Complications of glaucoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"glaucoma" AND "complications"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Complications of Glaucoma
Glaucoma is an optic neuropathy in which progressive damage to retinal ganglion cells and their axons results in loss of optic nerve tissue and damage to visual fields. Its complications can be divided into those arising from the disease itself and those arising from its treatment (medical and surgical).
I. Complications of the Disease Itself
1. Optic Nerve Damage and Cupping
The primary site of injury is the lamina cribrosa, where the axons of the optic nerve leave the eye. Rising IOP - or vascular insufficiency at normal IOP - destroys retinal ganglion cells and their axons. The key features are:
- Diffuse loss of ganglion cells with thinning of the retinal nerve fiber layer (RNFL)
- Optic disc cupping: enlargement of the cup-to-disc ratio (a ratio >0.6 is abnormal; asymmetry of >0.2 between the two eyes is suspicious)
- In advanced cases the optic nerve is both cupped and atrophic
- Peripapillary atrophy (PPA): the beta (inner) zone of chorioretinal atrophy around the disc is larger and more common in glaucoma, and its location predicts the orientation of visual field loss
- Disc haemorrhage: splinter/flame haemorrhages at the disc margin are an important risk factor for progression and can precede RNFL defects
(Kanski's Clinical Ophthalmology 10th ed.; Goldman-Cecil Medicine)
2. Retinal Nerve Fibre Layer (RNFL) Defects
Subtle RNFL defects precede detectable optic disc and visual field changes. Two patterns occur:
- Localized wedge-shaped defects - more specific to glaucoma
- Diffuse RNFL loss - larger, with indistinct borders
The arcuate fibres reaching the superotemporal and inferotemporal optic nerve head are most vulnerable; fibres in the papillomacular bundle are the most resistant.
(Kanski's Clinical Ophthalmology 10th ed.)
3. Visual Field Loss
Visual field loss is the hallmark functional complication. It is typically:
- Peripheral vision lost first - central vision is relatively preserved until late
- Arcuate (Bjerrum) scotoma: arises from damage to arcuate nerve fibres; appears as a curved defect above or below fixation
- Nasal step: a step in the nasal visual field respecting the horizontal meridian
- Paracentral scotoma
- Altitudinal defects in advanced disease
- In end-stage disease: tunnel vision, then complete blindness
The damage to vision caused by glaucoma is irreversible. (Textbook of Family Medicine 9e; Adams & Victor's Principles of Neurology)
4. Blindness
