
Kindly explain this question for dnb answer taking reference from Williams Obs and recent guidelines uski g simple flow charts and diagrams
"obstructed labour" AND "caesarean section" AND complications
"obstructed labor" AND "cesarean" AND complications
"cesarean section" AND "uterine extension" AND prevention
"cesarean delivery" AND "obstructed labor" AND morbidity
caesarean section obstructed labour complications prevention management Williams Obstetrics 26th edition
https://nursing.ceconnection.com/ovidfiles/00005721-20200300…
CS obstructed labour Bandl ring uterine rupture lower segment complications management RCOG ACOG guidelines
Medical flowchart titled "Complications of Caesarean Section in Obstructed Labour" showing two main columns: INTRAOPERATIVE COMPLICATIONS (left side, red/orange boxes) and POSTOPERATIVE COMPLICATIONS (right side, blue boxes). Intraoperative: 1. Haemorrhage - PPH due to atonic/traumatic uterus, uterine incision extensions, broad ligament haematoma; 2. Difficult fetal extraction - deeply engaged/impacted head, Bandl's ring; 3. Uterine injuries - extension of uterine incision, uterine rupture; 4. Bladder/ureter injury - especially with oedematous lower segment; 5. Bowel injury - adhesions; 6. Anaesthetic complications - failed intubation, aspiration; 7. Amniotic fluid embolism. Postoperative: 1. Haemorrhage - PPH; 2. Wound infection/dehiscence; 3. Endomyometritis; 4. UTI; 5. DVT/Pulmonary embolism; 6. Sepsis; 7. Paralytic ileus; 8. Vesico-vaginal fistula; 9. Neonatal asphyxia. Clean professional medical diagram style with color coding, arrows, and boxes.
Medical flowchart diagram titled "Management of Complications - CS in Obstructed Labour" with three sections. Section 1 (top, green): PREVENTION BEFORE SURGERY - Resuscitate patient (IV fluids, blood, correct anaemia), Decompress bladder (Foley catheter), Antibiotic prophylaxis (Cefazolin 1-2g IV), Choose experienced surgeon, Choose correct incision, Use tocolytics if Bandl's ring present (GTN sublingual/terbutaline). Section 2 (middle, orange): INTRAOPERATIVE MANAGEMENT - Difficult head: push up vaginally (Patwardhan/Classical method), Hemorrhage: bimanual compression → uterotonics → B-Lynch suture → hysterectomy, Bladder injury: immediate repair + catheter 7 days, Uterine extension: repair in layers. Section 3 (bottom, blue): POSTOPERATIVE MANAGEMENT - PPH protocol (Oxytocin, Misoprostol, TXA), Sepsis: broad spectrum antibiotics (Clindamycin + Gentamicin), DVT prophylaxis: LMWH, Wound care, VTE: heparinisation. Professional clean medical flowchart with arrows and color-coded boxes.
Medical diagram showing Bandl's Pathological Retraction Ring in obstructed labour. Anatomical illustration of the uterus showing: Upper uterine segment (thickened, retracted, labeled in red), Bandl's ring (visible constriction ring at junction, labeled with arrow, shown as a visible transverse groove), Lower uterine segment (thin, over-distended, labeled in blue), Fetal head impacted in pelvis below. Caption text: "Bandl's Ring = Junction of Upper & Lower Uterine Segment. Forms at umbilicus level. Indicates impending uterine rupture. Management: Emergency CS + IV Tocolytics (GTN/Terbutaline)". Clean anatomical diagram style, educational medical illustration.
