I now have everything needed. Here are your complete, exam-ready notes on Atelectasis:
🫁 ATELECTASIS
Complete Study Notes | Medical Surgical Nursing | 3rd Semester (INC/BFUHS Syllabus)
SECTION 1: DEFINITION
Atelectasis (from Greek: ateles = incomplete + ektasis = expansion) is defined as the loss of lung volume caused by inadequate expansion of air spaces, resulting in collapse of previously inflated lung tissue (or failure of neonatal lung to expand at birth).
- The affected lung continues to receive blood (perfusion) but has NO ventilation
- This creates a Ventilation-Perfusion (V/Q) mismatch leading to hypoxemia (low oxygen in blood)
- Also called Collapse of the lung
- It may involve an entire lung, a lobe, a segment, or a subsegment
Simple definition for exams: "Atelectasis is the collapse or incomplete expansion of lung tissue resulting in areas of poorly aerated or non-aerated pulmonary parenchyma."
SECTION 2: TYPES / CLASSIFICATION
There are 3 main types of atelectasis. This is the most important thing to memorize - examiners love asking this!
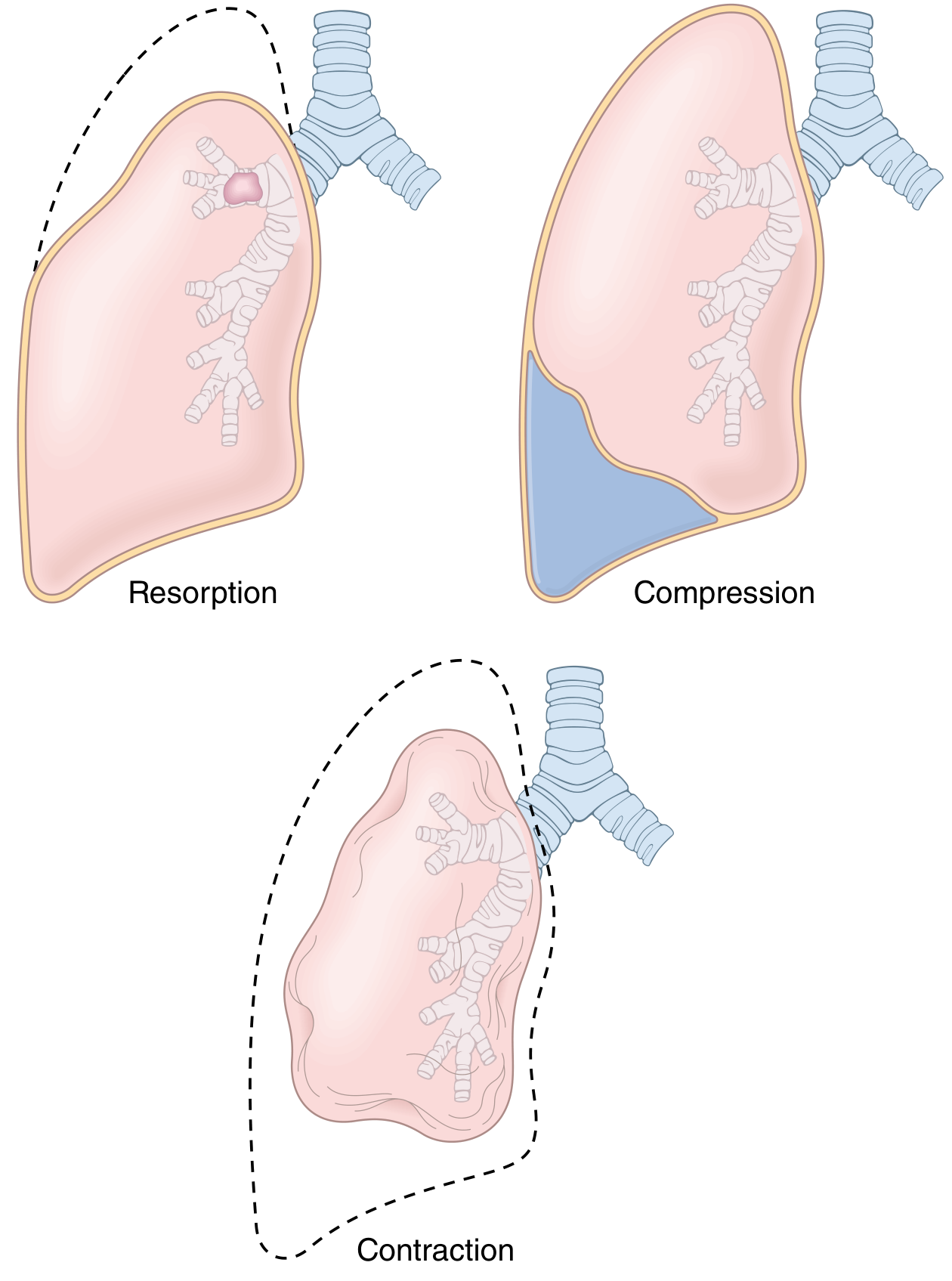
Fig: The three types of acquired atelectasis. Dashed lines indicate normal lung volume - Robbins, Cotran & Kumar Pathologic Basis of Disease
TYPE 1: RESORPTION (OBSTRUCTIVE) ATELECTASIS
The most common type
Mechanism:
- An obstruction BLOCKS air from entering the distal airways
- The air already present DISTAL to the obstruction is gradually resorbed (absorbed) into the blood
