Bronchiectasis
"bronchiectasis"[MeSH Terms] AND ("management" OR "treatment")
Bronchiectasis
Definition
- Robbins & Kumar Basic Pathology, p. 455
- Grainger & Allison's Diagnostic Radiology, p. 155
Etiology and Predisposing Conditions
- Cystic fibrosis - most common hereditary cause; viscid mucus causes obstruction and chronic infection
- Primary ciliary dyskinesia (Kartagener syndrome) - autosomal recessive; abnormal cilia impair mucociliary clearance; triad of bronchiectasis + sinusitis + situs inversus; associated with male infertility
- Immunodeficiency states - especially immunoglobulin deficiencies (hypogammaglobulinemia), leading to recurrent bacterial infections
- Alpha-1-antitrypsin deficiency
- Necrotizing/suppurative pneumonia (Staphylococcus aureus, Klebsiella spp.)
- Tuberculosis - post-TB bronchiectasis is a major cause in endemic regions
- Post-COVID-19 pneumonia (SARS-CoV-2)
- Tumors, foreign bodies, mucus impaction
- Rheumatic disorders, inflammatory bowel disease
- Chronic aspiration, GERD
- Atopic asthma, chronic bronchitis
Pathogenesis
- Obstruction (e.g., foreign body) → impaired secretion clearance → superimposed infection
- Infection → inflammatory damage to bronchial walls + accumulating exudate → further airway distension
- Alternatively: persistent necrotizing infection → poor secretion clearance → obstruction → peribronchial fibrosis → traction dilation
Morphology and Classification
| Type | Morphology |
|---|---|
| Cylindrical | Uniform, regular airway dilation; most common |
| Varicose | Non-uniform, serpiginous (beaded) dilation |
| Cystic | Marked dilation forming cysts, worst severity; air-fluid levels may be present |
Clinical Features
- Chronic productive cough - daily, copious mucopurulent sputum (typically >30 mL/day; may range 10-150+ mL)
- Hemoptysis - from chronically inflamed, friable mucosa; massive bleeding can occur from hypertrophied bronchial arteries
- Dyspnea - progressive exertional then resting dyspnea
- Fever, weight loss, fatigue during exacerbations
- Associated rhinosinusitis and postnasal drip common
- "Dry bronchitis" variant: minimal sputum, often upper lobe involvement
- Haemophilus influenzae
- Staphylococcus aureus
- Pseudomonas aeruginosa (especially in advanced/CF-related disease)
- Nontuberculous mycobacteria (NTM) - must always be screened with AFB smear/culture
