Relation of retina and diabetes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
diabetic retinopathy fundus classification stages
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile a thorough answer.
Diabetic Retinopathy: Relation of the Retina and Diabetes
Overview
Diabetic retinopathy (DR) is the most common cause of new blindness in industrialised countries among working-age adults. It is a pathognomonic microvascular complication that eventually affects more than 50% of people with long-standing diabetes. With effective screening and treatment (ETDRS, anti-VEGF trials), the risk of severe visual loss can be reduced to less than 5%.
— Kanski's Clinical Ophthalmology, 10th Ed.
Pathogenesis
DR is predominantly a microangiopathy — small retinal blood vessels are particularly vulnerable to damage from sustained hyperglycaemia. Key mechanisms include:
| Mechanism | Details |
|---|---|
| Pericyte loss | Supporting cells of retinal capillaries are lost early |
| Basement membrane thickening | Structural weakening of vessel walls |
| Altered retinal blood flow | Leads to areas of ischaemia |
| Capillary leak | Protein, red blood cells, and lipids leak → retinal oedema |
| Capillary occlusion | Causes chronic retinal hypoxia |
| Neovascularisation | VEGF-driven; new vessels are fragile and rupture-prone |
VEGF (Vascular Endothelial Growth Factor) is the principal angiogenic mediator driving neovascularisation.
— Goldman-Cecil Medicine; Kanski's Clinical Ophthalmology
Ophthalmic Complications of Diabetes
Common:
- Diabetic maculopathy — diabetic macular oedema (DMO) and macular ischaemia
- Retinopathy — neovascularisation of disc/retina, vitreous haemorrhage
- Unstable refraction (osmotic refractive changes — common at diagnosis or with high glucose)
Uncommon/Rare:
- Accelerated age-related cataract
- Tractional retinal detachment
- Neovascular glaucoma (NVG)
- Ocular motor nerve palsies (CN III or VI — due to diabetic mononeuropathy)
- Neovascularisation of the iris (rubeosis iridis)
- Reduced corneal sensitivity
- Diabetic papillopathy
Classification (ETDRS / International Classification)
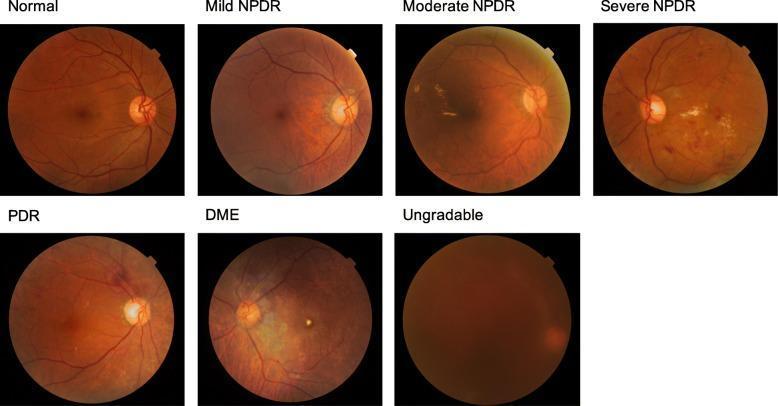
Non-Proliferative Diabetic Retinopathy (NPDR)
| Stage | Key Features | Follow-up |
|---|---|---|
| No DR | Normal | 12 months |
| Very Mild NPDR | Microaneurysms only | 12 months |
| Mild NPDR | Microaneurysms, dot/blot haemorrhages, exudates, cotton-wool spots | 6–12 months |
| Moderate NPDR | Severe haemorrhages, soft exudates, venous beading, IRMA | ~6 months |
| Severe NPDR | >20 intraretinal haemorrhages in all 4 quadrants, OR venous beading in ≥2 quadrants, OR prominent IRMA (4-2-1 rule) | Refer to retinal specialist |
Proliferative Diabetic Retinopathy (PDR)
- Neovascularisation of the disc (NVD) and/or new vessels elsewhere (NVE)
- High-risk PDR: vitreous/pre-retinal haemorrhage, NVD >1/3 disc area, or NVE >1/2 disc area
Advanced Diabetic Eye Disease
- Tractional retinal detachment
- Persistent vitreous haemorrhage
- Neovascular glaucoma
Clinically Significant Macular Oedema (CSMO)
- Retinal thickening or hard exudates at or approaching the centre of the macula — can occur at any stage
— Kanski's Clinical Ophthalmology; Goldman-Cecil Medicine
Clinical Signs (Fundoscopic Findings)
| Sign | Significance |
|---|---|
| Microaneurysms | Earliest sign; tiny red dots from capillary wall outpouchings |
| Dot and blot haemorrhages | Intraretinal blood from ruptured capillaries |
| Hard exudates | Lipid/protein leakage — yellow waxy deposits |