Caesarean Section in Obstructed Labour - DNB Answer (April 2023) [2+3+5 Marks]
WHY OBSTRUCTED LABOUR MAKES CS HIGH-RISK
- Lower uterine segment is thin, oedematous, and friable
- Bladder is pulled up and adherent to the lower segment
- Fetal head is deeply impacted in the pelvis
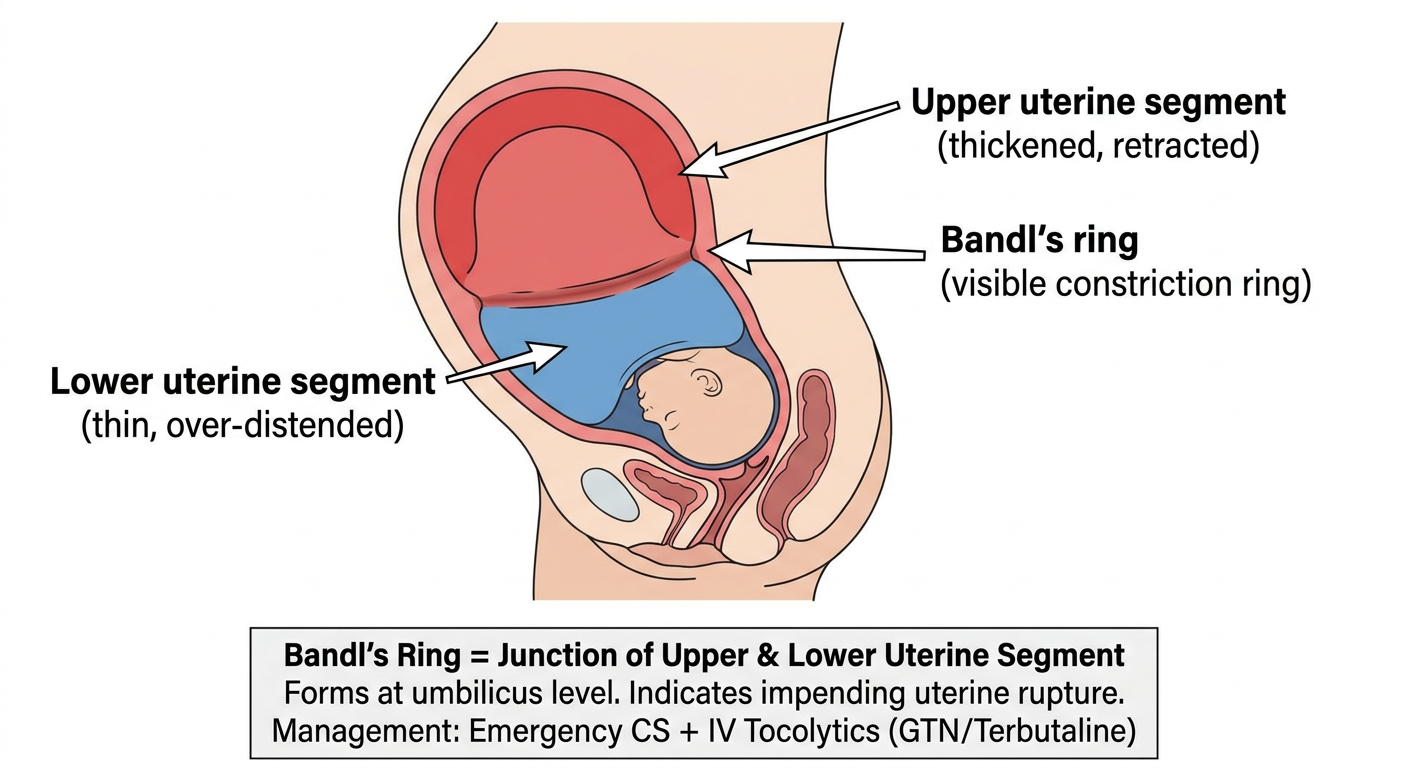
- Bandl's pathological retraction ring may be present
- Tissues are infected, hypoxic, and friable after prolonged labour
a) COMPLICATIONS OF CS IN OBSTRUCTED LABOUR (2 Marks)
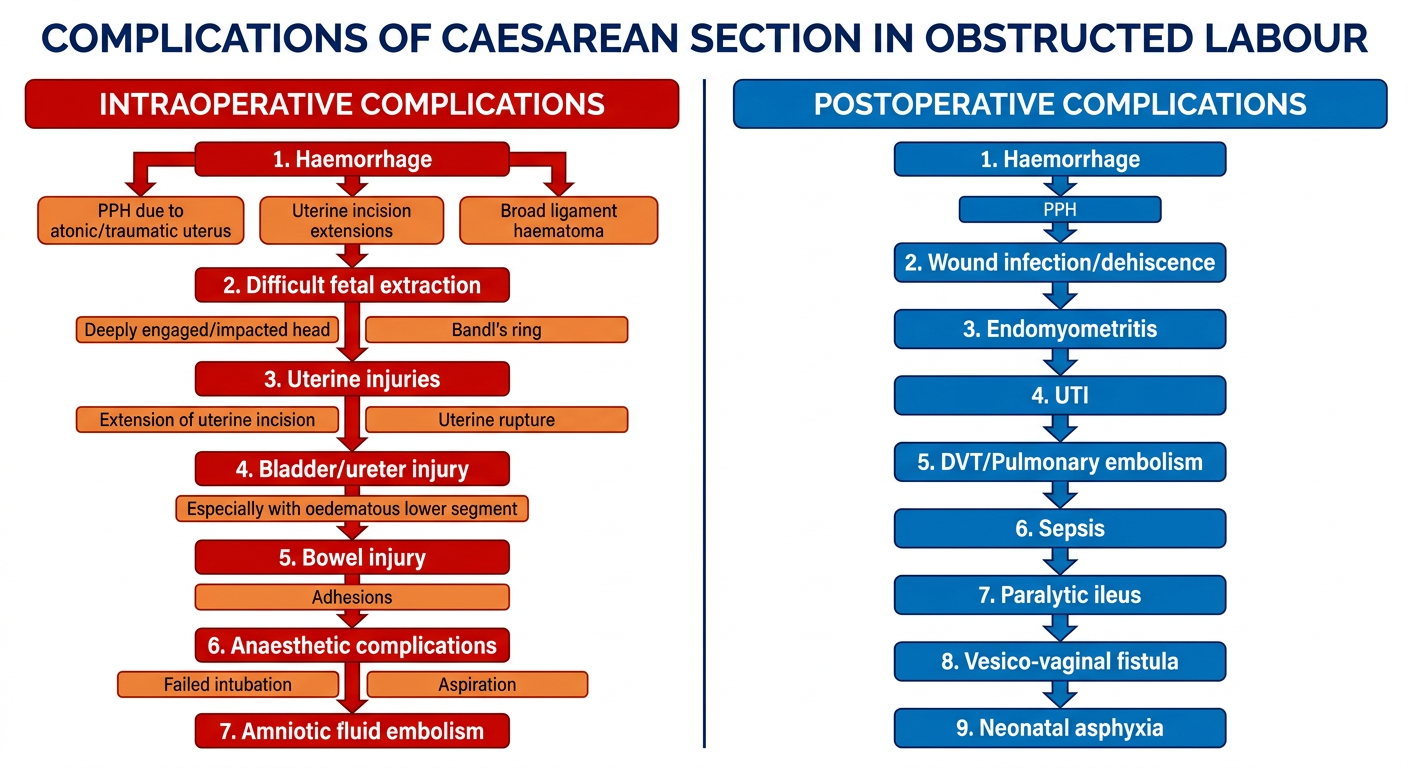
INTRAOPERATIVE COMPLICATIONS
| Category | Specific Complication |
|---|---|
| Haemorrhage | PPH due to uterine atony (most common), lateral extensions of uterine incision into uterine vessels, broad ligament haematoma |
| Difficult fetal extraction | Deeply impacted fetal head (stuck at the pelvic brim), Bandl's ring trapping the fetus |
| Uterine injuries | Lateral extensions of uterine incision (T or J extensions), uterine rupture if Bandl's ring is ignored |
| Bladder injury | Bladder pulled up due to prolonged obstruction; incidence ~1-2/1000 (10x higher than vaginal delivery) - Williams Obs Ch 30 |
| Ureteric injury | While dissecting oedematous bladder flap |
| Bowel injury | Rare; associated with adhesions |
| Anaesthetic complications | Failed intubation, pulmonary aspiration (Mendelson syndrome), drug reactions |
| Amniotic fluid embolism | Rare but life-threatening |
| Air embolism | Rare |
POSTOPERATIVE COMPLICATIONS
| Category | Specific Complication |
|---|---|
| Haemorrhage | Primary/secondary PPH |
| Sepsis / Endomyometritis | Polymicrobial; fever, uterine tenderness, malodorous lochia - already bacterially contaminated before CS |
| Wound complications | Infection (3%), dehiscence, haematoma, necrotising fasciitis |
| UTI | ~11% post-CS (related to catheterisation) |
| DVT/PE | DVT 1-2%; PE is a leading cause of maternal death - Williams Obs Ch 30 |
| Paralytic ileus | Adynamic ileus; rarely Ogilvie syndrome |
| Vesico-vaginal fistula (VVF) | From pressure necrosis of bladder - major complication of prolonged obstructed labour |
| Neonatal asphyxia | Fetal compromise from prolonged obstruction |
| Atelectasis / Pneumonia | Pulmonary complications post-anaesthesia |
