Enterohepatic circulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of enterohepatic circulation, drawn from multiple authoritative textbooks.
Enterohepatic Circulation
Definition
Enterohepatic circulation (EHC) refers to the cyclic movement of substances — primarily bile acids/salts — secreted by the liver into bile, delivered to the intestine, reabsorbed (mainly in the terminal ileum), returned to the liver via the portal vein, and re-secreted into bile. It is essentially a conservation loop between the intestine and the liver.
Anatomic Components
The anatomic components are:
- Liver (site of synthesis and re-uptake)
- Biliary tract and gallbladder (storage and delivery)
- Sphincter of Oddi (valve controlling flow)
- Small intestine (site of function + reabsorption)
- Ileocecal valve
- Portal venous circulation (return pathway)
- Colon (minor site of passive absorption + bacterial modification)
The system can be thought of as a series of storage chambers (gallbladder, small intestine), valves (sphincter of Oddi, ileocecal valve), mechanical pumps (intestinal peristalsis), and chemical pumps (hepatocyte, cholangiocyte, ileocyte transporters).
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Bile Acid Pool and Cycling
| Parameter | Value |
|---|---|
| Total bile salt pool | ~2.5 g |
| Amount secreted/day | 15–30 g/day |
| Amount recycled | >95% (>97%) |
| Fecal loss | ~0.5 g/day |
| Daily hepatic synthesis to replace loss | ~0.5 g/day |
The pool recycles 6–10 times per day. Between meals, bile acids are concentrated ~10-fold in the gallbladder. After a meal, CCK triggers gallbladder contraction and sphincter of Oddi relaxation, releasing bile into the duodenum.
The Circuit — Step by Step
1. Hepatic Synthesis & Secretion
- Cholesterol → Primary bile acids (cholic acid [CA] and chenodeoxycholic acid [CDCA]) via the rate-limiting enzyme cholesterol 7α-hydroxylase (CYP7A1)
- Conjugated with glycine or taurine → Primary bile salts (ionized form)
