Abdominal pain various site with causes
Reading File
Finding Sources
Finding Sources
Searching the Web
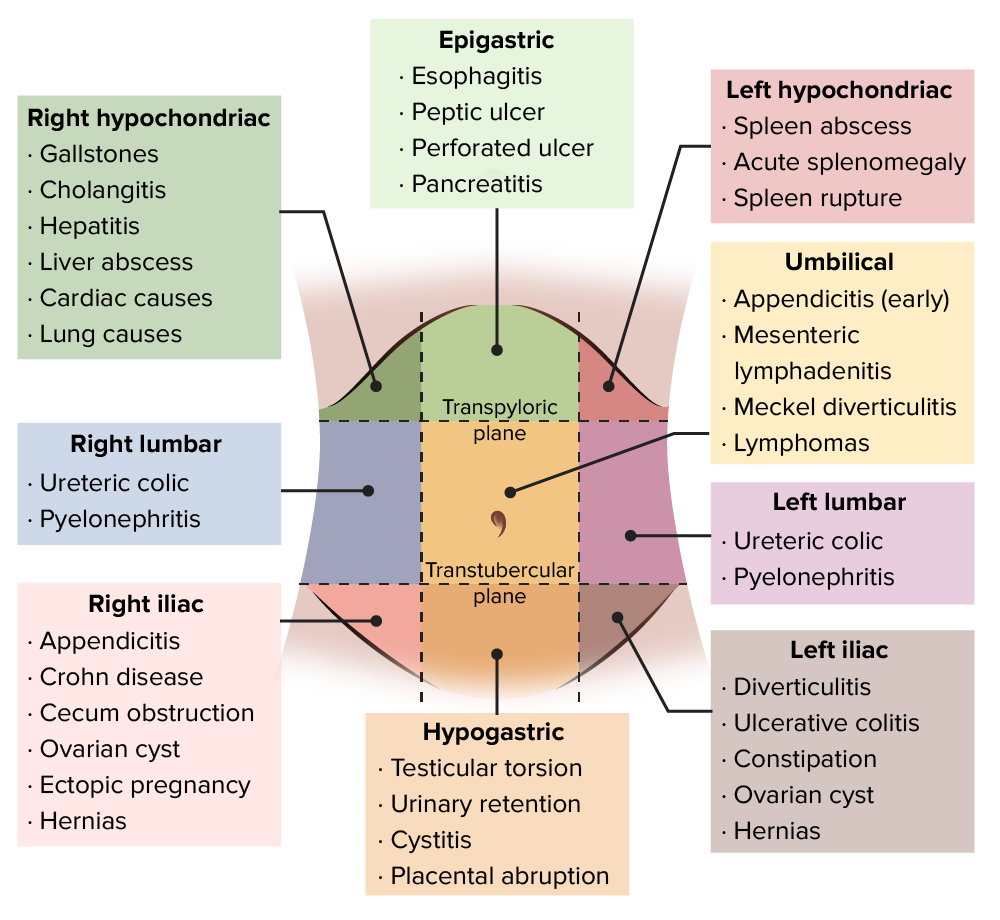
abdominal pain location site causes differential diagnosis diagram
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have rich textbook content and two excellent diagrams. Let me compile a comprehensive, well-organized answer.
Abdominal Pain by Site and Causes
Here is a complete breakdown of abdominal pain organized by anatomical location, drawn from authoritative medical textbooks (Tintinalli's Emergency Medicine, Sleisenger & Fordtran's GI Disease, Goldman-Cecil Medicine, Yamada's Gastroenterology).