| Anaemia | From intraoperative blood loss |
b) PREVENTIVE MEASURES (3 Marks)
PRE-OPERATIVE PREVENTION
- IV access x2; send blood for CBC, group & crossmatch
- Correct hypovolaemia: Ringer's Lactate/Normal Saline, blood transfusion if Hb <8 g/dL
- Correct electrolyte imbalance (dehydration is universal in obstructed labour)
- Nasogastric tube + antacid (0.3M sodium citrate 30 mL) to reduce aspiration risk
- Ensure Foley catheter is draining freely before starting
- Empty bladder completely - reduces bladder injury risk
- Cefazolin 2g IV at time of skin incision (ACOG/RCOG recommendation)
- OR if allergic: Clindamycin 600mg + Gentamicin 1.5mg/kg IV
- Azithromycin 500mg IV added for non-elective CS (Tita et al. - reduces endometritis significantly)
- Vaginal cleansing with 10% povidone-iodine before CS (Cochrane review, 2635 women: reduces SSI)
- Experienced anaesthetist mandatory
- Spinal anaesthesia preferred (avoids failed intubation risk)
- If GA needed: rapid sequence induction (RSI) with cricoid pressure
- Pre-oxygenation for 3-5 min before induction
- Left lateral tilt (15°) to avoid aortocaval compression
- Senior/experienced surgeon to perform the CS
- Do not delegate to a junior - obstructed labour CS is high risk
- If Bandl's ring identified: give IV/sublingual GTN (glyceryl trinitrate) OR terbutaline SC for uterine relaxation before/during extraction
- Tocolysis allows safe extraction without rupture (Queensland Clinical Guidelines 2025)
INTRAOPERATIVE PREVENTION
- Pfannenstiel incision is standard
- If previous scars/adhesions: Pfannenstiel with care OR midline (better exposure)
- Uterine incision: low transverse (Joel-Cohen modification preferred - less blood loss)
- Push bladder down carefully with a wet swab - do NOT cut hastily
- Identify bladder boundaries before making uterine incision
- Keep bladder retractor in position throughout
HEAD DEEPLY IMPACTED - APPROACH:
|
┌───────────┴───────────┐
PUSH technique PULL technique
(Assistant pushes head (Patwardhan method,
up from below vaginally) Classical incision if needed)
| |
Wrigley's forceps Reverse breech extraction
after disimpaction (feet first via fundal
pressure / incision)