- Secreted into bile canaliculi by the Bile Salt Export Pump (BSEP / ABCB11)
- Transported to duodenum via the bile duct (stored in gallbladder between meals)
2. Intestinal Transit & Function
- In the small intestine, bile salts form mixed micelles with phospholipids and cholesterol, facilitating:
- Emulsification of dietary fats
- Activation of pancreatic lipase on triglycerides
- Solubilization of fat-soluble vitamins (A, D, E, K) for absorption
- Concentration in intestinal lumen: 5–10 mmol/L (threshold for micelle formation: ~1.5 mmol/L)
3. Bacterial Modification (Colon / Distal Gut)
- Gut bacteria deconjugate bile salts (remove glycine/taurine)
- Dehydroxylate at carbon-7 → Secondary bile acids:
- Cholic acid → Deoxycholic acid (DCA)
- Chenodeoxycholic acid → Lithocholic acid (LCA)
- A small proportion of secondary bile acids are reabsorbed from the colon and returned to the liver
4. Ileal Reabsorption (Key Step)
- Active, Na⁺-coupled reabsorption in the terminal ileum via ASBT (Apical Sodium-dependent Bile acid Transporter / SLC10A2)
- Exit across the basolateral membrane via OST α/β (Organic Solute Transporter)
- Enter the portal circulation (transported bound to albumin)
- Strategically located in the terminal ileum so bile salts are present at high concentration throughout the entire small bowel for maximal fat absorption
5. Hepatic Re-uptake
- Portal blood delivers bile salts back to hepatocytes
- Taken up by NTCP (Na⁺-taurocholate cotransporting polypeptide / SLC10A1) and OATP1B1/1B3 (organic anion transporters)
- Re-conjugated and re-secreted → cycle repeats
— Lippincott Illustrated Reviews: Biochemistry, 8th ed; Costanzo Physiology, 7th ed
Diagram: Enterohepatic Circulation of Bile Salts
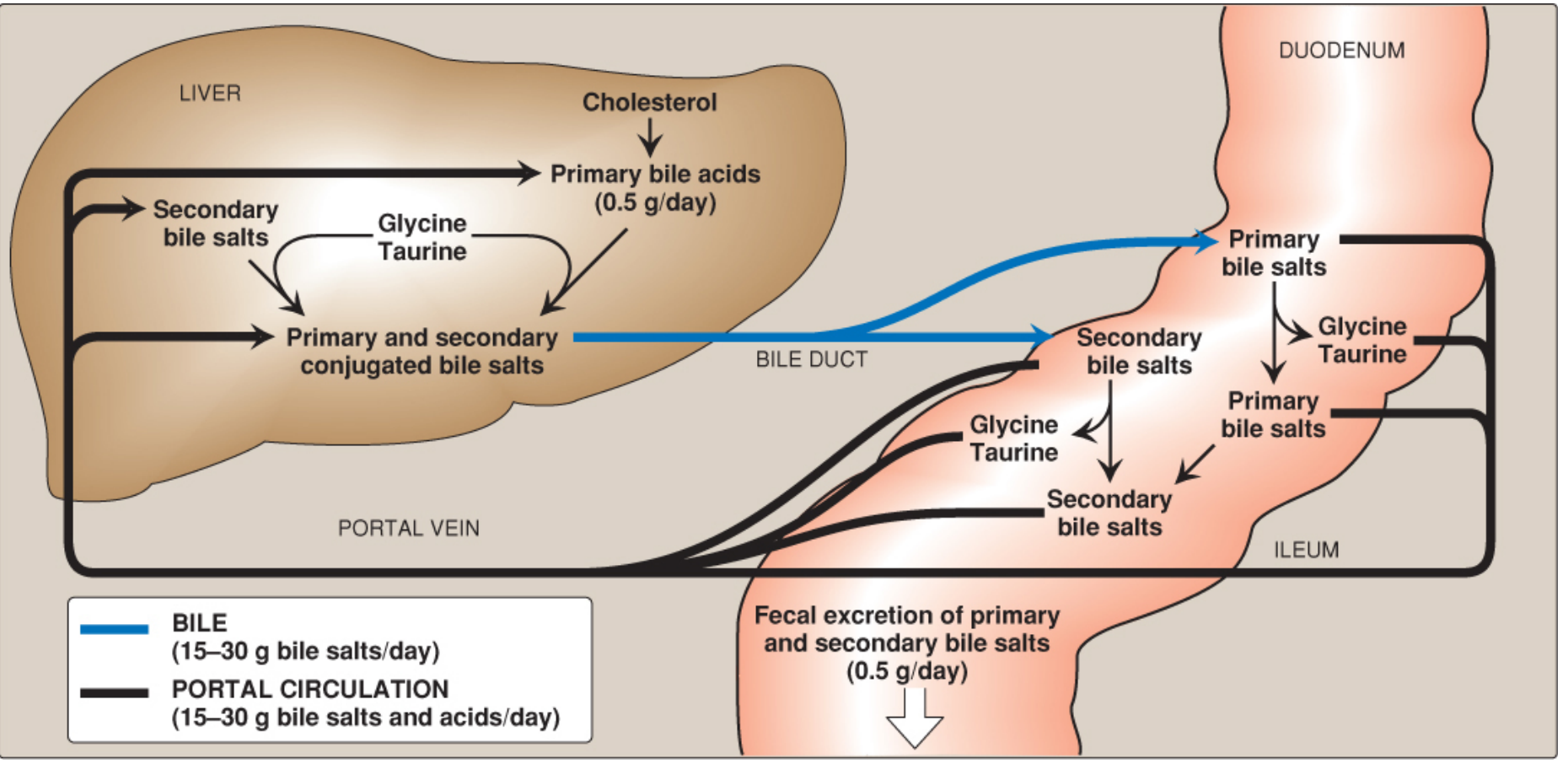
Enterohepatic circulation of bile salts — Lippincott Illustrated Reviews: Biochemistry, 8th ed
Diagram: Transport Proteins Involved
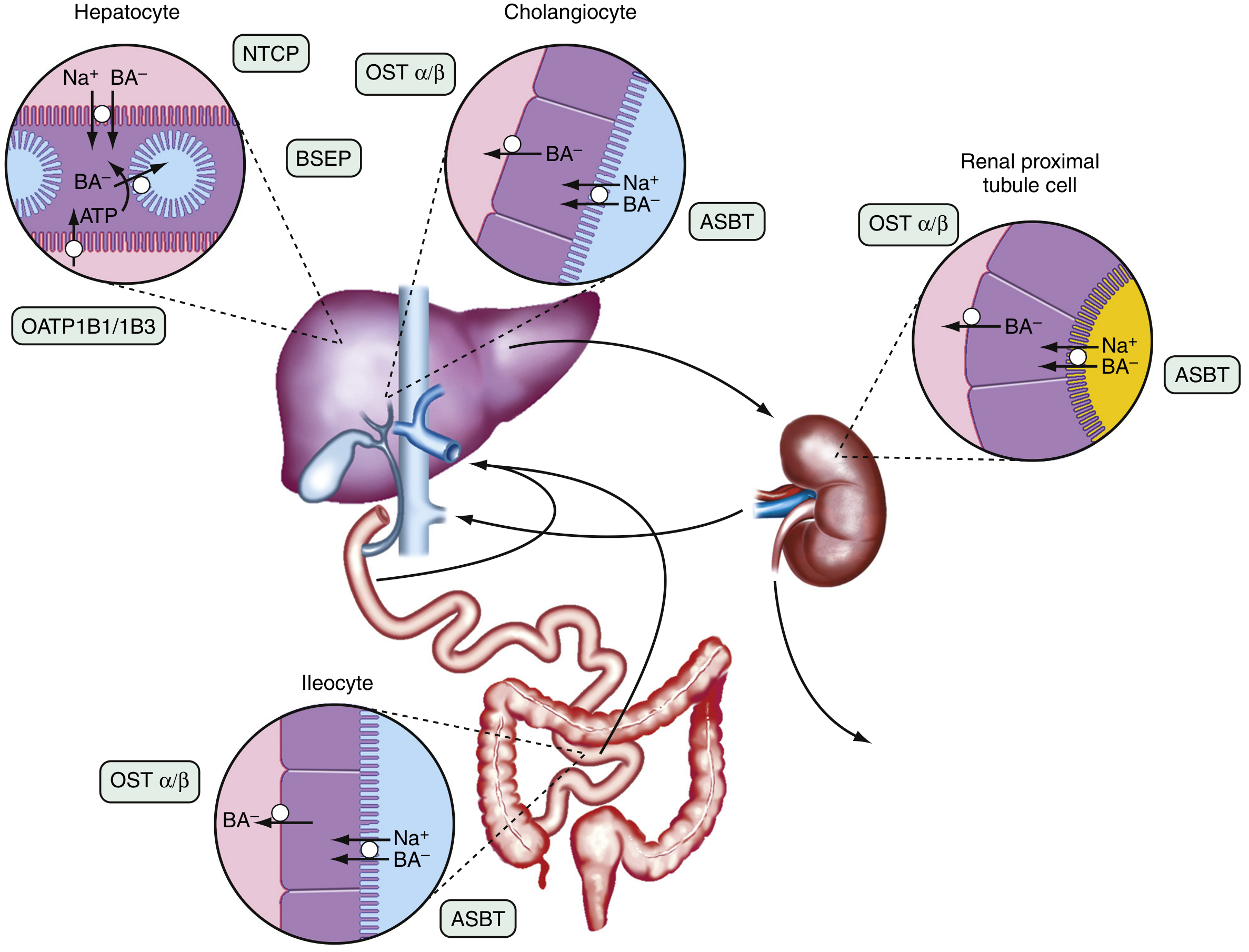