Diagnosis
Chest X-Ray
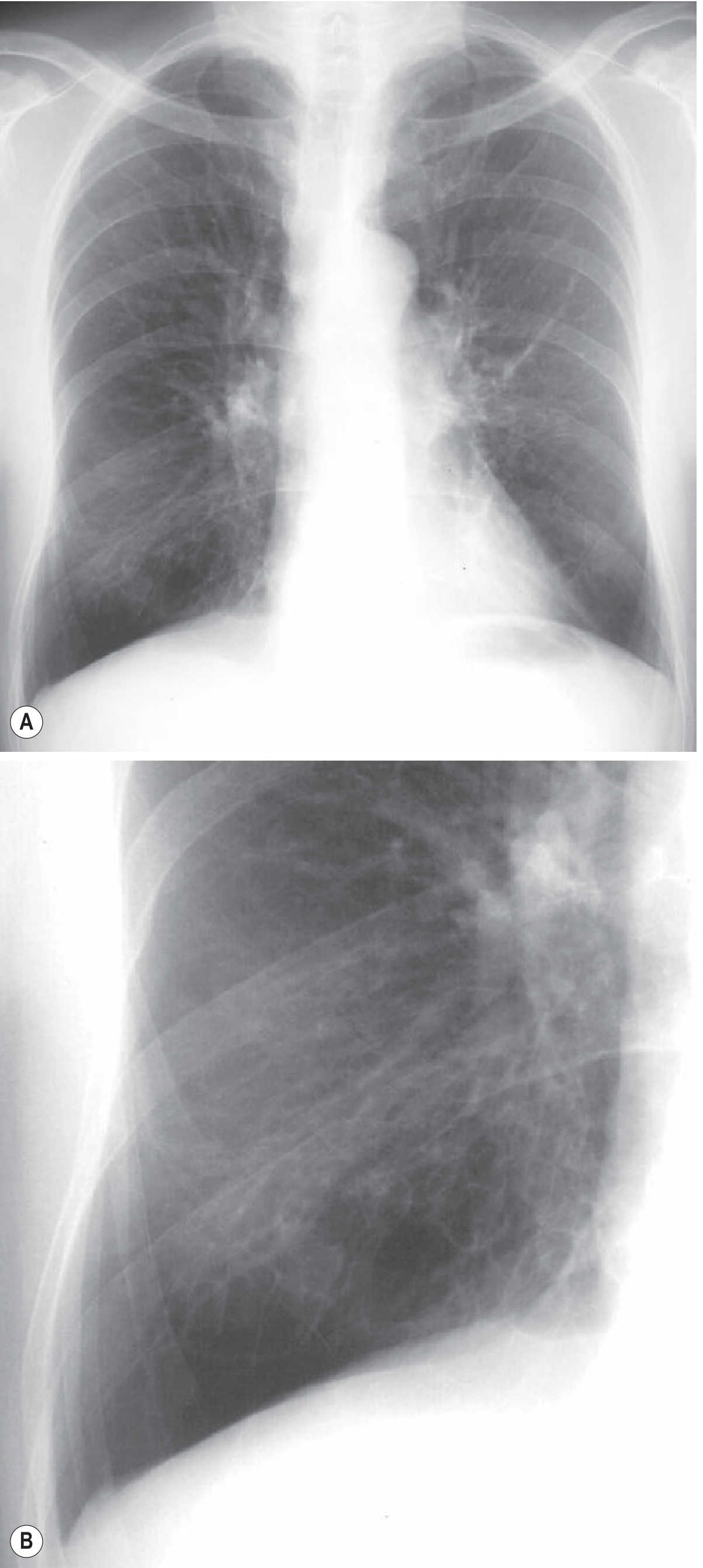
HRCT (Gold Standard)
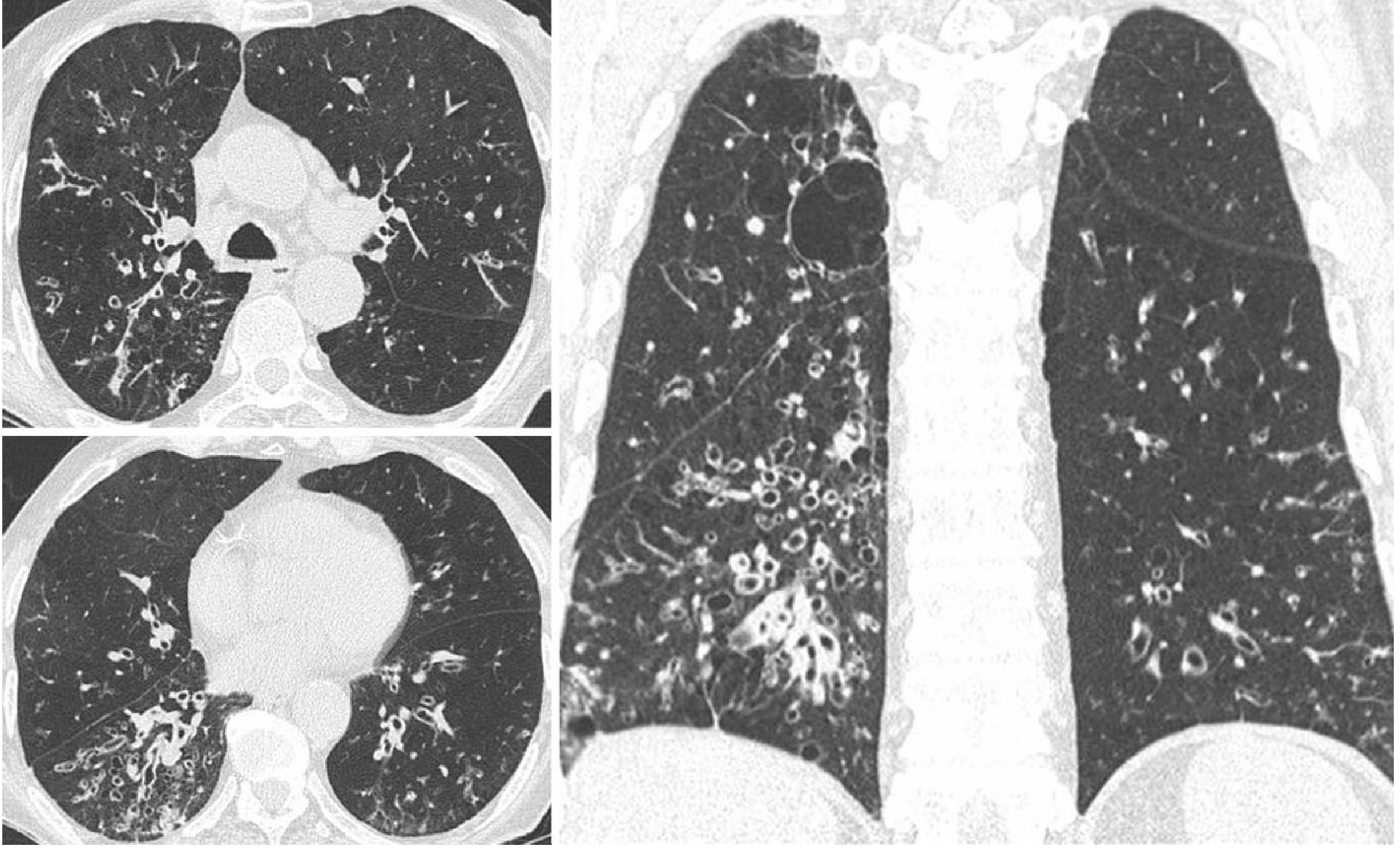
- Lack of tapering of bronchial lumina (cardinal sign)
- Signet ring sign - bronchial internal diameter > adjacent pulmonary artery diameter
- Bronchi visible within 1 cm of the costal pleura or abutting mediastinal pleura
- Mucus-filled dilated bronchi (glove-finger, V- or Y-shaped densities)
- Tree-in-bud sign - small centrilobular nodular/branching opacities reflecting infectious bronchiolitis (~70% of cases)
- Mosaic perfusion and expiratory air-trapping (obliterative bronchiolitis component)
Functional Assessment
- Spirometry: obstructive pattern (reduced FEV1)
- Sputum cultures including AFB
- Immunoglobulin levels, sweat chloride/CFTR testing, ciliary biopsy as indicated
Management
Underlying Cause
Airway Clearance (Cornerstone of Therapy)
- Chest physiotherapy with postural drainage, percussion, and vibration
- Oscillatory positive expiratory pressure devices (e.g., Acapella, flutter valve) - twice-daily use improves sputum volume and quality of life
- High-frequency chest wall oscillation vests
- Nebulized hypertonic saline (3-7%) - enhances mucociliary clearance, reduces exacerbations, improves FEV1 and quality of life; 7% NaCl produces ~15% FEV1 improvement vs. isotonic saline
- Pulmonary rehabilitation and exercise
Note: Recombinant human DNase (dornase alfa), effective in cystic fibrosis, has deleterious effects in non-CF bronchiectasis and should NOT be used.
Anti-inflammatory Therapy
- Long-term macrolide antibiotics (e.g., azithromycin): reduce exacerbations and improve lung function; inhibit cytokine release, neutrophil adhesion, Pseudomonas migration, and biofilm formation. Caveat: screen and exclude active NTM infection before starting macrolides, as they may drive resistance.
- Inhaled corticosteroids: medium-dose budesonide combined with formoterol is more effective than high-dose ICS alone
- Brensocatib (novel neutrophil elastase inhibitor, 10-25 mg orally daily): prolongs time to first exacerbation in non-CF bronchiectasis patients with ≥2 exacerbations/year - Goldman-Cecil Medicine, p. 917
Antimicrobial Therapy
- Acute exacerbations: 2-3 week course of broad-spectrum IV antibiotics tailored to culture/sensitivity, followed by oral regimen