- Use vacuum extractor or Wrigley's forceps gently after disimpacting the head
- Patwardhan's technique: deliver shoulders first, then head (for deeply engaged head)
- Consider classical (vertical) uterine incision if lower segment is poorly formed or Bandl's ring present
- AVOID fundal pressure without proper disimpaction - can cause uterine rupture
- Active management of third stage: Oxytocin 10 IU IV immediately after delivery
- Uterine massage
- Check for lateral extensions of incision before closing
- TED stockings intraoperatively
- LMWH (Enoxaparin 40mg SC) from 6-12 hours post-op (RCOG guidelines)
- Early mobilisation
c) MANAGEMENT OF COMPLICATIONS (5 Marks)
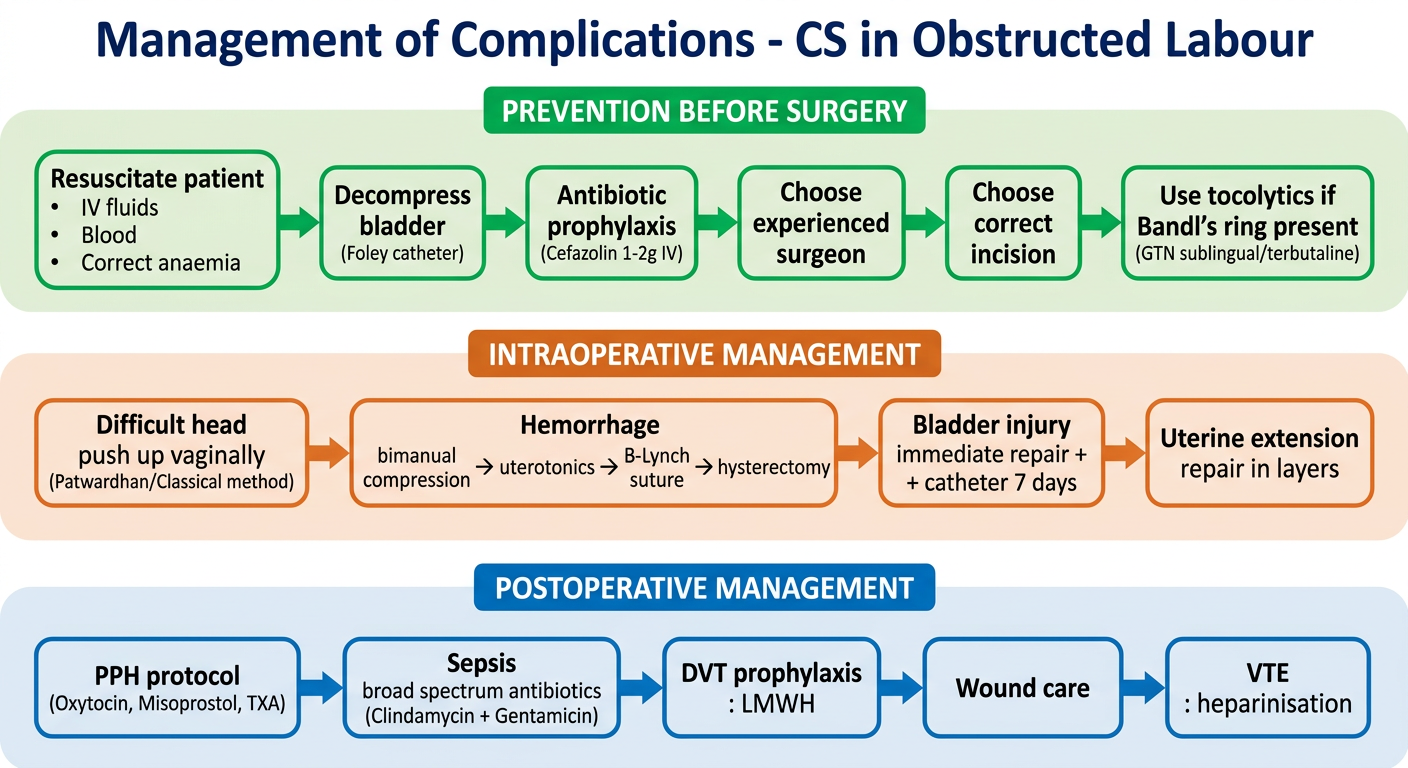
1. POSTPARTUM HAEMORRHAGE (PPH)
STEP 1: Bimanual uterine compression + Oxytocin 10-20 IU IV infusion
+Ergometrine 0.5mg IM (avoid in hypertension)
+Misoprostol 800 mcg sublingual/rectal
+Carboprost 0.25mg IM every 15 min (max 8 doses)
+Tranexamic acid (TXA) 1g IV within 3 hours of PPH onset
+IV fluids / Blood transfusion
↓
STEP 2: Surgical - Uterine compression sutures
B-Lynch suture / Hayman suture / Cho sutures (squeezing sutures)
↓
STEP 3: Uterine artery ligation (O'Leary stitch)
Internal iliac artery ligation
↓
STEP 4: Peripartum hysterectomy (life-saving - do not delay)
- TXA 1g IV is now first-line early adjunct - [WOMAN Trial 2017, PMID 28456509]: reduces death from bleeding by 31% if given within 3 hours
2. DIFFICULT FETAL EXTRACTION / IMPACTED HEAD
| Technique | When to Use |
|---|---|
| Vaginal disimpaction (reverse pressure) | Flex and push head up from vagina by assistant |
| Patwardhan's technique | Shoulder delivery first, then head extracted from below |
| Classical (vertical) uterine incision | When lower segment poorly formed (e.g. preterm, Bandl's ring) |
| Reverse breech extraction | Pull legs through fundal incision |
| Tocolysis (GTN sublingual) | Bandl's ring - pharmacological relaxation |
| Wrigley's/Neville Barnes forceps | Once head is partially accessible in incision |
3. UTERINE INCISION EXTENSION / RUPTURE
- Identify extension early (inspect all edges)
- Repair with delayed absorbable suture (Vicryl/PDS) in 1-2 layers
- For lateral extension into uterine vessels: figure-of-8 sutures, identify and ligate vessels