Visual Reference Diagrams
The 9-region diagram (Lecturio):
The Tintinalli's Emergency Medicine quadrant diagram:
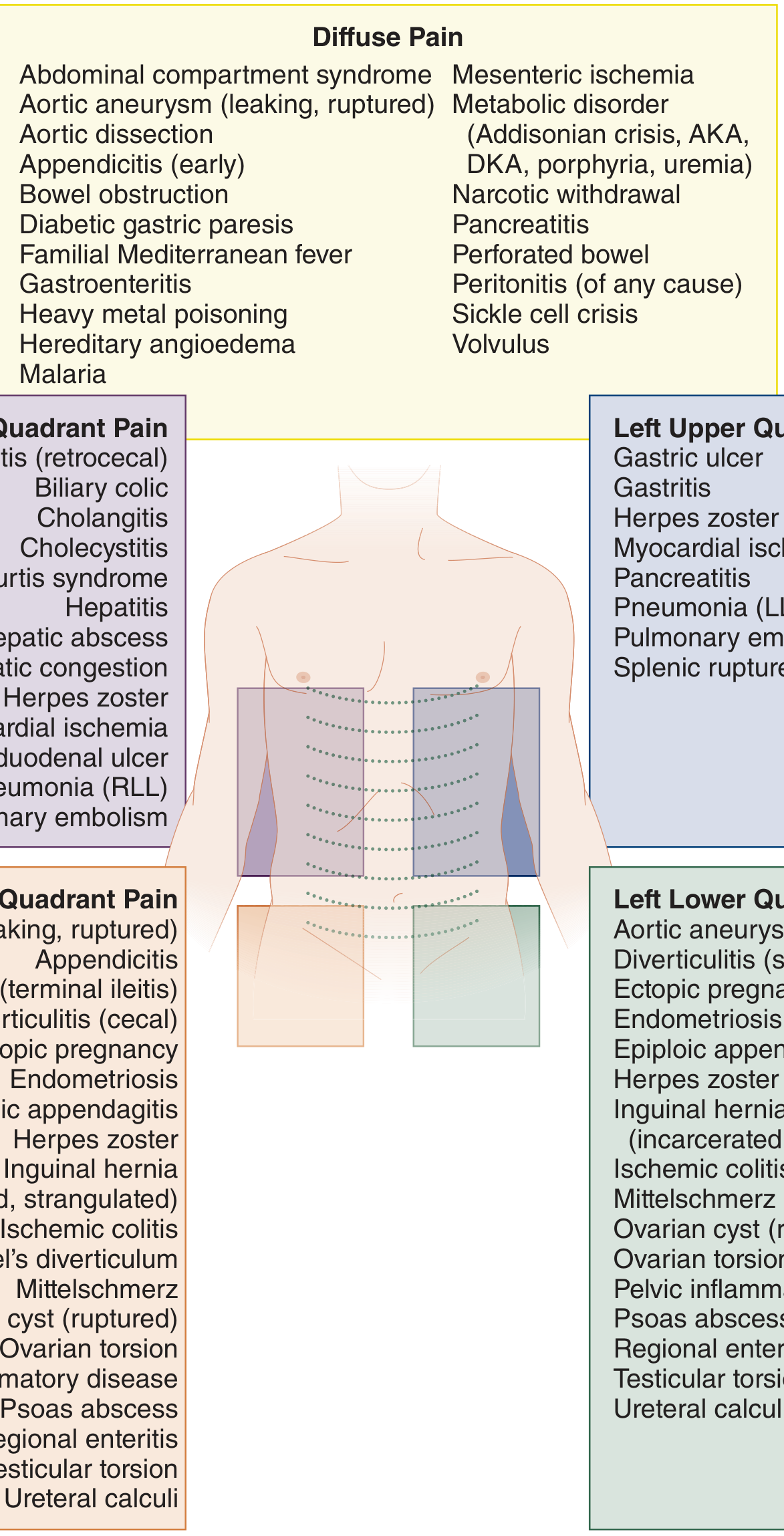
Diffuse / Generalized Abdominal Pain
These conditions tend to involve the entire peritoneum or produce pain that is not well-localized:
| Cause | Notes |
|---|---|
| Peritonitis (any cause) | Rigid abdomen, board-like |
| Bowel obstruction | Colicky, diffuse, with distension and vomiting |
| Early appendicitis | Starts periumbilical before localizing to RLQ |
| Pancreatitis | Can be diffuse or epigastric; radiates to back |
| Gastroenteritis | Crampy, associated with diarrhea/vomiting |
| Mesenteric ischemia | Severe pain out of proportion to signs |
| Aortic aneurysm (leaking/ruptured) | Sudden severe pain, pulsatile mass |
| Perforated bowel | Sudden onset, peritoneal signs |
| Volvulus | Crampy colicky pain, massive distension |
| Sickle cell crisis | Known history, systemic features |
| Metabolic disorders | Diabetic ketoacidosis (DKA), Addisonian crisis, porphyria, uremia |
| Familial Mediterranean fever | Recurrent episodic attacks |
| Heavy metal poisoning | Lead, arsenic |
| Hereditary angioedema | Episodic, no urticaria |
| Narcotic withdrawal | Drug history |
| Malaria | Fever, travel history |
| Abdominal compartment syndrome | Post-trauma/surgery setting |
Right Upper Quadrant (RUQ) / Right Hypochondriac Pain
The liver, gallbladder, and right lobe of the diaphragm are the main structures here.