Glaucoma is responsible for at least 10% of cases of blindness in the United States. It is the leading cause of irreversible blindness worldwide. The risk of blindness is substantially higher in:
- African Americans (8x more likely than Caucasians to develop glaucoma-related blindness)
- Patients with uncontrolled IOP
- Those with advanced disease at first presentation
Because glaucoma is asymptomatic until late in its course, the "silent thief of sight" nature makes late presentation common. (Textbook of Family Medicine 9e; Goldman-Cecil Medicine)
5. Corneal Complications
In acute angle-closure glaucoma, a sudden severe rise in IOP causes:
- Corneal oedema (epithelial and stromal) - presenting as blurring and halos around lights
- Corneal decompensation (bullous keratopathy) in chronic or repeated attacks
- Corneal clouding makes fundal examination difficult
In congenital glaucoma, elevated IOP causes:
- Buphthalmos (enlargement of the entire globe - "ox eye") due to scleral stretching in the first years of life
- Haab's striae: horizontal breaks in Descemet's membrane from stretching
6. Lens Complications
- Cataract: a complication of chronic IOP elevation, glaucomatocyclitic crises, or prolonged miotic therapy (cholinergic agents)
- Lens subluxation/dislocation can occur in secondary glaucoma associated with pseudoexfoliation syndrome or Marfan syndrome
- Glaukomflecken: anterior subcapsular lens opacities that are pathognomonic of a prior acute angle-closure attack
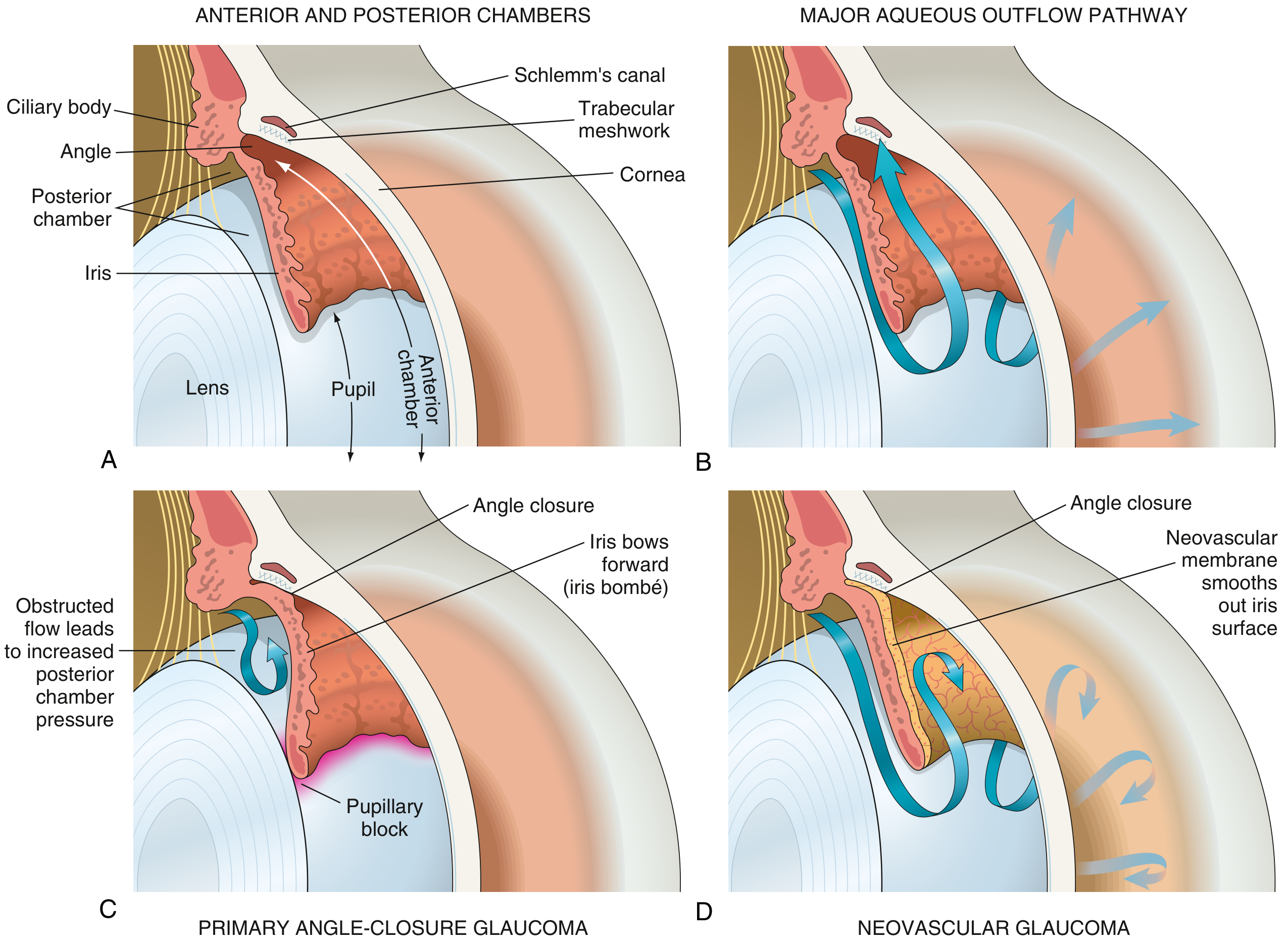
7. Neovascular Glaucoma (NVG)
Retinal ischaemia (from diabetic retinopathy, central retinal vein occlusion, or ocular ischaemic syndrome) triggers release of VEGF, leading to:
- Rubeosis iridis: abnormal new vessels growing over the iris surface
- A neovascular membrane contracts and forms peripheral anterior synechiae (PAS), closing the angle
- Severe, often intractable IOP elevation
- This represents both a complication of the underlying retinal vascular disease AND a secondary form of glaucoma itself
(Robbins & Kumar Basic Pathology)
8. Subacute and Chronic Angle-Closure Complications
- Peripheral anterior synechiae (PAS): adhesions between peripheral iris and trabecular meshwork/cornea, permanently closing the angle
- Posterior synechiae: adhesions between the iris and lens, leading to iris bombé and secondary angle closure
- Pupillary block: aqueous cannot flow from the posterior to the anterior chamber
II. Complications of Glaucoma Treatment
A. Medical Treatment Complications
| Drug Class | Notable Complications |
|---|---|
| Beta-blockers (timolol) | Bradycardia, bronchospasm, exacerbation of COPD/asthma, depression, impotence |