- Uterine rupture with uncontrolled haemorrhage or extensive damage: Subtotal/total hysterectomy
- Check bladder and ureter integrity after any lateral extension
4. BLADDER INJURY
- Recognised intraoperatively: immediate two-layer repair with 3-0 Vicryl (submucosa + muscularis)
- Foley catheter for 10-14 days postoperatively
- Cystogram before catheter removal to confirm healing
- Ureteric injury: consult urology; ureteric stenting or reimplantation
5. ENDOMYOMETRITIS / SEPSIS
- Most common postoperative complication in obstructed labour
- Treatment: Clindamycin 900mg IV 8-hourly + Gentamicin 1.5mg/kg IV 8-hourly (Creasy & Resnik; French & Smaill systematic review)
- This combination superior to all others (covers penicillin-resistant anaerobes)
- Oral follow-up antibiotics NOT needed once clinical improvement occurs
- If pelvic thrombophlebitis suspected (fever not responding to antibiotics): add IV Heparin - dramatic improvement confirms diagnosis
6. WOUND COMPLICATIONS
| Complication | Management |
|---|---|
| Wound haematoma | Drainage, pressure dressing |
| Wound infection | Wound opening, debridement, secondary closure after 72h of antibiotics |
| Wound dehiscence | Mechanical closure, secondary suturing |
| Necrotising fasciitis | Emergency surgical debridement + broad-spectrum IV antibiotics + ICU; high mortality |
7. DVT / PULMONARY EMBOLISM
- DVT: LMWH (Enoxaparin 1mg/kg BD) + compression stockings + anticoagulate 6 weeks
- PE: If haemodynamically stable: heparinisation; if unstable: consider thrombolysis or surgical embolectomy
- RCOG recommends risk stratification and thromboprophylaxis for all CS patients
8. PARALYTIC ILEUS
- NBM, nasogastric aspiration, IV fluids, electrolyte correction
- Neostigmine 2.5mg IV for Ogilvie syndrome (colonic pseudo-obstruction)
- Early mobilisation, chewing gum post-op (reduces ileus duration - meta-analysis evidence)
9. NEONATAL ASPHYXIA
- Senior neonatologist/paediatrician present at delivery
- Neonatal resuscitation: warm, dry, stimulate, suction, bag-mask ventilation, intubation
- APGAR at 1 and 5 minutes; cord blood gases
- Transfer to NICU if needed
SUMMARY TABLE (Quick Revision)
| Complication | Key Prevention | Key Management |
