Arteria blood gas
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, textbook-sourced reference on Arterial Blood Gas (ABG) analysis.
Arterial Blood Gas (ABG) Analysis
What It Measures
An ABG directly measures the following from an arterial blood sample (gold standard):
| Variable | Normal Value | Reference Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO2 | 40 mmHg | 35 - 45 mmHg |
| PaO2 | 100 mmHg | 75 - 100 mmHg |
| HCO3- | 24 mEq/L | 22 - 26 mEq/L |
| Base Excess | 0 | -4 to +4 |
pH and PO2/PCO2 are measured directly via electrodes; HCO3-, O2 saturation, and base excess are calculated (via the Henderson-Hasselbalch equation).
"Analysis of arterial blood gases... is based primarily on determination of PaO2, PaCO2, and pH. As a rule, these parameters are measured directly. Other values, including O2 saturation, bicarbonate concentration, and base excess (or deficit), are usually calculated." - Fishman's Pulmonary Diseases and Disorders
Sampling Technique
Preferred site: Radial artery - superficial, easy to compress for hemostasis, no large veins nearby, and the ulnar artery provides collateral circulation in case of thrombosis.
Other sites: brachial and femoral arteries.
Key technical points:
- Blood is drawn anaerobically into heparin-coated syringes
- Air bubbles artificially raise PO2 and lower PCO2
- The sample must be analyzed immediately or kept on ice; if left at 37°C, over 10 minutes: pH falls ~0.01, PCO2 rises ~1 mmHg, O2 content falls
- Local anesthetic (lidocaine) minimizes the hyperventilatory response to pain/anxiety during puncture
Clinical Information Obtained
- Oxygenation - PaO2 is the gold standard; allows calculation of the alveolar-arterial oxygen gradient (A-a gradient)
- Ventilation - PaCO2 reflects alveolar ventilation directly
- Acid-base balance - pH + HCO3- together classify acid-base disorders
- Hypercapnia type - Distinguishes acute vs. chronic CO2 retention
- Cause of hypercapnia - A-a gradient helps separate lung disease from pump failure
Stepwise ABG Interpretation
(Current Surgical Therapy, 14th ed.)
Step 1 - Assess pH
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
Step 2 - Assess PaCO2
- In respiratory disorders, PaCO2 moves opposite to pH
- In metabolic disorders, PaCO2 moves in the same direction as pH (compensation)
Step 3 - Assess HCO3-
- Low HCO3- = metabolic acidosis
- High HCO3- = metabolic alkalosis
Step 4 - Assess Base Excess (BE)
- BE is the amount of base needed to titrate 1 L of blood to pH 7.4 at 37°C
- BE > +4 = alkalosis; BE < -4 (base deficit) = acidosis
- Represents the pure metabolic component
Step 5 - Assess PaO2
- Hypoxemia may coexist with or cause acid-base disorders and must not be overlooked
Acid-Base Disorders and Compensation Formulas
(Current Surgical Therapy, 14th ed.)
| Disorder | Key Finding | Expected Compensation |
|---|---|---|