| Prostaglandin analogues (latanoprost) | Iris hyperpigmentation (irreversible), eyelash growth, periorbital fat atrophy, anterior uveitis |
| Alpha-2 agonists (brimonidine) | Allergic conjunctivitis, CNS depression in children, fatigue |
| Carbonic anhydrase inhibitors (dorzolamide topical; acetazolamide oral) | Metallic taste, urolithiasis, aplastic anaemia (acetazolamide), paraesthesias |
| Miotics (pilocarpine) | Induced myopia, brow ache, cataract with long-term use, retinal detachment (rare) |
| Steroids (as a cause of secondary glaucoma) | Steroid-induced open-angle glaucoma; reversible after discontinuation, but visual loss during the period may be permanent |
(Goodman & Gilman's Pharmacological Basis of Therapeutics; Textbook of Family Medicine 9e)
B. Laser Treatment Complications
- Laser trabeculoplasty (SLT/ALT): Transient IOP spike in the first hours post-procedure; uveitis; corneal endothelial damage
- Laser iridotomy: Lens damage, corneal burns, transient IOP spike, monocular diplopia, dysphotopsia
C. Postoperative Complications of Glaucoma Surgery (Trabeculectomy / Tube-Shunt)
These are systematically classified by the Wills Eye Manual and summarized below:
| Complication | IOP | Anterior Chamber | Key Feature |
|---|---|---|---|
| Inflammation / Fibrin | Variable / Low | Deep | Post-op inflammatory response |
| Hyphema | Mildly elevated | Variable | Blood in AC |
| Failure to filter | Elevated | Deep | Flat/failed bleb |
| Aqueous misdirection (Malignant glaucoma) | Elevated | Diffusely shallow (Grade 2-3) | No iris bombé; bleb flat |
| Suprachoroidal haemorrhage | Markedly elevated initially | Grade 1-2 | Excruciating pain |
| Pupillary block | Moderately to markedly elevated | Grade 1-3 | Iris bombé present |
| Serous choroidal detachment | Low | Variable | "Kissing choroidals" |
| Wound leak | Low | Shallow | Positive Seidel test |
| Overfiltration / Hypotony | <7-8 mmHg | Shallow | Maculopathy, choroidal folds |
(Wills Eye Manual 9.18)
Low postoperative IOP (<4 mmHg) is associated with:
- Hypotony maculopathy (choroidal folds leading to visual distortion/loss)
- Flat anterior chamber
- Corneal oedema
- Suprachoroidal haemorrhage
Bleb-related complications:
- Blebitis (superficial bleb infection) - can progress to endophthalmitis
- Endophthalmitis - most serious complication; can cause permanent severe visual loss
- Bleb dysaesthesia - discomfort from overhanging or thin-walled blebs
- Conjunctival bleb failure and encapsulated (Tenon's) cysts
(Wills Eye Manual, Kanski's Clinical Ophthalmology 10th ed.)