|---|---|---|
| PPH | Oxytocin at delivery, repair extensions | Step-up: uterotonics → B-Lynch → hysterectomy + TXA |
| Impacted head | Experienced surgeon, tocolysis | Patwardhan/disimpact/classical incision |
| Bladder injury | Push bladder down carefully | 2-layer repair + catheter 10-14 days |
| Infection | Antibiotic prophylaxis, vaginal prep | Clindamycin + Gentamicin IV |
| DVT/PE | LMWH, TED stockings | Heparinisation, anticoagulate |
| Uterine rupture | Avoid fundal pressure, tocolysis for Bandl's | Repair or hysterectomy |
KEY REFERENCES
- Williams Obstetrics 26th Ed, Ch. 23 (Abnormal Labour), Ch. 30 (Caesarean Delivery), Ch. 33 (Term Newborn)
- Creasy & Resnik's Maternal-Fetal Medicine, Complications of Cesarean Delivery (p. 960)
- RCOG Green Top Guideline No. 45 (Birth After Previous CS)
- Queensland Clinical Guidelines: Obstructed Labour and Impacted Fetal Head (2025)
- WOMAN Trial (2017) - Tranexamic acid in PPH [PMID: 28456509]
- French & Smaill Cochrane Review - Antibiotic regimens for endometritis post-CS
Kindly explain obstructed labour and it’s management and complications -Kindly explain this question for dnb answer taking reference from Williams Obs and recent guidelines uski g simple flow charts and diagrams
"obstructed labor" AND management AND complications
obstructed labour definition causes diagnosis management Williams Obstetrics chapter 23 abnormal labour
"obstructed labor" AND "maternal morbidity" AND "uterine rupture"
obstructed labour partograph signs symptoms maternal fetal complications management WHO guidelines 2025
https://qme.csds.qld.edu.au/wp-content/uploads/sites/3/2025/…
Medical educational diagram titled "CAUSES OF OBSTRUCTED LABOUR - The 3 Ps" showing three main color-coded columns with icons. Column 1 (red, labeled PASSENGER): Fetal macrosomia (>4 kg), Malpresentation - Brow presentation, Face presentation (mento-posterior), Shoulder presentation/Transverse lie, Hydrocephalus, Locked twins, Conjoined twins. Column 2 (blue, labeled PASSAGE): Bony pelvis - Contracted inlet (AP diameter <10 cm), Contracted midpelvis (interspinous <9 cm), Outlet contraction; Soft tissue - Cervical stenosis/fibroids/ovarian tumour, Pelvic tumours (fibroid/ovarian