Relation of diabetes and retina
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
diabetic retinopathy fundus findings microaneurysms neovascularization
Reading File
Reading File
Reading File
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile a thorough answer.
Diabetes and the Retina — Diabetic Retinopathy
Overview
Diabetic retinopathy (DR) is the commonest cause of new blindness in industrialized countries among working-age adults. It is a microvascular complication of diabetes that ultimately affects more than 50% of people with long-standing disease, though with effective screening and modern treatment the risk of severe visual loss can be reduced to less than 5%.
— Kanski's Clinical Ophthalmology, p. 506
Ophthalmic Complications of Diabetes
| Frequency | Complication |
|---|---|
| Common | Maculopathy (DME, macular ischaemia), Retinopathy (ischaemia → neovascularization, vitreous haemorrhage), Unstable refraction |
| Uncommon | Recurrent styes, Xanthelasma, Accelerated cataract |
| Serious | Tractional retinal detachment, Neovascular glaucoma, Ocular motor nerve palsies |
| Rare | Diabetic papillopathy, acute-onset cataract, rhino-orbital mucormycosis |
Pathogenesis
DR is predominantly a microangiopathy. Chronic hyperglycaemia causes direct damage to retinal small vessels through several mechanisms:
- Pericyte loss — the supporting cells of retinal capillaries are selectively destroyed
- Basement membrane thickening
- Altered retinal blood flow
- Capillary leakage — damaged vessels leak protein, red blood cells, and lipids → retinal oedema
- Capillary occlusion → retinal hypoxia → upregulation of VEGF (Vascular Endothelial Growth Factor)
- Neovascularization — VEGF drives growth of new, fragile, abnormal vessels prone to rupture
— Goldman-Cecil Medicine, p. 1556; Kanski's Clinical Ophthalmology, p. 522
Risk Factors
| Factor | Notes |
|---|---|
| Duration of diabetes | Most important predictor; DR rarely appears within 5 years or before puberty |
| Poor glycaemic control (HbA1c ↑) | DCCT and UKPDS confirm tight control prevents/delays DR |
| Hypertension | Must be controlled <140/80 mmHg; particularly important in T2DM maculopathy |
| Nephropathy | Severe nephropathy worsens DR; renal transplantation may improve it |
| Pregnancy | Can accelerate progression, especially if pre-existing DR or pre-eclampsia |
| Hyperlipidaemia | Fenofibrate may slow progression |
| Type 1 > Type 2 | Prevalence in T2DM is 67% at 10 years; 10% develop proliferative disease |
| Drugs | Pioglitazone → worsening DME; GLP-1 agonists with rapid glycaemic improvement may worsen DR |
Note: A sudden improvement in glycaemic control paradoxically can cause transient worsening of DR.
— Kanski's Clinical Ophthalmology, p. 507; Harrison's Principles of Internal Medicine 22E, p. 3267
Classification
ETDRS / International Classification
| Stage | Clinical Features | Follow-up |
|---|---|---|
| No DR | Normal | 12 months |
| Mild NPDR | Microaneurysms only | 12 months |
| Moderate NPDR | Microaneurysms, blot haemorrhages, hard exudates, cotton-wool spots, venous beading | 6 months |
| Severe NPDR ("4-2-1 rule") | >20 intraretinal haemorrhages in all 4 quadrants, or venous beading in ≥2 quadrants, or IRMA in ≥1 quadrant | Refer promptly |
| PDR | NVD, NVE, and/or vitreous/preretinal haemorrhage | Urgent treatment |
| DME | Retinal thickening ± hard exudates at/near fovea | Can occur at any stage |
Descriptive clinical categories (Kanski):
- Background DR (BDR): Microaneurysms, dot/blot haemorrhages, hard exudates — the earliest signs
- Preproliferative DR (PPDR): Cotton-wool spots, venous beading, IRMA — signify progressive retinal ischaemia
- Proliferative DR (PDR): NVD (≤1 disc diameter of disc) ± NVE; High-risk PDR = vitreous haemorrhage + neovascularization ≥1/3 disc area