- Inhaled antibiotics (tobramycin, colistin): improve bacterial clearance, may slow FEV1 decline; however, meta-analysis of 12 RCTs (n=1154) showed no reduction in exacerbation risk and no quality-of-life improvement
- Bronchodilators (inhaled β2-agonists): improve mucociliary clearance and reverse associated bronchoconstriction; no routine indication without confirmed airway reactivity
Surgical Options
| Indication | Procedure |
|---|---|
| Localized/refractory disease | Segmental or lobar resection |
| Massive hemoptysis | Bronchial artery embolization ± resection |
| End-stage bilateral disease | Lung transplantation |
Complications
- Progressive airflow obstruction (bronchiectasis in COPD is associated with increased mortality)
- Massive hemoptysis
- Lung abscess, empyema
- Cor pulmonale (right heart failure from chronic hypoxia)
- Amyloidosis (in longstanding disease)
- NTM superinfection
Recent Evidence (2024-2026)
- A 2026 systematic review and meta-analysis on mucoactive agents (PMID 42342264) in bronchiectasis is now published in European Respiratory Review
- A 2026 network meta-analysis in Chest on anti-inflammatory therapies in non-CF bronchiectasis (PMID 41534709) - reinforcing the role of macrolides and evaluating newer agents
- Obstructive sleep apnea has been identified as a significant comorbidity in bronchiectasis (PMID 41905893)
Diagrams for cylinder varcoicise and cyrtix
Medical diagram comparing three types of bronchiectasis side by side: cylindrical (tubular), varicose, and cystic (saccular). Show each type as a cross-sectional and longitudinal airway illustration. Normal bronchus shown first for comparison. Cylindrical bronchiectasis: uniformly dilated, parallel walls, no tapering, smooth walls - like a cylinder. Varicose bronchiectasis: irregular alternating dilation and constriction giving a beaded or varicose vein appearance, outpouchings along the wall. Cystic (saccular) bronchiectasis: balloon-like peripheral sacs at the end of bronchi, cluster of cysts, often with air-fluid levels depicted inside the cysts. Label each type clearly with its name and key features. Include a severity arrow showing cylindrical is mild, varicose is moderate, cystic is severe. Clean medical illustration style with anatomical labels, white background.