III. Complications in Special Forms of Glaucoma
Congenital / Infantile Glaucoma
- Buphthalmos (globe enlargement)
- Haab's striae (corneal tears)
- Corneal opacification
- Amblyopia - a major risk due to corneal clouding and induced high astigmatism
- Nystagmus in aniridia-associated glaucoma
Neurofibromatosis Type 1
- Glaucoma (usually unilateral) associated with ipsilateral plexiform neurofibroma; mechanisms include angle anomaly and ectropion uveae
Sturge-Weber Syndrome
- Glaucoma in ~30% of patients; surgical correction carries relatively high risk of choroidal effusion and suprachoroidal haemorrhage due to raised episcleral venous pressure
(Kanski's Clinical Ophthalmology 10th ed.)
Summary
| Category | Key Complications |
|---|---|
| Optic nerve | Cupping, atrophy, RNFL loss, disc haemorrhage |
| Visual field | Arcuate scotoma, nasal step, tunnel vision, blindness |
| Cornea | Oedema, bullous keratopathy, Haab's striae (congenital), buphthalmos |
| Lens | Cataract, glaukomflecken, subluxation |
| Angle | PAS, posterior synechiae, iris bombé, NVG |
| Surgical | Hypotony maculopathy, bleb infection, endophthalmitis, suprachoroidal haemorrhage, malignant glaucoma |
| Medical therapy | Systemic effects of anti-glaucoma drugs, steroid-induced glaucoma |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (comprehensive optic nerve and RNFL changes, special glaucomas)
- Robbins & Kumar Basic Pathology (pathophysiology, neovascular glaucoma)
- The Wills Eye Manual (postoperative complications table)
- Goldman-Cecil Medicine (clinical course and blindness risk)
- Textbook of Family Medicine, 9e (steroid glaucoma, epidemiology)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (drug complications)
- Adams & Victor's Principles of Neurology (visual field defects)
Point wise complications
Here is a concise point-wise summary of all complications of glaucoma:
Complications of Glaucoma
A. Ocular Complications of the Disease
Optic Nerve
- Progressive optic disc cupping (increased cup-to-disc ratio)
- Optic nerve atrophy
- Retinal nerve fibre layer (RNFL) thinning - wedge-shaped or diffuse defects
- Peripapillary atrophy (beta zone)
- Disc haemorrhages (splinter/flame - marker of progression)
Visual Field
- Paracentral scotoma (earliest)
- Arcuate (Bjerrum) scotoma - above or below fixation
- Nasal step (respects horizontal meridian)
- Altitudinal defects
- Tunnel vision (end-stage)
- Total blindness (irreversible)
Cornea
- Corneal oedema (in acute angle-closure)
- Bullous keratopathy (chronic corneal decompensation)
- Haab's striae - horizontal Descemet tears (congenital glaucoma)
- Corneal clouding / opacification
Lens
- Cataract (from chronic IOP elevation or miotic therapy)
- Glaukomflecken - anterior subcapsular opacities (pathognomonic of previous acute attack)
- Lens subluxation / dislocation (in pseudoexfoliation or Marfan-associated glaucoma)
Angle & Uvea
- Peripheral anterior synechiae (PAS) - permanent angle closure
- Posterior synechiae - iris to lens adhesion
- Iris bombé - from pupillary block
- Rubeosis iridis (neovascularisation of iris)
- Neovascular glaucoma (secondary to retinal ischaemia)
Globe
- Buphthalmos ("ox eye") - globe enlargement in congenital/infantile glaucoma
- Amblyopia - due to corneal clouding or anisometropia (congenital glaucoma)
B. Complications of Medical Treatment
- Beta-blockers (timolol): Bradycardia, bronchospasm, depression, impotence
- Prostaglandin analogues (latanoprost): Iris hyperpigmentation (irreversible), eyelash lengthening, periorbital fat atrophy, uveitis
- Alpha-2 agonists (brimonidine): Allergic follicular conjunctivitis, CNS depression in infants