Transport proteins of the enterohepatic circulation — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Regulation: Feedback Control
- Bile salts inhibit CYP7A1 (cholesterol 7α-hydroxylase) → negative feedback on synthesis
- When more bile salts return to the liver → synthesis decreases
- When less returns (e.g., ileal resection, cholestyramine) → synthesis is maximally stimulated but may not compensate → pool depletion
- FGF19 (fibroblast growth factor 19), released from ileal enterocytes in response to bile acid reabsorption, also inhibits CYP7A1 and induces gallbladder relaxation during the interdigestive period
- TGR5 (G-protein coupled receptor) is activated directly by bile acids
Physiological Significance
- Cholesterol elimination: The enterohepatic circulation is the primary mechanism for eliminating excess cholesterol — it is converted to bile acids and lost in feces
- Fat digestion: Recycling ensures adequate bile salt concentration for lipid absorption across the full length of the small intestine
- Choleretic effect: Returning bile salts to the liver stimulates further bile secretion (choleresis)
— Sabiston Textbook of Surgery
Clinical Consequences of Disruption
Ileal Resection / Crohn's Disease (Terminal Ileum)
- Loss of active reabsorption → massive fecal bile acid loss
- Synthesis cannot compensate → pool depletion
- Reduced micellar solubilization → steatorrhea, fat-soluble vitamin deficiency
- Bile acids reaching the colon → choleretic diarrhea (bile acid diarrhea)
Disorders of Enterohepatic Circulation (Classification)
- Defects in bile acid synthesis/conjugation (e.g., CYP7A1 deficiency, Zellweger syndrome)
- Defects in membrane transport (e.g., BSEP mutations → progressive familial intrahepatic cholestasis)
- Disturbances in bacterial transformation (e.g., bacterial overgrowth → premature deconjugation → reduced micelle formation)
- Disturbances in bile acid circulation (e.g., cholestasis, ileal disease)
— Sleisenger and Fordtran's GI and Liver Disease
Cholelithiasis (Gallstones)