- With no new air entering, the alveoli progressively collapse
Key feature on X-ray:
- Mediastinum SHIFTS TOWARD the affected (collapsed) side - because the lung shrinks and pulls structures toward it
Causes:
| Cause | Example |
|---|
| Mucus plugs (most common) | Post-operative patients, asthma, bronchiectasis, chronic bronchitis |
| Foreign body aspiration | Especially in children |
| Intrabronchial tumor | Lung cancer - may be the FIRST sign of malignancy |
| Extrinsic compression of bronchus | Enlarged lymph nodes pressing on airway |
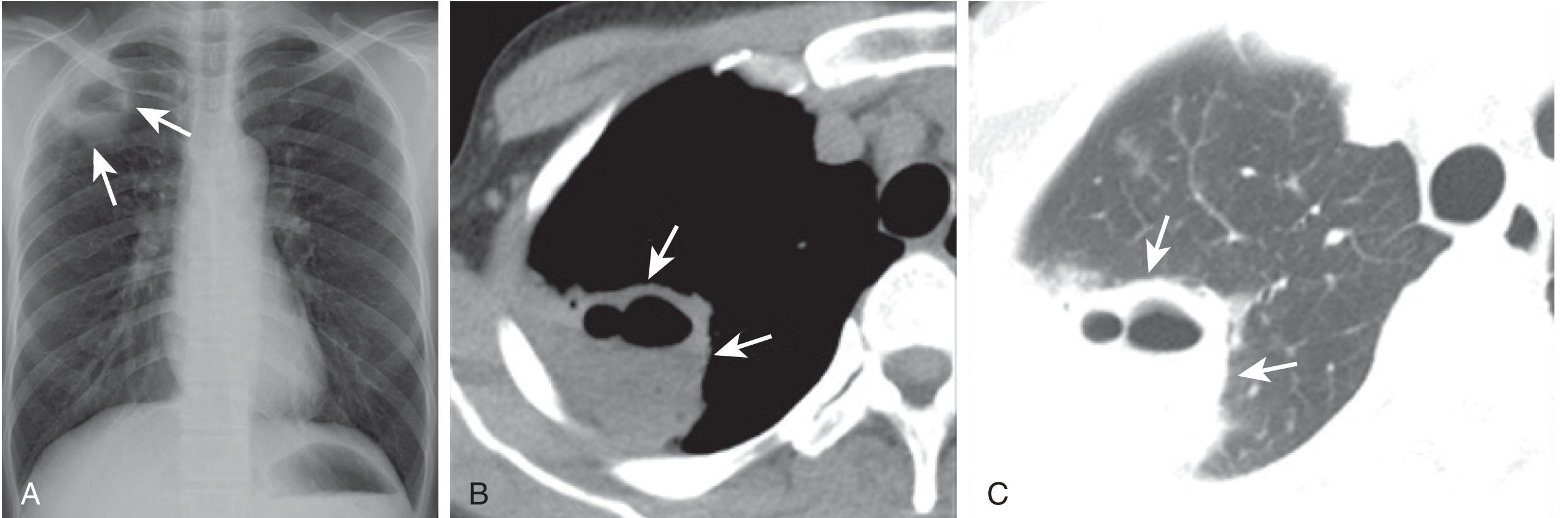
TYPE 2: COMPRESSION (PASSIVE/RELAXATION) ATELECTASIS
Mechanism:
- External pressure is applied on the lung from OUTSIDE, compressing it
- The lung is literally "squashed" and collapses
Key feature on X-ray:
- Mediastinum SHIFTS AWAY from the affected side - because the space-occupying material pushes structures away
Causes:
| Cause | Example |
|---|
| Pleural effusion | Most common - fluid in pleural space (congestive heart failure) |
| Pneumothorax | Air in pleural space |
| Hemothorax | Blood in pleural space |
| Tumors | Large pleural/chest wall tumors |
| Ascites | In bedridden patients - pushes diaphragm up causing basal atelectasis |
Basal atelectasis - a subtype of compression atelectasis. Occurs at lung bases in bedridden patients due to failure to breathe deeply, abdominal pressure pushing up the diaphragm. Very common post-operatively.