- Advanced diabetic eye disease: Tractional retinal detachment, persistent vitreous haemorrhage, neovascular glaucoma
— Goldman-Cecil Medicine, Table 210-13; Kanski's Clinical Ophthalmology, p. 522; Wills Eye Manual, p. 811
Retinal Signs (What You See on Fundoscopy)
| Sign | Significance |
|---|---|
| Microaneurysms | Earliest sign — focal outpouchings of weakened capillary walls |
| Dot & blot haemorrhages | Intraretinal bleeding from microaneurysms |
| Hard (waxy) exudates | Lipid/protein deposits from leaking capillaries |
| Cotton-wool spots | Nerve fibre layer infarcts → ischaemia marker |
| Venous beading | Irregular vein calibre — severe ischaemia |
| IRMA | Intraretinal microvascular abnormalities — dilated collateral vessels |
| Neovascularization (NVD/NVE) | New fragile vessels → bleed easily |
| Vitreous/preretinal haemorrhage | Rupture of new vessels |
| Tractional retinal detachment | Fibrovascular membranes contract |
| Neovascular glaucoma | Iris/angle neovascularization → IOP rise |
Fundus Images
NPDR — Moderate stage (microaneurysms, dot-blot haemorrhages, cotton-wool spots):

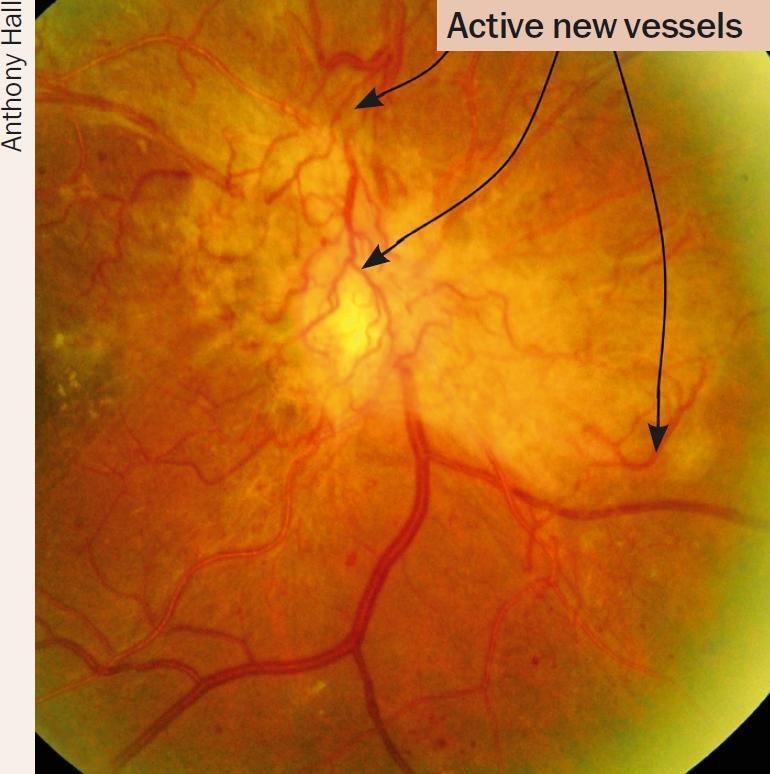
PDR — Proliferative stage (neovascularization of disc and elsewhere, preretinal haemorrhage):
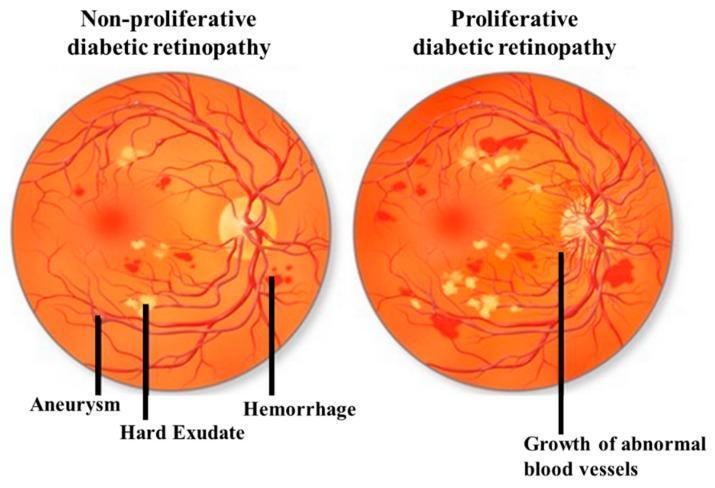
NPDR vs PDR comparison diagram:
Workup
- Dilated fundus exam — 90D/60D lens at slit lamp; indirect ophthalmoscopy for peripheral retina
- Fluorescein angiography (IVFA) — perfusion abnormalities, foveal ischaemia, subclinical NVE
- OCT — macular thickness, detect DME
- OCT-Angiography (OCTA) — central macular ischaemia
- Systemic labs: HbA1c, fasting glucose, lipid panel, blood pressure
— Wills Eye Manual, p. 813
Treatment
Diabetic Macular Oedema (DME)
- Anti-VEGF agents (first-line for centre-involving DME): ranibizumab, aflibercept, bevacizumab (off-label)
- Intravitreal corticosteroids: dexamethasone implant, fluocinolone acetonide — for anti-VEGF non-responders; risk of cataract and elevated IOP
- Focal macular laser: for extrafoveal microaneurysms; adjunctive role
Proliferative DR (PDR)
- Panretinal photocoagulation (PRP) — indicated for high-risk characteristics (NVD > ¼ disc area, any NVD with haemorrhage, NVE > ½ disc area with haemorrhage, any NVI/NVA)
- Anti-VEGF therapy — alternative to PRP; preferred if DME coexists or if vitreous haemorrhage limits view
- Vitrectomy — for dense non-clearing VH, traction retinal detachment threatening macula, traction-rhegmatogenous detachment
Systemic Prevention
- Tight glycaemic control (HbA1c target); tight BP control (<140/80 mmHg)
- Fenofibrate to lower triglycerides
- Fenofibrate may reduce DR progression independent of lipid-lowering effect
— Harrison's, p. 3267; Wills Eye Manual, p. 813–814; Goldman-Cecil, p. 1556
Screening Guidelines
- Type 1 DM: Screen at 5 years after diagnosis, then annually
- Type 2 DM: Screen at diagnosis (hyperglycaemia often pre-dates clinical recognition), then annually
- Requires dilated eye exam by ophthalmologist/optometrist or retinal photography with remote grading — routine non-dilated exams are inadequate
- Pregnant women with DM: screen before and during pregnancy; DME in late pregnancy often resolves spontaneously
Key Clinical Pearls
- DR is largely asymptomatic even in severe PDR — screening is essential
- Duration of diabetes is the single most important risk factor
- In T1DM, presence of CKD without retinopathy should prompt investigation for alternative kidney disease causes
- Aspirin does NOT influence the natural history of DR and can be continued in patients on anti-VEGF therapy
- The risk of severe visual loss can be reduced to <5% with proper screening and treatment
This is a shared conversation. Sign in to Orris to start your own chat.