- Topical carbonic anhydrase inhibitors (dorzolamide): Stinging, corneal oedema
- Oral acetazolamide: Paraesthesias, urolithiasis, electrolyte disturbances, aplastic anaemia
- Miotics (pilocarpine): Induced myopia, brow ache, cataract (long-term), retinal detachment (rare)
- Steroids (cause of secondary glaucoma): Steroid-induced open-angle glaucoma; any visual loss during IOP elevation is permanent
C. Complications of Laser Treatment
- Transient IOP spike (post-laser trabeculoplasty or iridotomy)
- Anterior uveitis
- Corneal endothelial burns
- Lens damage (iridotomy)
- Monocular diplopia / dysphotopsia (patent iridotomy)
D. Postoperative Complications of Glaucoma Surgery
Early
- Hyphema (blood in anterior chamber)
- Wound leak (shallow AC, low IOP, positive Seidel test)
- Overfiltration / hypotony (IOP <7 mmHg)
- Flat anterior chamber
- Choroidal detachment (serous)
- Suprachoroidal haemorrhage (sudden severe pain, markedly elevated IOP)
- Pupillary block (iris bombé, elevated IOP)
- Aqueous misdirection / malignant glaucoma (diffusely shallow AC, elevated IOP, flat bleb)
Late
- Bleb failure / encapsulated (Tenon's) cyst
- Blebitis (superficial bleb infection)
- Endophthalmitis (most serious - can cause permanent severe visual loss)
- Bleb dysaesthesia (chronic discomfort)
- Hypotony maculopathy (choroidal folds, visual distortion)
- Cataract progression (following trabeculectomy)
- Tube erosion / exposure (tube-shunt surgery)
- Corneal decompensation (tube-cornea touch)
E. Systemic / Epidemiological Consequence
- Responsible for ≥10% of all blindness in the United States
- Leading cause of irreversible blindness worldwide
- Vision loss is permanent - no recovery once ganglion cells are lost
Bsc nursing students complications of glaucoma
Here is a BSc Nursing-level, easy-to-understand, point-wise coverage of complications of glaucoma — organized the way it would appear in a nursing exam or clinical posting.
Complications of Glaucoma
(For BSc Nursing Students)
First, Understand Why Complications Occur
Glaucoma = Raised intraocular pressure (IOP) → damages optic nerve → visual loss If not detected early or not treated properly, complications develop.
COMPLICATIONS
1. 👁️ Visual Field Loss (Most Important)
- First sign: Loss of peripheral (side) vision
- Patient does not notice it early — glaucoma is called "Silent thief of sight"
- Progresses to tunnel vision (only central vision remains)
- Finally leads to complete blindness
- Visual loss in glaucoma is IRREVERSIBLE ← Exam point
2. Optic Nerve Damage
- Raised IOP compresses the optic nerve at the lamina cribrosa
- Leads to optic disc cupping (cup-to-disc ratio increases >0.6)
- Followed by optic atrophy (nerve fibres die permanently)
- Seen on fundus examination as a pale, cupped disc
3. Corneal Complications
| Complication | When it occurs |
|---|---|
| Corneal oedema | Acute angle-closure attack |
| Bullous keratopathy | Chronic/repeated attacks |
| Haab's striae | Congenital glaucoma (horizontal cracks in Descemet's membrane) |
| Buphthalmos | Congenital glaucoma - entire globe enlarges ("ox eye") |
4. Cataract
- Raised IOP reduces nutrition to the lens → lens opacity (cataract)
- Also caused by long-term use of miotic eye drops (e.g., pilocarpine)
- Glaukomflecken = small white dots on the front of the lens seen after an acute attack of angle-closure glaucoma ← Exam point
5. Amblyopia (Lazy Eye)
- Occurs in children with congenital glaucoma
- Corneal clouding or high astigmatism prevents clear image formation
- Brain suppresses the blurred image → permanent visual impairment develops if not treated early