TYPE 3: CONTRACTION (CICATRIZATION) ATELECTASIS
Mechanism:
- Fibrosis (scarring) of the lung or pleura prevents the lung from expanding fully
- The lung is "trapped" in a contracted state by scar tissue
- Cicatrization = scarring
Key features:
- This is the ONLY IRREVERSIBLE type of atelectasis
- Seen in late-stage tuberculosis, old healed pneumonia, interstitial fibrosis
Causes:
- Pulmonary fibrosis
- Pleural fibrosis / thickening
- Old tuberculosis with scarring
- Radiation-induced fibrosis
ADDITIONAL TYPES (also asked in exams)
| Type | Description |
|---|
| Plate-like / Discoid / Linear atelectasis | Thin horizontal lines seen on CXR; common in bedridden patients; caused by small areas of underventilation |
| Rounded atelectasis | Ovoid mass-like density touching the pleura; associated with asbestos-related pleural disease; can mimic a lung tumor |
| Microatelectasis | Collapse at the microscopic level; not visible on CXR; seen in ARDS |
| Neonatal atelectasis | Failure of lungs to expand at birth; seen in premature infants (surfactant deficiency - Respiratory Distress Syndrome of newborn) |
SECTION 3: PREDISPOSING / RISK FACTORS
Understanding WHO is at risk helps you write better nursing care plans:
Post-operative Patients (MOST IMPORTANT)
- General anesthesia decreases Functional Residual Capacity (FRC) - the amount of air left in lungs after normal exhalation
- Upper abdominal or thoracic surgery - pain prevents deep breathing; also stimulates GI viscera altering diaphragm function
- Anesthesia impairs mucociliary clearance - the tiny hairs that sweep secretions out of airways stop working
- Patients cannot cough effectively because of pain
Other High-Risk Groups
| Risk Factor | Reason |
|---|
| Immobilized / bedridden patients | Shallow breathing; secretions pool in dependent lung zones |
| Morbid obesity | Abdominal fat pushes diaphragm up; reduces lung volume |
| Smokers | Damaged mucociliary clearance; excess mucus production |
| COPD, asthma, bronchiectasis | Excessive secretions; airway narrowing |
| Neuromuscular diseases | Weak respiratory muscles; cannot breathe deeply |
| Children with foreign body aspiration | Bronchial obstruction |
| Patients with pleural effusion, pneumothorax | Compression of lung |
| Patients with chest pain (rib fractures, pleurisy) | Reluctant to breathe deeply due to pain (splinting) |
SECTION 4: PATHOPHYSIOLOGY
OBSTRUCTION / COMPRESSION / FIBROSIS
↓
Airway blocked OR lung externally compressed OR restricted by fibrosis
↓
Air cannot enter distal alveoli (or existing air gets resorbed)
↓
Alveolar COLLAPSE (atelectasis)
↓
Lung continues to receive blood supply (perfusion) BUT no ventilation
↓
V/Q MISMATCH (blood goes through collapsed areas without getting oxygenated)
↓
HYPOXEMIA (low PaO2 in blood) → Tachypnea, Dyspnea
↓
If prolonged → Mucus stagnates → BACTERIAL INFECTION → PNEUMONIA
Why does V/Q mismatch cause hypoxemia?