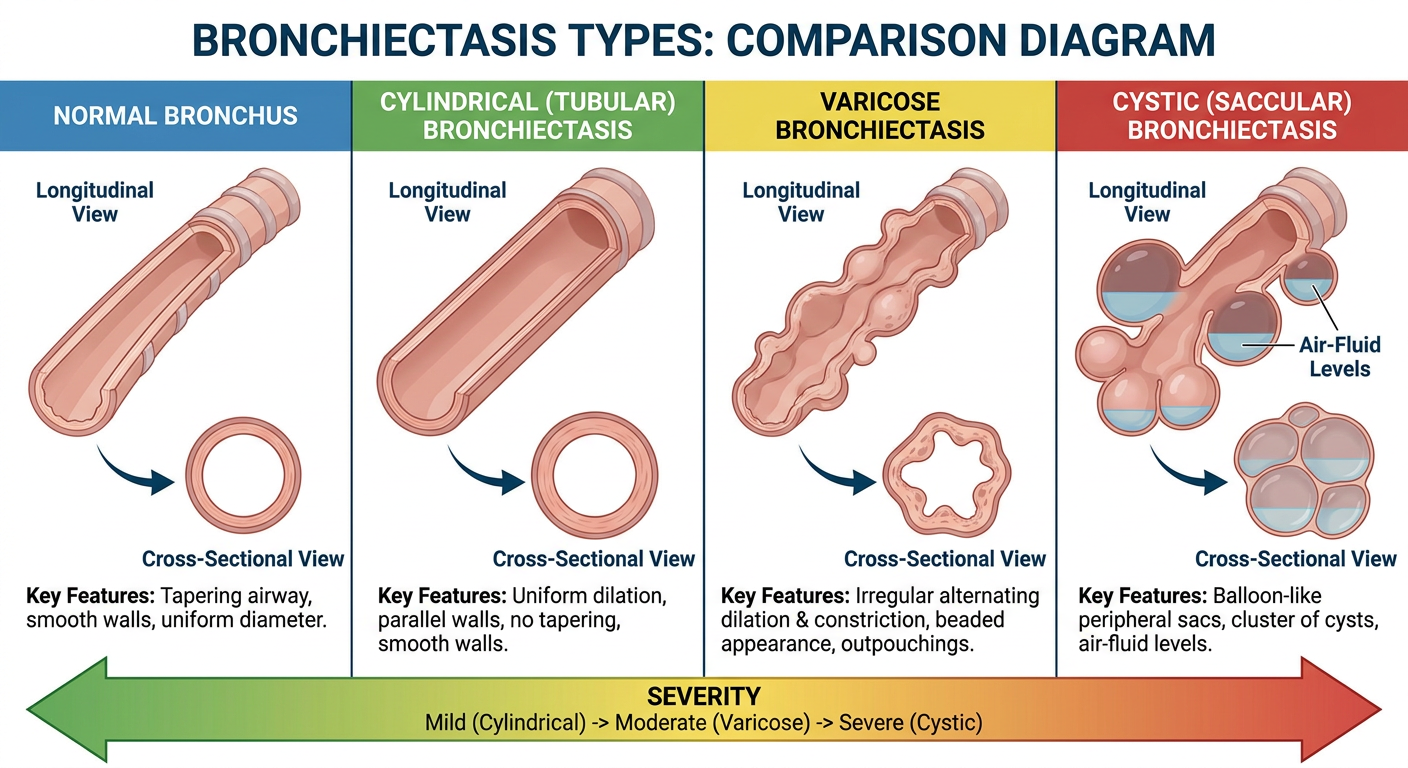
Three Types of Bronchiectasis
1. Cylindrical (Tubular) - Mild
- Airways are uniformly and symmetrically dilated with no tapering as they travel distally
- Bronchial walls are smooth and regular
- On HRCT: "tram-track sign" on longitudinal view; signet ring sign on cross-section (bronchus larger than adjacent pulmonary artery)
- Mildest form; best prognosis
2. Varicose - Moderate
- Irregular alternating dilation and constriction of the airway wall, resembling varicose veins
- Non-uniform, serpiginous (twisting) dilation with focal outpouchings
- On HRCT: beaded configuration of the bronchial lumen
- Intermediate severity
3. Cystic (Saccular) - Severe
- Balloon-like or grape-like peripheral sacs at the end of bronchi
- Distal airways destroyed and replaced by clusters of cysts
- On HRCT: string of cysts (bronchi cut along their length) or cluster of cysts (adjacent dilated bronchi); air-fluid levels common from retained secretions
- Most severe form; most common after bronchial obstruction or severe necrotizing infection
- Confluent cystic distortion produces bronchiectatic consolidation and volume loss
Severity increases: Cylindrical → Varicose → Cystic
??