| Metabolic acidosis | Low pH, Low HCO3- | PaCO2 = 1.5 × [HCO3-] + 8 ± 2 (Winter's formula) |
| Metabolic alkalosis | High pH, High HCO3- | PaCO2 = 0.7 × [HCO3-] + 20 ± 5 |
| Acute respiratory acidosis | Low pH, High PaCO2 | ↑ HCO3- = ΔPaCO2 / 10 |
| Chronic respiratory acidosis | Near-normal pH, High PaCO2 | ↑ HCO3- = 4 × (ΔPaCO2 / 10) |
| Acute respiratory alkalosis | High pH, Low PaCO2 | ↓ HCO3- = 2 × (ΔPaCO2 / 10) |
| Chronic respiratory alkalosis | Near-normal pH, Low PaCO2 | ↓ HCO3- = 5 × (ΔPaCO2 / 10) |
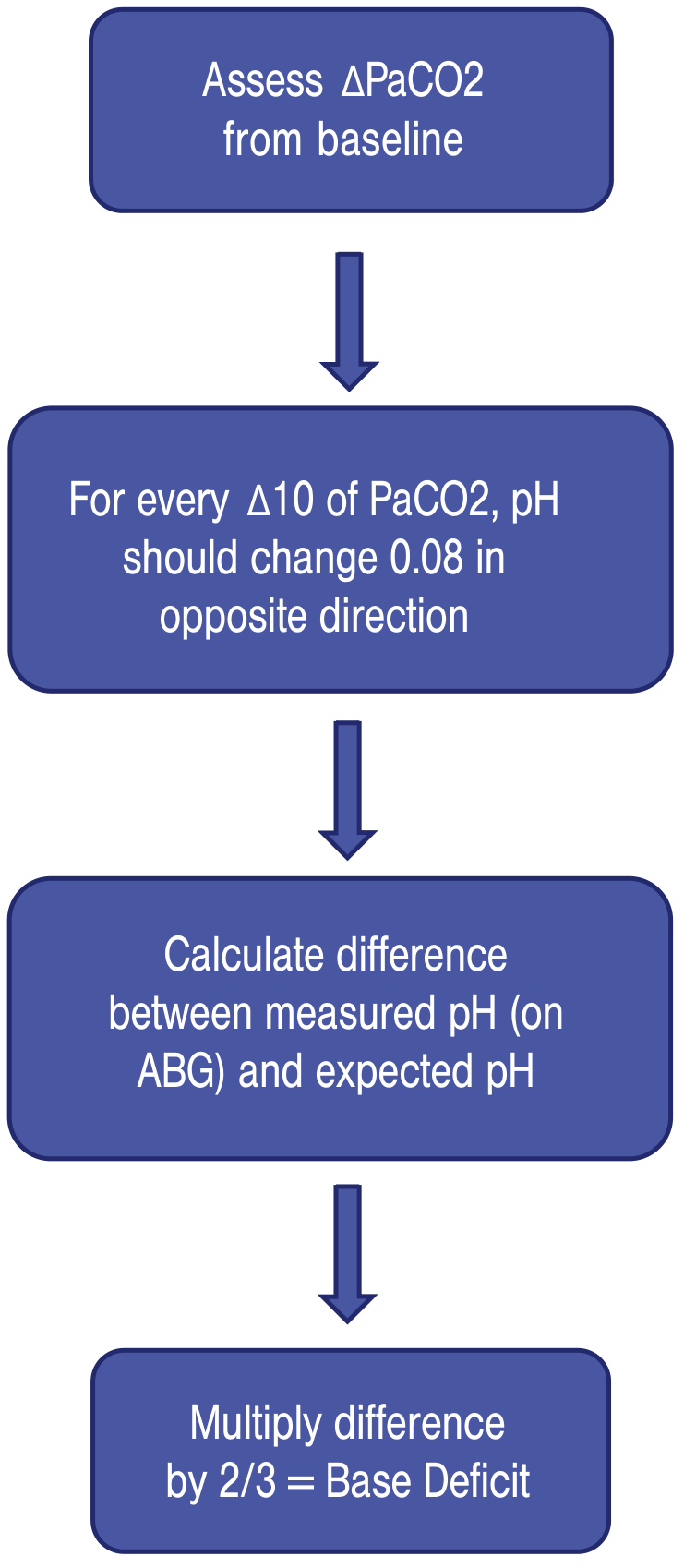
Acute hypercapnia rule: For every 10 mmHg rise in PaCO2, pH falls by 0.08 and HCO3- rises by ~1 mEq/L.
Chronic hypercapnia rule: For every 10 mmHg rise in PaCO2, HCO3- rises by 3.5-5 mEq/L (renal compensation over 3-5 days).
Primary Respiratory Disorders (Fishman's Classification)
| Disorder | PaCO2 | pH |
|---|---|---|
| Acute respiratory alkalosis | < 36 mmHg | > 7.44 |
| Chronic respiratory alkalosis | < 36 mmHg | Normal (renal compensation, HCO3- < 19) |
| Acute respiratory acidosis | > 44 mmHg | < 7.36 |
| Chronic respiratory acidosis | > 44 mmHg | Normal (renal compensation, HCO3- > 30) |
Alveolar-Arterial (A-a) Oxygen Gradient
- Normal A-a gradient: ~10 mmHg (increases slightly with age)
- A-a gradient > 20 mmHg: Suggests underlying lung disease contributing to hypercapnia
- Normal A-a gradient with hypercapnia: Suggests depressed central drive or neuromuscular failure (pump problem, not lung problem)
- Formula: A-a gradient = PAO2 - PaO2
ABG vs. Venous Blood Gas (VBG)
(Tintinalli's Emergency Medicine)
- VBG pH correlates closely with ABG (difference ±0.05 units) - clinically acceptable for most scenarios
- VBG PCO2 trends with ABG but can vary up to ±20 mmHg - not reliably substitutable for arterial CO2
- VBG PO2 does not correlate with arterial oxygenation and cannot be used to assess hypoxemia
PaO2 Age Correction
PaO2 decreases predictably with age:
PaO2 = 109 - 0.43 × (age in years) ± 4.1 mmHg - Fishman's Pulmonary Diseases and Disorders
It also decreases with altitude (by ~20 mmHg at 1,500 m elevation, e.g., Denver) and with the supine position.
ABG vs. Pulse Oximetry
- Pulse oximetry measures saturation, not partial pressure - it is insensitive to PaO2 changes above 60 mmHg (flat part of the oxyhemoglobin dissociation curve)
- It cannot detect hypoventilation in patients receiving supplemental oxygen (the most important clinical limitation)
- It is fooled by: carboxyhemoglobin, methemoglobin, methylene blue, dark nail polish, poor perfusion, and dark skin pigmentation (tends to overestimate SpO2 in Black individuals)
- ABG remains necessary when precise assessment of PaO2, PCO2, or pH is required
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Tintinalli's Emergency Medicine | Current Surgical Therapy, 14th ed.
This is a shared conversation. Sign in to Orris to start your own chat.