- Normal: Every unit of lung that gets blood flow (Q) also gets ventilation (V) → oxygen properly loaded onto haemoglobin
- In atelectasis: Blood still flows through the collapsed lung units but there is NO air → blood passes through without picking up oxygen → "shunt" → hypoxemia
SECTION 5: CLINICAL FEATURES (Signs & Symptoms)
Small Atelectasis (subsegmental / plate-like):
- Often ASYMPTOMATIC - discovered incidentally on X-ray
- May cause mild dyspnea
Larger Atelectasis (lobar / whole lung):
| Symptom/Sign | Description |
|---|
| Dyspnea | Shortness of breath - degree depends on size of collapse |
| Tachypnea | Rapid breathing (respiratory rate >20/min) |
| Tachycardia | Compensatory increase in heart rate |
| Cough | Dry, non-productive initially |
| Hypoxemia | Low SpO2; patient may appear cyanosed (bluish discoloration) |
| Fever (low-grade) | Very important: Atelectasis is the most common cause of fever in the first 24-48 hours post-operatively |
| Chest pain | Especially if associated with pleural irritation |
| Accessory muscle use | In significant respiratory distress |
Physical Examination Findings:
| Examination | Finding |
|---|
| Inspection | Reduced chest expansion on affected side; tracheal deviation TOWARD affected side (resorption type) |
| Palpation | Reduced tactile fremitus on affected side |
| Percussion | DULL note on affected side |
| Auscultation | Absent or decreased breath sounds; may hear bronchial breathing near the collapsed area |
Exam Tip: In post-operative patients, fever in first 24-48 hours = think atelectasis first! (not infection - that comes later, usually after 48-72 hours).
SECTION 6: INVESTIGATIONS
1. Chest X-Ray (First-line investigation)
Signs on CXR:
- Loss of lung volume on affected side
- Displacement of lobar fissures toward the collapse
- Tracheal/mediastinal shift toward the collapsed side (in resorption atelectasis)
- Elevated hemidiaphragm on the affected side
- Crowding of ribs on the affected side
- Plate-like (discoid) atelectasis - thin horizontal lines, usually at bases
- Increased opacity (whiteness) in the area of collapse
2. CT Scan of Chest
- More sensitive than CXR
- Can detect early or subtle atelectasis
- Helps identify the underlying CAUSE (mucus plug, mass, lymph nodes)
- Can distinguish atelectasis from pneumonia, pleural effusion, or tumor
3. Bronchoscopy
- When obstruction is suspected
- Can directly visualize the airway obstruction (tumor, mucus plug, foreign body)
- Can also be THERAPEUTIC - remove the obstruction
4. Arterial Blood Gas (ABG)
- Shows hypoxemia (low PaO2)
- May show hypocapnia (low PaCO2) early due to tachypnea (hyperventilation)
- Later: respiratory failure with hypercapnia if large area involved
5. Pulse Oximetry (SpO2)
- SpO2 ≤96% after breathing oxygen via Venturi mask for 30 minutes is a moderately sensitive test for diagnosing post-operative atelectasis
- Quick bedside monitoring tool - nurses use this continuously
6. Bedside Ultrasound
- Increasingly used to detect atelectasis at bedside in ICU patients
SECTION 7: COMPLICATIONS
| Complication | Explanation |
|---|
| Hypoxemia / Respiratory failure | V/Q mismatch from large areas of collapse |
| Pneumonia | Stagnant secretions in collapsed lung become infected; bacteria multiply |
| Lung abscess | If infection progresses to suppuration |
| Pleural effusion | Secondary to infection/inflammation |
| Permanent lung damage / fibrosis | If untreated for a long time |
| Septicemia | Spread of infection from collapsed infected lung |
SECTION 8: MEDICAL MANAGEMENT
1. Treat the Underlying Cause
- Relieve the obstruction (mucus plug, foreign body, tumor)
- Drain pleural effusion or pneumothorax (compression type)
- Manage underlying fibrosis (contraction type)
2. Incentive Spirometry
- Patient breathes deeply through a spirometer device to expand collapsed alveoli
- Commonly prescribed post-operatively for prevention and treatment
- Patient takes a slow, deep inhalation, sustains it for 5-6 seconds, then exhales
3. Positive Pressure Breathing
- IPPB (Intermittent Positive Pressure Breathing) - delivers positive pressure during inhalation
- CPAP (Continuous Positive Airway Pressure) / BiPAP (Non-invasive ventilation) - keeps alveoli open by maintaining positive end-expiratory pressure; very effective for post-operative atelectasis
- PEEP (Positive End-Expiratory Pressure) - in mechanically ventilated patients
4. Bronchoscopy