- Did the diagram not load or display properly?
- Did you want a different style of diagram?
- Do you have a follow-up question about bronchiectasis?
- Was there something unclear in the previous response?
Cor pulmonale
"cor pulmonale"[MeSH Terms] AND "pulmonary hypertension"[MeSH Terms]
Cor Pulmonale
Definition
- Robbins & Kumar Basic Pathology, p. 363
Etiology - Causes of Underlying Pulmonary Hypertension
| Category | Examples |
|---|---|
| Obstructive lung disease | COPD (most common), bronchiectasis, asthma |
| Restrictive/interstitial lung disease | Pulmonary fibrosis, pneumoconioses, sarcoidosis |
| Pulmonary vascular disease | Pulmonary embolism (acute cor pulmonale), primary pulmonary arterial hypertension |
| Hypoventilation syndromes | Obesity-hypoventilation, OSA, neuromuscular disease, kyphoscoliosis |
| High altitude | Chronic hypoxia-induced vasoconstriction |
Pathophysiology
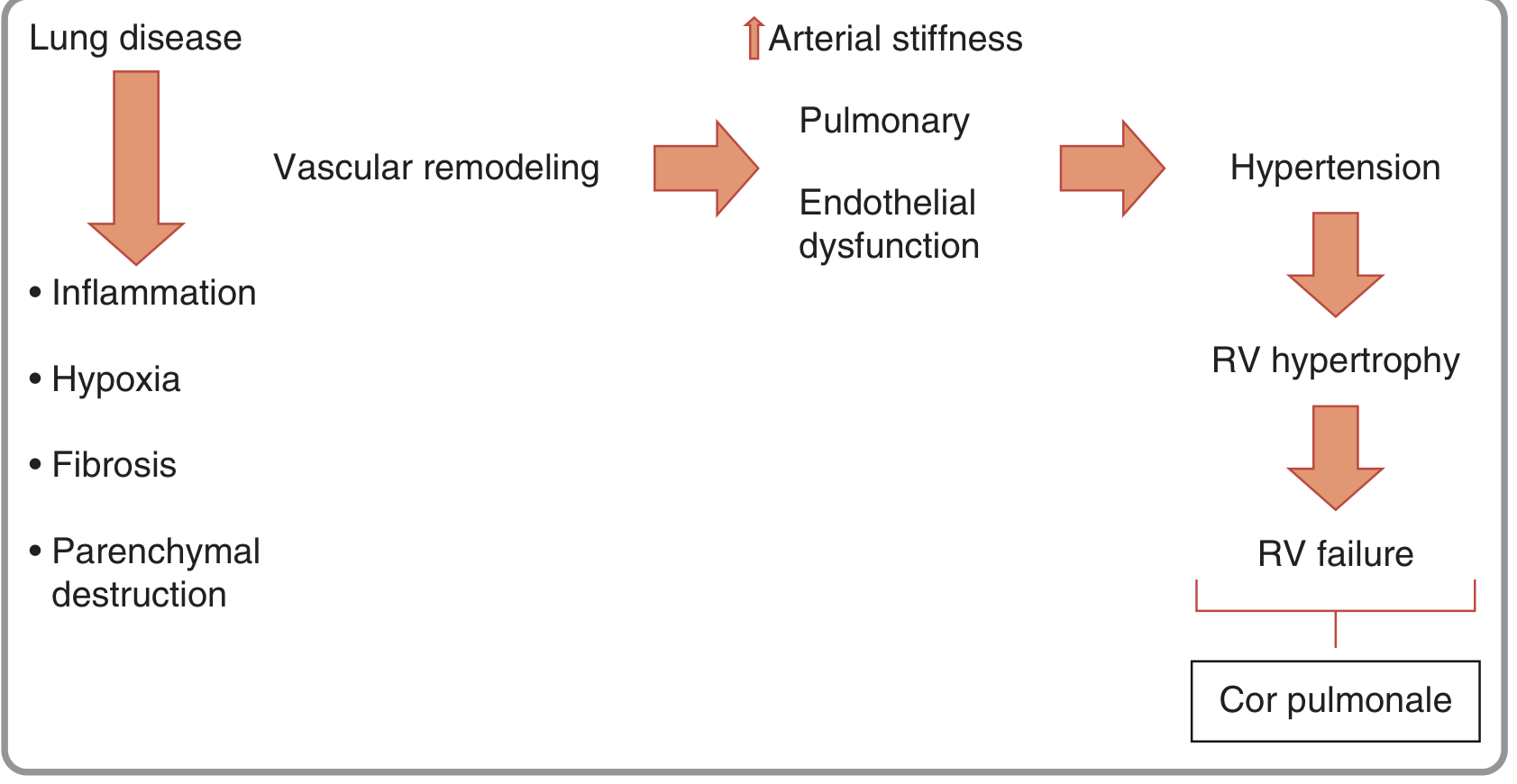
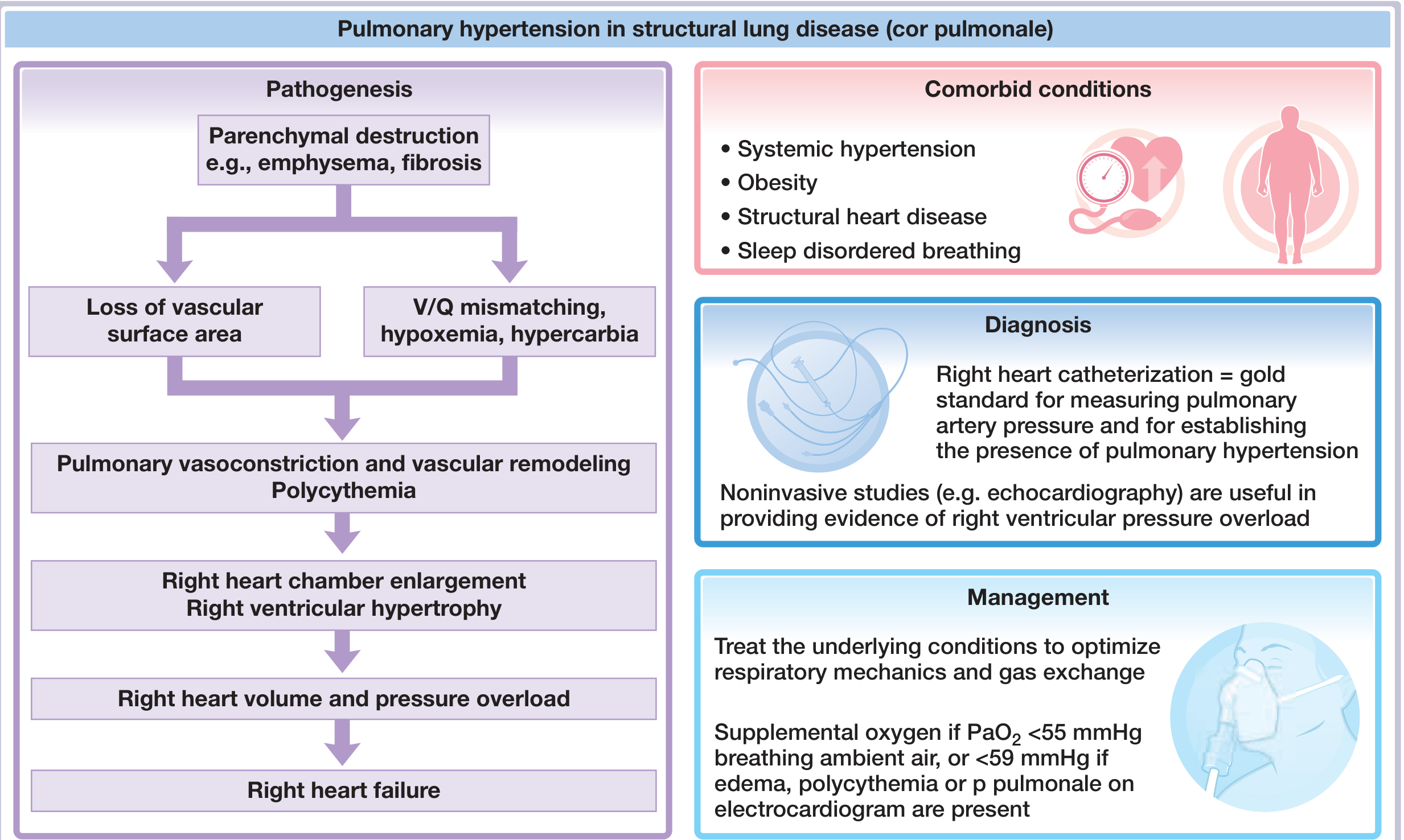
Key mechanisms raising pulmonary vascular resistance (PVR):
- Alveolar hypoxia (dominant driver) - acute hypoxia causes vasoconstriction of small muscular pulmonary arteries (50-100 μm); chronic hypoxia causes vascular stiffness and remodeling
- Loss of vascular cross-sectional area - destruction/obliteration from emphysema or fibrosis
- Endothelial dysfunction - reduced NO and prostacyclin (vasodilators) + increased endothelin (vasoconstrictor), promoting vascular remodeling
