Transverse myelitis
Reading File
Finding Sources
Searching PubMed
"transverse myelitis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
transverse myelitis MRI spinal cord T2
Here is a comprehensive overview of Transverse Myelitis (TM):
Definition
Transverse myelitis is an acute or subacute inflammatory-demyelinating disorder of the spinal cord that interrupts ascending and descending pathways, producing motor, sensory, and autonomic dysfunction below the lesion level. The term "transverse" implies involvement across the full cross-sectional width of the cord at a given level, though involvement may be incomplete. It is rare, affecting approximately 1 in 100,000 people.
Etiology & Pathogenesis
The pathogenesis is presumed to be autoimmune. Key associations include:
| Category | Examples |
|---|---|
| Inflammatory/demyelinating | Multiple sclerosis (MS), Neuromyelitis optica spectrum disorder (NMOSD) |
| Autoimmune/connective tissue | SLE, Sjögren syndrome, antiphospholipid antibody syndrome, vasculitis |
| Post-infectious / Para-infectious | HSV, VZV, CMV, EBV, enterovirus (~30% of cases preceded by viral illness) |
| Post-vaccinal | Rabies, polio vaccines |
| Vascular | Spinal cord infarction, dural arteriovenous fistula |
| Paraneoplastic | Paraneoplastic myelopathy |
| Idiopathic | No cause found in ~30% |
Progression is rapid: 66% reach maximal deficit within 24 hours, though symptoms may evolve over days to weeks. The thoracic cord is most commonly involved (60–70% of cases).
Clinical Features
- Motor: Weakness progressing to paraparesis/paraplegia; hyperreflexia, hypertonia, clonus, Babinski signs (UMN pattern after acute phase)
- Sensory: Ascending paresthesias, loss of deep sensation in the feet, a clear sensory level on the trunk
- Autonomic: Sphincteric dysfunction (bowel, bladder, sexual); in cervical/high thoracic lesions — hemodynamic instability (hyper-/hypotension, brady-/tachycardia)
- Other: Back pain, low-grade fever
In its fulminant form: complete motor and sensory loss below the lesion + bowel, bladder, and sexual dysfunction.
Key Imaging Features
MRI with gadolinium is the diagnostic modality of choice:
- T2: Increased (hyperintense) intramedullary signal
- Cord enlargement/edema
- Gadolinium enhancement in acute phase (blood-spinal cord barrier breakdown)
- Longitudinally Extensive TM (LETM): Lesion spanning ≥3 vertebral segments — hallmark of NMOSD
MS-related TM tends to be short-segment, peripheral/asymmetric.
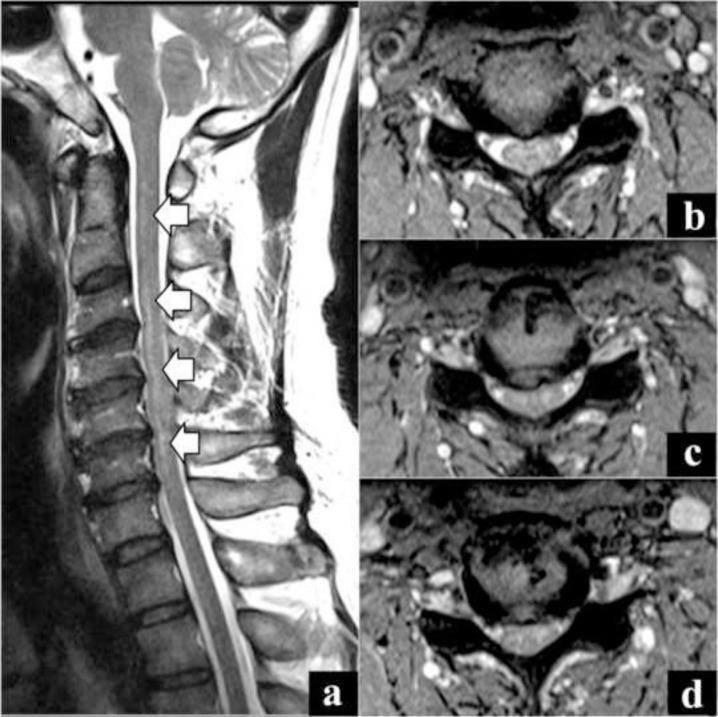
Sagittal T2 MRI showing longitudinally extensive transverse myelitis (LETM) from C2–C7 with bilateral central hyperintensity on axial views — characteristic of NMOSD.