| Cotton-wool spots | Nerve fibre layer infarcts from capillary occlusion |
| Venous beading | Irregular venous calibre — sign of significant ischaemia |
| IRMA | Intraretinal microvascular anomalies — shunts bypassing ischaemic areas |
| Neovascularisation | Hallmark of PDR — frond-like new vessels |
| Vitreous/preretinal haemorrhage | Ruptured new vessels |
| Traction retinal detachment | Fibrovascular membrane contraction |
Risk Factors for Diabetic Retinopathy
- Duration of diabetes — most important predictor; DR rarely develops within 5 years of onset
- Poor glycaemic control (high HbA1c) — DCCT and UKPDS confirmed tight control prevents/delays DR
- Hypertension — accelerates progression
- Dyslipidaemia — elevated triglycerides worsen macular exudates
- Nephropathy — co-prevalence especially in type 1 DM
- Pregnancy — can accelerate retinopathy; screening required before and during
- Puberty — DR rare before puberty
- Type of diabetes — more common in type 1 than type 2, but type 2 has larger absolute numbers
Paradoxical Worsening with Glycaemic Improvement
A sudden improvement in blood glucose control can cause transient worsening of retinopathy in the first 6–12 months. Long-term, improved control is beneficial. GLP-1 receptor agonists (when associated with marked glycaemic improvement) have been associated with increased risk of worsening DR — this should be factored into choice of therapy. Patients may be candidates for prophylactic laser photocoagulation before rapid normalisation (e.g., prior to pancreas/islet transplantation).
— Harrison's Principles of Internal Medicine, 22nd Ed.
Screening Recommendations
| Diabetes Type | Start Screening |
|---|---|
| Type 2 DM | At diagnosis (hyperglycaemia may have been present years before clinical recognition) |
| Type 1 DM | 5 years after diagnosis |
| Pregnancy | Before and during pregnancy |
- Routine non-dilated exams are inadequate — requires dilated fundus exam or retinal photography with remote reading
- Significant retinopathy can be present with no symptoms — Harrison's; Goldman-Cecil Medicine
Treatment
| Modality | Indication |
|---|---|
| Glycaemic control | Primary prevention and slowing progression |
| Blood pressure control | Reduces progression |
| Panretinal laser photocoagulation (PRP) | Severe NPDR and PDR; ablates ischaemic retina to reduce VEGF drive |
| Anti-VEGF agents (ranibizumab, aflibercept, bevacizumab — intravitreal injection) | Diabetic macular oedema; proliferative DR; equally successful as laser |
| Focal/grid laser | Clinically significant macular oedema |
| Vitrectomy | Vitreous haemorrhage, traction retinal detachment involving macula |
| Fenofibrate | May reduce DR progression (lowers triglycerides) |
| Aspirin | Does NOT influence natural history; antiplatelet agents can be continued with intravitreal injections |
— Harrison's Principles of Internal Medicine; Goldman-Cecil Medicine; Kanski's Clinical Ophthalmology
Key Takeaways
- DR is a microvascular complication driven by chronic hyperglycaemia and mediated largely by VEGF
- It progresses through well-defined stages: No DR → Mild NPDR → Moderate NPDR → Severe NPDR → PDR → Advanced disease
- Macular oedema is the leading cause of visual impairment; proliferative disease causes blindness via haemorrhage and traction
- DR is largely asymptomatic until late stages — screening is essential
- Treatment is highly effective when started early; most blindness from DR is preventable
This is a shared conversation. Sign in to Orris to start your own chat.