- Disruption of the bile salt:cholesterol:phospholipid ratio → cholesterol crystallizes in the gallbladder
- Caused by reduced bile acids or increased cholesterol secretion (e.g., fibrate therapy)
Pharmacological Relevance
Bile Acid Sequestrants (Cholestyramine, Colesevelam)
- Bind bile salts in the gut → prevent reabsorption → increase fecal excretion
- Relieves negative feedback on CYP7A1 → liver diverts more cholesterol into bile acid synthesis → lowers serum LDL cholesterol
- Also used in bile acid diarrhea and cholestatic pruritus
Drugs with Significant Enterohepatic Circulation
Some drugs are excreted in bile, deconjugated by intestinal bacteria, reabsorbed from the gut, and recirculated — giving them prolonged half-lives or secondary plasma peaks:
- Diazepam (secondary plasma peak at 6–12 hours)
- Morphine, carbamazepine, digoxin, doxepin, phenobarbital, piroxicam, dapsone
- Disruption by antibiotics (killing gut flora) or activated charcoal (interrupts recirculation) can lower drug levels
Multidose Activated Charcoal
- Particularly useful for drugs that undergo enterohepatic circulation and have long half-lives, as it interrupts re-absorption with each cycle
— Morgan & Mikhail's Clinical Anesthesiology, 7e; Lippincott Biochemistry, 8th ed
Summary
| Component | Role |
|---|---|
| Liver (BSEP) | Secretes bile salts into bile |
| Gallbladder | Concentrates and stores bile between meals |
| CCK | Triggers gallbladder contraction post-meal |
| Small intestine | Site of micelle formation and lipid absorption |
| Terminal ileum (ASBT) | Active reabsorption of >95% of bile salts |
| Portal vein | Returns bile salts to liver |
| Liver (NTCP/OATP) | Re-uptakes bile salts from portal blood |
| CYP7A1 | Rate-limiting synthesis enzyme, feedback inhibited by bile salts |
| Gut bacteria | Generate secondary bile acids (DCA, LCA) |
| Feces | Final excretion route (~0.5 g/day) |
This is a shared conversation. Sign in to Orris to start your own chat.