| Cause | Key Features |
|---|---|
| Biliary colic | Colicky RUQ, radiates to right scapula, after fatty meals; resolves in <6 hours |
| Acute cholecystitis | Persistent RUQ pain, positive Murphy's sign, fever, nausea |
| Cholangitis | Charcot's triad: RUQ pain + fever + jaundice |
| Hepatitis (viral, alcoholic, autoimmune) | RUQ dull ache, jaundice, elevated LFTs |
| Hepatic abscess | Fever, tender hepatomegaly |
| Hepatic congestion (right heart failure) | Dull RUQ, raised JVP, peripheral edema |
| Duodenal ulcer | Epigastric-RUQ, relieved by food, worse at night |
| Subphrenic abscess | Post-surgical, shoulder tip pain |
| Myocardial ischemia / infarction | Referred pain - especially inferior MI; ECG mandatory |
| Pneumonia (right lower lobe) | Pleuritic, respiratory signs present |
| Pulmonary embolism | Pleuritic chest/right side pain, hypoxia |
| Herpes zoster | Dermatomal pain before rash |
Epigastric Pain
The stomach, duodenum, pancreas, and aorta are the main sources.
| Cause | Key Features |
|---|---|
| Peptic ulcer disease (gastric/duodenal) | Burning, relationship to meals, H. pylori |
| Perforated peptic ulcer | Sudden severe "knife-like" pain, peritonitis |
| Gastritis / esophagitis | Burning, worse with food/alcohol/NSAIDs |
| GERD | Burning, worse lying down, regurgitation |
| Acute pancreatitis | Severe, radiates to back, relieved leaning forward; elevated lipase/amylase |
| Aortic aneurysm | Pulsatile epigastric mass, radiates to back |
| Myocardial infarction | Do not miss - get ECG in all epigastric pain |
| Mesenteric ischemia | Severe pain out of proportion to exam |
Left Upper Quadrant (LUQ) / Left Hypochondriac Pain
The stomach, spleen, left kidney, pancreatic tail, and left lung are here.
| Cause | Key Features |
|---|---|
| Gastric ulcer / gastritis | Burning, worse with food |
| Splenic rupture | Trauma history, Kehr's sign (referred to left shoulder) |
| Splenomegaly / splenic abscess | Fullness, dull ache |
| Pancreatitis (tail) | Radiates to left back |
| Pneumonia (left lower lobe) | Respiratory signs, pleuritic |
| Pulmonary embolism | Pleuritic left-sided pain |
| Myocardial ischemia | Referred pain to epigastrium/LUQ |
| Herpes zoster | Dermatomal |
Right Lumbar (Right Flank) Pain
| Cause | Key Features |
|---|---|
| Ureteric colic (renal stone) | Severe colicky pain radiating to groin/scrotum/labia; hematuria in 85-90%; peak age 30-40 |
| Pyelonephritis | Dull aching flank pain + fever + dysuria + CVA tenderness |
| Hepatitis | Can extend to right flank |
| Mesenteric ischemia | |
| Small bowel obstruction | Colicky, associated with vomiting |
Left Lumbar (Left Flank) Pain
| Cause | Key Features |
|---|---|
| Ureteric colic | Same features as right, contralateral side |
| Pyelonephritis | Flank tenderness, fever, dysuria |
| Inflammatory bowel disease | Crohn's disease, associated diarrhea |
Umbilical / Periumbilical Pain
| Cause | Key Features |
|---|---|
| Early appendicitis | Begins periumbilical, then migrates to RLQ over 12-24 hours - classic presentation |
| Mesenteric lymphadenitis | Children, viral illness, no migration |
| Meckel's diverticulitis | Children/young adults; mimics appendicitis |
| Umbilical hernia | Visible/palpable |
| Aortic aneurysm | Mid-abdominal pulsatile mass |
| Intestinal obstruction | Colicky |
| Lymphoma | Painless mass, may cause obstruction |
Right Iliac Fossa (RLQ) Pain
This is one of the most clinically important regions.