- Hypercapnia and acidosis - potentiates hypoxic vasoconstriction
- Polycythemia - secondary erythrocytosis from chronic hypoxia increases blood viscosity and PVR
- Hypervolemia and thromboembolism - contribute mechanically
- Vascular inflammation - CD8+ T-cell infiltration of pulmonary arterial walls, intimal thickening, smooth muscle proliferation
Morphology
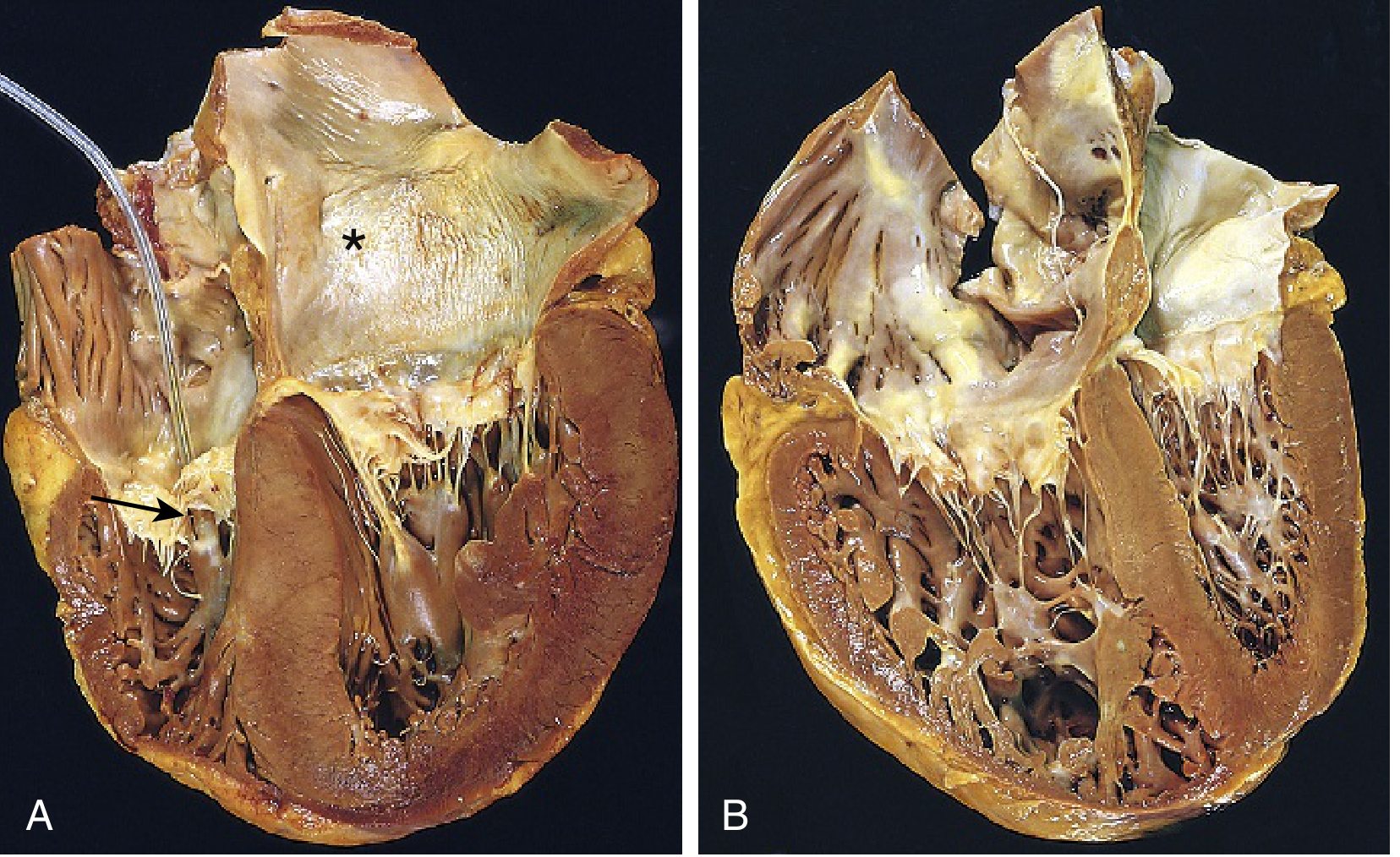
- Acute cor pulmonale (e.g., massive PE): right ventricle shows only dilation; may even be of normal size if sudden death occurs
- Chronic cor pulmonale: RV + often right atrial hypertrophy; in extreme cases the RV free wall thickness equals or exceeds that of the left ventricle; pulmonary arteries show abnormal intimal thickening
Clinical Features
- Dyspnea (progressive, exertional then at rest)
- Fatigue, reduced exercise tolerance
- Peripheral edema (ankle swelling)
- Syncope on exertion (in severe pulmonary hypertension)
- Jugular venous distension with prominent V wave (tricuspid regurgitation)
- Right ventricular heave (parasternal)
- Loud P2 (accentuated pulmonary component of S2)
- Graham Steell murmur - early diastolic murmur of pulmonary regurgitation (late finding)
- Hepatomegaly, ascites, peripheral edema (late - signs of RV volume overload)
- Cyanosis (from underlying lung disease and hypoxemia)
Why Edema Develops (Mechanism)
- Chronic hypercapnia → renal compensatory sodium and bicarbonate retention → fluid retention