- For obstructive atelectasis
- Suction out mucus plugs
- Remove foreign bodies
- Biopsy tumors
5. Pharmacological Treatment
- Bronchodilators (nebulized Salbutamol, Ipratropium) - dilate airways, facilitate mucus clearance
- Mucolytics (N-Acetylcysteine) - thin out thick secretions
- Antibiotics - if secondary infection / pneumonia develops
- Analgesics - for post-operative patients so pain does not prevent deep breathing
6. Positioning
- Semi-Fowler's (30-45°) or High Fowler's (90°) - reduces compression of lung bases by abdominal organs
- Frequent repositioning every 2 hours - changes dependent areas, redistributes ventilation
7. Oxygen Therapy
- Supplemental oxygen to correct hypoxemia
- Monitor SpO2 continuously
SECTION 9: NURSING MANAGEMENT
Nursing Assessment
- Monitor vital signs - temperature (especially post-op fever), respiratory rate, SpO2, pulse
- Observe breathing pattern - depth, rate, use of accessory muscles
- Auscultate breath sounds - note any absent/decreased areas
- Assess cough effectiveness - can the patient cough and raise secretions?
- Assess pain level - especially post-operative incisional pain that prevents deep breathing
- Monitor ABG results and SpO2
- Assess level of consciousness and mobility
Nursing Diagnoses (NANDA)
- Ineffective Breathing Pattern related to pain, anesthesia, or airway obstruction, manifested by shallow respirations and decreased SpO2
- Impaired Gas Exchange related to V/Q mismatch secondary to collapsed alveoli, manifested by hypoxemia and dyspnea
- Ineffective Airway Clearance related to retained secretions, manifested by inability to cough effectively
- Acute Pain related to surgical incision (post-op patients), manifested by reluctance to breathe deeply (splinting)
- Risk for Infection related to stagnant secretions in collapsed lung
- Anxiety related to dyspnea and hypoxemia
Nursing Interventions
1. AIRWAY CLEARANCE
- Deep breathing exercises - instruct patient to take 5 slow deep breaths, hold for 5-6 seconds, then exhale fully; repeat every 1-2 hours
- Coughing exercises - "Huff coughing" (2-3 short huffs followed by a strong cough) is less painful and more effective than hard coughing
- Splinting technique - teach post-op patients to hold a pillow firmly against the incision while coughing to reduce pain and allow more effective cough
- Incentive spirometry - demonstrate correct use; encourage patient to use every 1-2 hours while awake
- Chest physiotherapy (CPT) - percussion (clapping) and vibration over affected areas to loosen secretions
- Postural drainage - position the affected lung upward/elevated so gravity assists drainage of secretions
- Suction - nasotracheal or tracheal suction if patient cannot clear secretions independently
2. PROMOTING VENTILATION
- Positioning: Elevate head of bed to High Fowler's or Semi-Fowler's position (30-90°) to allow maximum lung expansion
- Ambulation / Early mobilization - encourage early walking post-operatively (within 24 hours if possible)
- Turn and reposition every 2 hours in immobilized patients
- Oxygen therapy as prescribed - monitor SpO2, keep ≥95%
- Assist with CPAP/BiPAP if prescribed
3. PAIN MANAGEMENT (critical in post-op patients)
- Administer prescribed analgesics (paracetamol, NSAIDs, opioids as needed)
- Coordinate deep breathing and coughing exercises to happen after analgesic administration (when pain is controlled)
- Teach splinting technique
- Regional blocks (epidural) may be used by the anaesthesia team
4. HYDRATION
- Encourage oral fluid intake (2-3 litres/day if no contraindication)
- Adequate hydration thins secretions, making them easier to cough up
- Administer IV fluids as ordered
5. MONITORING AND RECORDING
- Monitor SpO2 continuously
- Monitor respiratory rate, depth, and effort every 2-4 hours
- Auscultate breath sounds at least every shift
- Monitor temperature for post-operative fever
- Document any changes in sputum colour, amount, consistency
- Report: SpO2 <94%, RR >25, worsening dyspnea, increasing fever - to the physician immediately
6. PREVENTION OF ATELECTASIS (Pre-operative and Post-operative Nursing)
| Timing | Nursing Action |
|---|
| Pre-operative | Teach deep breathing and coughing exercises BEFORE surgery; smoking cessation; incentive spirometry teaching |
| Post-operative | Early ambulation; pain management; deep breathing exercises every 1-2 hours; incentive spirometry; frequent repositioning |