6. Neovascular Glaucoma
- Prolonged high IOP or retinal ischaemia → new abnormal blood vessels grow on iris (rubeosis iridis)
- These vessels block drainage angle → worsens glaucoma further
- Very difficult to treat; often leads to blindness
7. Corneal Blindness / Decompensation
- Chronic high IOP → corneal endothelium fails
- Cornea becomes permanently cloudy
- May require corneal transplant
8. Subluxation of Lens
- Seen in secondary glaucoma (e.g., pseudoexfoliation syndrome, Marfan syndrome)
- Weakened zonules → lens shifts out of position
- Causes sudden worsening of vision
9. Complications of Drug Treatment (Nursing Responsibility)
Nurses must monitor for side effects of anti-glaucoma medications:
| Drug | Side Effects to Watch |
|---|---|
| Timolol (beta-blocker drops) | Bradycardia, low BP, bronchospasm — avoid in asthma/COPD |
| Pilocarpine (miotic drops) | Headache (brow ache), blurred vision (miosis), sweating |
| Latanoprost (prostaglandin) | Iris colour change (permanent darkening), eyelash growth |
| Brimonidine | Allergy, dry mouth, drowsiness — dangerous in infants |
| Acetazolamide (oral tablet) | Tingling in fingers/toes, kidney stones, low potassium, rarely blood dyscrasia |
10. Complications of Surgery (Trabeculectomy)
| Complication | Simple Explanation |
|---|---|
| Hyphema | Bleeding inside the eye (blood in anterior chamber) |
| Flat anterior chamber | Space between cornea and iris collapses |
| Wound leak | Fluid leaking through surgical wound |
| Choroidal detachment | Fluid collects behind the choroid layer |
| Suprachoroidal haemorrhage | Sudden severe bleeding → severe pain, sudden blindness risk |
| Malignant glaucoma | Aqueous goes in wrong direction → very shallow AC, high IOP |
| Blebitis / Endophthalmitis | Infection of the filtration bleb → can cause permanent blindness |
| Hypotony maculopathy | IOP too low → retina folds, blurred/distorted vision |
| Cataract | Lens becomes cloudy after surgery |
11. Blindness (End-Stage Complication)
- Leading cause of irreversible blindness worldwide
- Responsible for ≥10% of all blindness in the USA
- African Americans are 8 times more likely to go blind from glaucoma
- Prevention through early detection and regular IOP monitoring is key
Nursing Key Points to Remember
| Point | Detail |
|---|---|
| Earliest visual field defect | Paracentral scotoma → arcuate scotoma → nasal step |
| Pathognomonic of past acute attack | Glaukomflecken on lens |
| Congenital glaucoma sign | Buphthalmos + Haab's striae |
| Most dangerous surgical complication | Endophthalmitis |
| Most common cause of irreversible blindness | Glaucoma |
| Drug to avoid in asthma | Timolol (beta-blocker) eye drops |
| Visual loss is | Irreversible — stress early detection |
Nursing Role in Preventing Complications
- Teach patients to use eye drops correctly and regularly
- Monitor IOP at every visit
- Educate about signs of acute attack — red eye, severe headache, blurred vision, nausea/vomiting
- Advise regular ophthalmology follow-up
- Screen high-risk groups — elderly, diabetics, family history, African Americans
- Post-surgical care — watch for pain, redness, discharge, sudden vision change
- Emotional support — fear of blindness causes anxiety; counselling is important
Exam Tip: In BSc Nursing exams, complications are commonly asked as: "List the complications of glaucoma" or "Nursing management of a patient with glaucoma" Always mention irreversible blindness as the end-stage complication and early detection as the key preventive measure.
This is a shared conversation. Sign in to Orris to start your own chat.