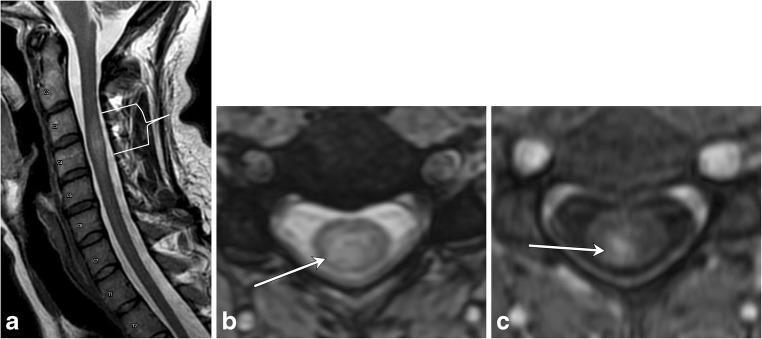
Cervical TM: (a) Short-segment T2 cord hyperintensity with focal expansion; (b) Axial T2 showing >2/3 cord area involvement; (c) Post-contrast T1 showing dusky enhancement.
Diagnosis
Transverse myelitis is primarily a clinical diagnosis confirmed by MRI. Essential workup:
- MRI spine with gadolinium — exclude compressive etiology; characterize lesion
- MRI brain — look for disseminated demyelinating lesions (MS)
- CSF analysis — lymphocytic pleocytosis + elevated protein (but normal in ~40% of cases); oligoclonal bands
- Serology: Anti-AQP4 (aquaporin-4) IgG (NMO-IgG), anti-MOG IgG, ANA, antiphospholipid antibodies
- Spinal angiography if vascular cause suspected (older patients, vascular risk factors, central cord edema on MRI)
Primary Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| MS | Short, asymmetric/incomplete lesion; brain MRI dissemination |
| NMOSD | LETM (≥3 segments), bilateral optic neuritis, anti-AQP4 positive |
| Spinal cord compression | Spondylosis, disc, tumor — excluded by MRI |
| Spinal epidural abscess/hematoma | Fever/coagulopathy; extradural mass on MRI |
| Spinal cord infarction | Sudden onset, vascular risk factors, DWI restricted diffusion |
| Paraneoplastic | Systemic malignancy, anti-neuronal antibodies |
Treatment
Acute Phase
- IV Methylprednisolone 1000 mg/day × 3–5 days — first-line for most cases
- Plasma exchange (PLEX) — steroid-refractory cases
- IVIG — alternative in refractory cases
- Cyclophosphamide — considered in refractory/severe cases
NMOSD-Specific (Relapse Prevention)
| Agent | Mechanism | Dosing |
|---|---|---|
| Satralizumab | Anti-IL-6 receptor (humanized mAb) | 120 mg SC at 0, 2, 4 weeks, then every 4 weeks |
| Eculizumab | Terminal complement inhibitor | 900 mg IV weekly ×4, then 1200 mg every 2 weeks |
| Tocilizumab | IL-6 receptor inhibitor | 8 mg/kg IV every 4 weeks |
| Rituximab | Anti-CD20 | 1000 mg IV, two doses 2 weeks apart, every 6 months |
| Azathioprine | Purine antimetabolite | 3 mg/kg/day |
Prognosis
- Most idiopathic cases: partial recovery begins 1–3 months after onset; maximal improvement by 3–6 months
- Outcomes: ~30% "good" recovery, ~25% "fair," ~30% "poor" (remain paralyzed); 15% mortality at 5 years
- Overall prognosis worse than MS — significant recovery seen in fewer than 50%
- ~1/3 of patients who present with isolated acute myelitis eventually develop clinical MS within 5 years (similar conversion rate to those presenting with optic neuritis)
- LETM (NMOSD) carries higher risk of sustained disability with recurrent attacks
TM vs. MS vs. NMOSD — Key Distinctions
| Feature | MS-TM | Idiopathic TM | NMOSD-TM |
|---|---|---|---|
| Lesion extent | Short-segment (<3 levels) | Often ≥3 levels | LETM (≥3 levels) |
| Cord involvement | Peripheral, asymmetric | Central, full cross-section | Central, full cross-section |
| Brain MRI | Periventricular plaques | Usually normal | Brainstem predilection |
| Anti-AQP4 | Negative | Negative | Positive (hallmark) |
| Course | Relapsing-remitting | Usually monophasic | Relapsing, severe |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine, 2e; Rosen's Emergency Medicine; Adams and Victor's Principles of Neurology, 12e; Localization in Clinical Neurology, 8e
This is a shared conversation. Sign in to Orris to start your own chat.