| Ongoing | Monitor all immobilized patients; never leave a patient flat in bed for prolonged periods |
7. PATIENT AND FAMILY EDUCATION
- Explain what atelectasis is and why it happens (especially to post-op patients/families)
- Demonstrate incentive spirometry use before surgery; observe return demonstration
- Teach deep breathing and huff coughing technique
- Explain importance of early ambulation after surgery
- Tell patient to report any worsening breathlessness, chest pain, or fever
- Explain the purpose of all devices (O2 mask, spirometer, suction)
SECTION 10: PREVENTION
Prevention is very important for nursing practice - this is often asked as a short note:
- Pre-operative breathing exercises - teach before surgery
- Incentive spirometry - before and after surgery
- Early ambulation post-operatively
- Adequate pain control - so patients can breathe deeply
- Deep breathing and coughing exercises every 1-2 hours post-op
- Frequent repositioning - every 2 hours for all immobilized patients
- Adequate hydration - to prevent thick, sticky secretions
- Smoking cessation - before elective surgery
- Avoidance of prolonged supine position
- Proper management of pleural effusions and pneumothorax
PREVIOUS YEAR-STYLE QUESTIONS WITH ANSWERS
LONG ANSWER QUESTIONS (10-15 marks)
Q1. Define atelectasis. Describe its types, causes, clinical features, and nursing management.
Answer Structure:
- Definition (see Section 1)
- Types with diagram: Resorption, Compression, Contraction (see Section 2)
- Causes for each type (see Section 3)
- Clinical features (see Section 5)
- Nursing Management in detail (see Section 9)
Q2. Discuss the nursing management of a post-operative patient with atelectasis.
Key Points to Cover:
- Why post-op patients are at risk (anesthesia, pain, reduced FRC)
- Assessment (SpO2, breath sounds, temperature, pain level)
- Nursing diagnoses
- Interventions: deep breathing, incentive spirometry, pain management, early ambulation, positioning, splinting technique, chest physiotherapy
- Patient education
- Monitoring and reporting criteria
SHORT ANSWER QUESTIONS (5 marks)
Q1. What is resorption atelectasis? Give two causes.
- Obstruction of airway → air distal to obstruction gets absorbed → alveolar collapse
- Mediastinum shifts TOWARD affected side
- Causes: mucus plugs (most common), foreign body aspiration
Q2. What is incentive spirometry? What is its role in atelectasis?
- Device that provides visual feedback during slow, deep inhalation
- Patient inhales slowly, ball/float rises to target, hold for 5-6 sec
- Expands collapsed alveoli by creating negative intrathoracic pressure
- Used every 1-2 hours post-operatively for prevention and treatment
Q3. Differentiate between resorption and compression atelectasis.
| Feature | Resorption | Compression |
|---|
| Cause | Airway obstruction | External pressure (fluid/air in pleural space) |
| Mechanism | Air resorbed from distal alveoli | Lung physically compressed |
| Mediastinal shift | TOWARD affected side | AWAY from affected side |
| Reversibility | Reversible | Reversible |
| Example | Mucus plug post-op | Pleural effusion, pneumothorax |
Q4. Atelectasis is the most common cause of post-operative fever. Explain.
- General anesthesia reduces FRC
- Mucociliary clearance is impaired
- Inadequate deep breathing due to pain causes secretion retention
- Secretions pool in dependent lung zones → alveoli collapse (atelectasis)
- Collapsed lung with stagnant secretions triggers an inflammatory response → fever
- This typically occurs in the first 24-48 hours post-operatively
- Treatment: deep breathing exercises, early ambulation, incentive spirometry - NOT antibiotics (no infection yet)
MCQs ON ATELECTASIS (15 Questions)
1. Atelectasis is BEST defined as:
- A) Inflammation of the lung parenchyma
- B) Loss of lung volume due to inadequate expansion of air spaces ✅
- C) Accumulation of fluid in the pleural space
- D) Overinflation of air spaces
2. The MOST common type of atelectasis encountered in post-operative patients is:
- A) Compression atelectasis
- B) Contraction atelectasis
- C) Resorption (obstructive) atelectasis ✅
- D) Rounded atelectasis
3. In resorption atelectasis, the mediastinum shifts:
- A) Away from the affected side
- B) Toward the affected side ✅
- C) Does not shift
- D) Shifts downward only
4. A 45-year-old patient develops a fever of 38.2°C on the first post-operative day after abdominal surgery. The MOST likely cause is:
