic)
- The entire cardiac output (~5 L/min) passes through the lungs at any given time
- Pulmonary capillary transit time: ~0.75 sec at rest (sufficient for complete O₂ equilibration); decreases to ~0.25 sec during heavy exercise
- Blood flow distribution is gravity-dependent, giving rise to three classic West's zones:
- Zone 1 (apex): PA > Pa > Pv (alveolar pressure exceeds arterial - occurs only in pathology or during positive-pressure ventilation; dead space)
- Zone 2 (mid): Pa > PA > Pv (flow driven by arterial-alveolar pressure difference; "Starling resistor")
- Zone 3 (base): Pa > Pv > PA (flow driven by arteriovenous pressure difference; continuously perfused; highest flow)
Bronchial Circulation
A separate systemic circulation from the bronchial arteries (branches of the descending aorta or intercostal arteries) supplies the airway walls from the trachea to the respiratory bronchioles. Bronchial venous blood drains partly into the azygous system and partly via bronchopulmonary anastomoses directly into the pulmonary veins (contributing to the physiological shunt).
Lymphatics
The lung has an extensive lymphatic network running in the peribronchovascular connective tissue spaces and in the interlobular septa. Lymph flows centrally toward the hilum. The interlobar lymph nodes form the "lymphatic sump of Borrie," draining all lobes on each side.
- Schwartz's Principles of Surgery, p. 947
Part 6: Pleura
The lungs are enclosed by a double-layered pleural membrane:
- Visceral pleura: Tightly adherent to the lung surface; supplied by bronchial (systemic) vessels
- Parietal pleura: Lines the chest wall, diaphragm, and mediastinum; has pain receptors
The pleural space in health is only several micrometers wide (a potential space), maintained by the opposing elastic recoil forces of the lung (tending to collapse) and chest wall (tending to expand). The resting pleural pressure is subatmospheric (approximately -5 cmH₂O at FRC).
The pleural fluid is a thin serous film providing lubrication during breathing.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 33
Part 7: Physiology of Ventilation
Mechanics of Breathing
During inspiration:
- Diaphragm contracts and descends; external intercostals pivot the ribs outward
- Thoracic cavity expands → pleural pressure becomes more negative
- Transpulmonary pressure gradient increases → air flows into alveoli (tidal volume, VT)
- Decreased intrathoracic pressure (ITP) also increases venous return (VR) to the right heart
During expiration (normally passive):
- Respiratory muscles relax
- Elastic recoil of previously expanded parenchyma drives gas out
- ITP increases → slight decrease in RV stroke volume
Normal breathing: more time in expiration (Te) than inspiration (Ti), because a compliant lung fills rapidly and needs little time for gas entry.
- Fischer's Mastery of Surgery, p. 264
Compliance
Compliance (C) = ΔV/ΔP (change in volume per change in pressure). Normal pulmonary compliance is 100-150 mL/cmH₂O. Compliance is reduced in pulmonary fibrosis and increased in emphysema.
Lung Volumes and Capacities
| Volume/Capacity | Definition | Normal Value |
|---|---|---|
| Tidal volume (VT) | Volume per normal breath | 500 mL |
| Inspiratory reserve volume (IRV) | Extra volume above VT at max inspiration | ~3000 mL |
| Expiratory reserve volume (ERV) | Extra volume expelled below VT at max expiration | ~1200 mL |
| Residual volume (RV) | Volume remaining after maximal expiration (not measurable by spirometry) | ~1200 mL |
| Inspiratory capacity (IC) | VT + IRV | ~3500 mL |
| Functional residual capacity (FRC) | ERV + RV; resting end-expiratory position where lung and chest wall recoil forces are equal | ~2400 mL |
| Vital capacity (VC) | IRV + VT + ERV | ~4700 mL |
| Total lung capacity (TLC) | All volumes combined | ~6000 mL |
RV and FRC (and any capacity containing RV) cannot be measured by simple spirometry - they require body plethysmography (most accurate), helium dilution, or nitrogen washout.
FRC is the key physiological resting volume: it is the point where the inward elastic recoil of the lung exactly equals the outward elastic recoil of the chest wall.
- Goldman-Cecil Medicine, p. 1621
Minute and Alveolar Ventilation
Minute ventilation (VE) = VT × respiratory rate
Normal ≈ 6-8 L/min (0.5 L × 12-15 breaths/min)
Normal ≈ 6-8 L/min (0.5 L × 12-15 breaths/min)
Alveolar ventilation (VA) corrects for dead space:
VA = (VT - VD) × Rate
VA = (VT - VD) × Rate
The physiological dead space (VD, ~150 mL or ~30% of VT) includes:
- Anatomical dead space: Conducting airways (trachea to terminal bronchioles) that are ventilated but do not participate in gas exchange
- Alveolar dead space: Ventilated alveoli that are not perfused (minimal in healthy lungs)
The alveolar ventilation equation is the fundamental relationship of respiratory physiology:
PACO₂ = (VCO₂ × K) / VA
This shows that alveolar PCO₂ is inversely proportional to alveolar ventilation - doubling VA halves PACO₂. This is why hyperventilation reduces PaCO₂ and hypoventilation raises it.