| Cause | Key Features |
|---|---|
| Appendicitis | Most common surgical cause in young adults; RLQ tenderness, rebound, Rovsing's sign |
| Crohn's disease (terminal ileitis) | Chronic, diarrhea, weight loss, skip lesions |
| Cecal obstruction / volvulus | Colicky, distension |
| Ovarian cyst (ruptured/torsion) | Sudden severe pain, adnexal mass on exam |
| Ectopic pregnancy | Missed period, positive hCG; can rupture causing hemodynamic instability |
| Pelvic inflammatory disease (PID) | Cervical motion tenderness, vaginal discharge, bilateral/unilateral |
| Inguinal hernia (incarcerated/strangulated) | Visible groin bulge, severe pain |
| Endometriosis | Cyclic pain, dysmenorrhea |
| Mittelschmerz | Mid-cycle, brief |
| Psoas abscess | Flexion deformity of hip, fever |
| Ureteral calculi | Radiates to groin, hematuria |
| Herpes zoster | Dermatomal rash |
| Ischemic colitis | Older patients, post-prandial pain |
| Testicular torsion | Adolescents, sudden scrotal/lower abdominal pain |
Left Iliac Fossa (LLQ) Pain
| Cause | Key Features |
|---|---|
| Diverticulitis | Older adults, "left-sided appendicitis," fever, altered bowel habit |
| Ulcerative colitis | Bloody diarrhea, urgency, tenesmus |
| Constipation | Often overlooked, most common cause in primary care |
| Ovarian cyst / torsion | Same as RLQ contralateral |
| Ectopic pregnancy | |
| PID / endometriosis | |
| Inguinal hernia (incarcerated) | |
| Ischemic colitis | |
| Sigmoid volvulus | Elderly/institutionalized; massive distension |
| Ureteral calculi | |
| Aortic aneurysm | Can extend to LLQ |
| Regional enteritis (Crohn's) |
Hypogastric / Suprapubic Pain
| Cause | Key Features |
|---|---|
| Cystitis (UTI) | Burning, frequency, urgency, pyuria |
| Urinary retention | Inability to void, distended bladder, elderly male (BPH) |
| Testicular torsion | Adolescents; also may feel suprapubic |
| Ovarian pathology (bilateral cysts, torsion) | |
| Uterine causes (fibroids, endometriosis) | |
| Placental abruption / obstetric causes | Pregnant patient |
| PID | Bilateral pelvic tenderness |
| Bladder outlet obstruction / BPH | |
| Prostatitis | Perineal and suprapubic ache, dysuria |
Referred Pain - Important Clinical Pitfalls
Some extra-abdominal conditions present as abdominal pain:
| Extra-abdominal Source | Location of Referred Pain |
|---|---|
| Inferior MI / coronary ischemia | Epigastric or RUQ |
| Right lower lobe pneumonia | RUQ / right flank |
| Left lower lobe pneumonia | LUQ / left flank |
| Pulmonary embolism | Either upper quadrant |
| Diaphragmatic irritation (any cause) | Shoulder tip (Kehr's sign) |
| Testicular pathology | Lower abdominal / groin |
| Hip/spine pathology | Lower abdominal or inguinal |
| Diabetic ketoacidosis | Diffuse |
| Acute MI in elderly/diabetics | Epigastric (silent ischemia) |
Key clinical principle (Goldman-Cecil Medicine): "The site of the abdominal pain has a significant correlation with the organ involved" - but the history must also cover acuity, severity, radiation, duration, pattern (colicky vs. constant), and relationship to food and bowel movements.
A Quick Aide-Memoire: Mnemonic by Quadrant
- RUQ = Gall bladder, Hepatitis, Hepatic abscess, Duodenal ulcer, Cardiac (inferior MI)
- Epigastric = Pancreatitis, Peptic ulcer, Perforated ulcer, GERD, MI
- LUQ = Spleen, Stomach, Pancreatitis (tail)
- Periumbilical = Early appendicitis, Mesenteric ischemia, Aortic aneurysm
- RLQ = Appendicitis, Crohn's, Ovarian (right), Ectopic (right)
- LLQ = Diverticulitis, Ulcerative colitis, Constipation, Ovarian (left)
- Suprapubic = Cystitis, Uterine, Bladder obstruction
Sources: Tintinalli's Emergency Medicine (9e), Sleisenger & Fordtran's GI and Liver Disease, Goldman-Cecil Medicine (2-vol set), Yamada's Textbook of Gastroenterology (7e), Lecturio Differential Diagnosis Diagram
This is a shared conversation. Sign in to Orris to start your own chat.