- A) Wound infection
- B) Urinary tract infection
- C) Atelectasis ✅
- D) Deep vein thrombosis
5. Which type of atelectasis is IRREVERSIBLE?
- A) Resorption atelectasis
- B) Compression atelectasis
- C) Contraction atelectasis ✅
- D) Plate-like atelectasis
6. Incentive spirometry works by:
- A) Applying positive pressure during exhalation
- B) Encouraging slow, deep inhalation to expand alveoli ✅
- C) Vibrating the chest wall to loosen secretions
- D) Delivering nebulized bronchodilators
7. The MOST important nursing intervention to prevent atelectasis in a post-operative patient is:
- A) Administering antibiotics prophylactically
- B) Keeping patient in supine position for 24 hours
- C) Deep breathing exercises and early ambulation ✅
- D) Restricting oral fluids to prevent secretions
8. In compression atelectasis caused by pleural effusion, the mediastinum shifts:
- A) Toward the affected side
- B) Away from the affected side ✅
- C) Does not shift
- D) Superiorly
9. A patient with atelectasis will show which finding on PERCUSSION of the affected area?
- A) Hyperresonance
- B) Tympany
- C) Dullness ✅
- D) Normal resonance
10. Which of the following is the HALLMARK of V/Q mismatch in atelectasis?
- A) Hypercapnia
- B) Hypoxemia ✅
- C) Metabolic acidosis
- D) Hyperglycemia
11. "Splinting" in post-operative nursing refers to:
- A) Applying a brace to the surgical site
- B) Holding a pillow against incision while coughing to reduce pain ✅
- C) Tying the patient's legs together post-operatively
- D) Applying external pressure to reduce lung expansion
12. Rounded atelectasis is characteristically associated with:
- A) Tuberculosis
- B) Foreign body aspiration
- C) Asbestos-related pleural disease ✅
- D) Right heart failure
13. Which gas is primarily resorbed in resorption atelectasis causing alveolar collapse?
- A) Oxygen ✅ (along with other gases already present distal to obstruction)
- B) Carbon dioxide only
- C) Nitrogen only
- D) Helium
14. On chest X-ray, plate-like (discoid) atelectasis appears as:
- A) Round opacity near the pleura
- B) Thin horizontal lines, usually at lung bases ✅
- C) Homogeneous opacity of an entire lobe
- D) Cavitary lesion with air-fluid level
15. The CORRECT position for a patient with atelectasis to maximize lung expansion is:
- A) Supine (flat)
- B) Trendelenburg (head down)
- C) High Fowler's or Semi-Fowler's ✅
- D) Left lateral decubitus
QUICK REVISION TABLE
| Feature | Key Point |
|---|
| Definition | Collapse / incomplete expansion of lung tissue |
| Types | Resorption, Compression, Contraction |
| Most common type | Resorption (obstruction) |
| Most common cause | Mucus plug post-operatively |
| Only irreversible type | Contraction (cicatrization) atelectasis |
| Mediastinum in resorption | Shifts TOWARD affected side |
| Mediastinum in compression | Shifts AWAY from affected side |
| V/Q mismatch causes | Hypoxemia |
| Most common post-op complication | Atelectasis |
| Most common cause of post-op fever (day 1-2) | Atelectasis ("Wind" - remember Wind, Water, Wound, Walking, Wonder drugs - 5 Ws of post-op fever) |
| Key nursing intervention | Deep breathing, incentive spirometry, early ambulation |
| Key investigation | CXR (shows loss of volume + fissure/mediastinal displacement) |
| Irreversible type | Contraction atelectasis |
| Percussion note | Dull |
| Breath sounds | Decreased / absent |
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E; Sabiston Textbook of Surgery
Would you like me to now generate a downloadable PDF of these notes, or shall we move on to the next respiratory topic? 📚