- Costanzo Physiology, p. 1672
Part 8: Gas Exchange
Diffusion
O₂ moves from alveolar gas (PAO₂ ≈ 100 mmHg) across the air-blood barrier into pulmonary capillary blood (mixed venous PO₂ ≈ 40 mmHg). CO₂ moves in the reverse direction (mixed venous PCO₂ ≈ 46 mmHg → alveolar PACO₂ ≈ 40 mmHg).
Normal values:
| Parameter | Value |
|---|---|
| Inspired PO₂ (at sea level) | 160 mmHg |
| Alveolar PAO₂ | 100 mmHg |
| Arterial PaO₂ | 100 mmHg |
| Alveolar PACO₂ | 40 mmHg |
| Arterial PaCO₂ | 40 mmHg |
O₂ diffusion is not normally rate-limiting, except during heavy exercise at high altitude when capillary transit time is shortened by high cardiac output.
Ventilation/Perfusion (V/Q) Matching
The V/Q ratio is the most important determinant of gas exchange efficiency.
- Normal V/Q = 0.8 (alveolar ventilation ~4 L/min, pulmonary blood flow ~5 L/min)
- Both ventilation and perfusion increase from apex (zone 1) to base (zone 3) in the upright lung due to gravity
- But perfusion increases proportionally more than ventilation → V/Q is highest at the apex (~3.3) and lowest at the base (~0.6)
- Zone 1 (apex): High V/Q → high PaO₂, low PaCO₂
- Zone 3 (base): Low V/Q → lower PaO₂, higher PaCO₂
| V/Q Extreme | Cause | Effect |
|---|---|---|
| V/Q = 0 (shunt) | Perfused but not ventilated | Venous blood enters systemic circulation; causes hypoxemia that does not correct with supplemental O₂ |
| V/Q = ∞ (dead space) | Ventilated but not perfused | Wasted ventilation; causes hypercapnia |
V/Q mismatch is the most common cause of hypoxemia in clinical practice (e.g., pneumonia, COPD, pulmonary embolism).
- Costanzo Physiology, p. 2833-2860
Hypoxic Pulmonary Vasoconstriction (HPV)
When a lung region is poorly ventilated (low PAO₂), the local pulmonary arterioles constrict, diverting blood to better-ventilated areas. This is a protective reflex that optimizes V/Q matching and is the opposite of how systemic vessels behave. Conditions that impair HPV (e.g., volatile anesthetics, nitric oxide) worsen V/Q mismatch.
Part 9: Control of Breathing
Breathing is controlled by a respiratory center in the brainstem (pons and medulla):
- Medullary center: Sets the basic respiratory rhythm via the pre-Botzinger complex
- Apneustic center (lower pons): Prolongs inspiration
- Pneumotaxic center (upper pons): Limits inspiration, increases rate
Chemical control:
- Central chemoreceptors (ventral medulla): Respond to changes in CSF pH (reflect PaCO₂); CO₂ is the most potent stimulus to breathing
- Peripheral chemoreceptors (carotid and aortic bodies): Respond to decreased PaO₂ (<60 mmHg), increased PaCO₂, and decreased pH
In chronic hypercapnia (e.g., severe COPD), central chemoreceptors are reset. Peripheral chemoreceptors (hypoxic drive) become the primary stimulus - the "hypoxic drive" concept.
Part 10: Non-Respiratory Functions of the Lung
The lung is also a metabolically active organ:
| Function | Details |
|---|---|
| Angiotensin conversion | Pulmonary endothelial ACE converts angiotensin I → angiotensin II |
| Bradykinin inactivation | ~80% inactivated in one pulmonary pass |
| Serotonin clearance | Taken up and inactivated by pulmonary endothelium |
| Prostaglandin metabolism | PGE₁, PGE₂, PGF₂α inactivated; prostacyclin (PGI₂) passes through |
| Filter function | Filters small blood clots, fat emboli, and tumor cells before they reach systemic circulation |
| Reservoir | Acts as a blood reservoir for the left heart |
Summary Diagram (Conceptual)
TRACHEA
↓
Main Bronchi (L & R)
↓
Lobar Bronchi (3R, 2L)
↓
Segmental Bronchi (10 per lung)
↓ conducting zone (dead space, generations 0–16)
Terminal Bronchioles
↓ ← transition zone
Respiratory Bronchioles (gen. 17–19)
↓
Alveolar Ducts (gen. 20–22) } Terminal Respiratory Unit
↓ } (gas exchange zone)
Alveolar Sacs & Alveoli }
← ~300 million alveoli, ~70-80 m² surface area →
Key Sources:
- Murray & Nadel's Textbook of Respiratory Medicine - Chapters 1 (Anatomy), pp. 32-50
- Costanzo Physiology, 7th Edition - Chapter 5 (Respiratory Physiology)
- Goldman-Cecil Medicine - Chapter 73 (Lung Volumes)
- Fischer's Mastery of Surgery, 8th ed. - Normal Pulmonary Physiology, p. 264
- Schwartz's Principles of Surgery, 11th ed. - Thoracic Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.