- Reduced effective renal plasma flow → impaired urinary sodium excretion
- Activation of the renin-angiotensin-aldosterone system
Investigations
ECG
- P pulmonale - peaked P waves >2.5 mm in lead II (right atrial enlargement)
- Right axis deviation (QRS axis >+90°)
- R/S ratio >1 in V1 (RV hypertrophy)
- S1Q3T3 pattern (acute cor pulmonale from PE)
- Incomplete or complete right bundle branch block
- ST depression and T-wave inversion in right precordial leads (V1-V4)
Echocardiography
- Dilated RV with reduced RV function
- RV free wall hypertrophy (>5 mm)
- Paradoxical interventricular septal motion ("D-shape" of LV on short axis)
- Doppler estimation of pulmonary artery systolic pressure via tricuspid regurgitation jet velocity
- Note: Doppler-estimated PA pressure correlates poorly with direct catheter measurements in severe disease
Chest X-Ray
- Prominent pulmonary arteries (central pulmonary artery dilation)
- Cardiomegaly with right heart enlargement
- Oligaemic peripheral lung fields
- Evidence of underlying lung disease
Right Heart Catheterization (Gold Standard)
- Directly measures pulmonary artery pressure (mean PAP >20 mmHg = pulmonary hypertension)
- Pulmonary capillary wedge pressure normal (rules out left heart cause)
- Used when noninvasive studies are inconclusive
Additional
- Pulmonary function tests, ABG, CT pulmonary angiography (to exclude PE)
- Cardiac MRI: most accurate assessment of RV volumes and function
Management
Primary Approach: Treat the Underlying Lung Disease
- Optimize bronchodilators, inhaled corticosteroids for COPD/asthma
- CPAP/BiPAP for OSA or hypoventilation syndromes
- Nocturnal noninvasive ventilation in stable chronic hypercapnia (neuromuscular disease, kyphoscoliosis)
Long-Term Oxygen Therapy (LTOT) - Cornerstone
- Indications: PaO2 <55 mmHg on room air, OR PaO2 <59 mmHg if edema, polycythemia, or P pulmonale on ECG are present
- Reduces hypoxic vasoconstriction, lowers PVR, reduces polycythemia
- Goal: SaO2 ≥90%; use ≥15 hours/day
Diuretics
- Reduce volume overload and edema; optimize preload
- Monitor electrolytes carefully; avoid over-diuresis (RV is preload-dependent)
Vasodilators
- Calcium channel blockers and other vasodilators can dilate the pulmonary circulation but may worsen hypoxemia - benefit not established in secondary cor pulmonale
- PAH-specific agents (sildenafil, endothelin receptor antagonists, prostacyclins) are used in idiopathic PAH but evidence is limited in cor pulmonale from structural lung disease
Polycythemia
- Traditionally treated with phlebotomy; recent cohort data suggest polycythemia is less common than expected and has uncertain effect on outcomes
- Hematocrit kept <55% if polycythemia present
Prognosis
- Once cor pulmonale is established, survival is significantly diminished
- If mean pulmonary artery pressure exceeds 25 mmHg, average 5-year survival is reduced by 50%