cyst), Vaginal stenosis/FGM, Full rectum/bladder. Column 3 (orange, labeled POWER - Contributory): Uterine inertia/hypotonic contractions, Incoordinate uterine action. Bottom note: "Power alone does NOT cause obstruction - mechanical block required". Clean professional medical diagram with arrows pointing to central box "OBSTRUCTED LABOUR"
Medical educational diagram titled "CLINICAL FEATURES OF OBSTRUCTED LABOUR" divided into two sections. Left section "MATERNAL SIGNS" (red boxes): 1. General - Maternal exhaustion, dehydration, anxiety, tachycardia, fever; 2. Abdomen - Bandl's pathological retraction ring visible (transverse groove at umbilicus level), distended lower uterine segment thin and tender, uterine tenderness, round ligaments taut and palpable, haematuria; 3. Vagina/Cervix - Oedematous cervix, oedematous vulva and vagina, caput and moulding, impacted presenting part, no progress on partograph. Right section "FETAL SIGNS" (blue boxes): Fetal tachycardia, Meconium-stained liquor, Late decelerations on CTG, Absent fetal movements - fetal distress. Bottom warning box in red: "IMPENDING UTERINE RUPTURE - Bandl's ring + Constant abdominal pain + Tachycardia = EMERGENCY CS". Professional clean medical diagram.
Medical diagram showing a Partograph/Partogram for obstructed labour. The graph shows cervical dilatation (y-axis 0-10 cm) against time in hours (x-axis 0-12 hours). Shows: a normal labor curve (green) progressing steadily; Alert line (diagonal yellow line from 4cm at 0 hours to 10cm at 6 hours); Action line (diagonal red line 4 hours to the right of alert line). A plotted patient curve (orange) that starts normal, crosses the alert line, then the action line, showing arrested progress (flat line) at 6cm for 4+ hours = OBSTRUCTED LABOUR. Additional panels showing: caput succedaneum grading (1+ to 3+), moulding grading (0 to 3+), fetal heart rate panel below. Caption: "When cervical dilation CROSSES the ACTION LINE with adequate contractions = Obstructed Labour. Action required immediately." Professional obstetric educational partograph style diagram.
Medical flowchart titled "MANAGEMENT OF OBSTRUCTED LABOUR" with sequential steps and decision boxes. Step 1 (green box): IMMEDIATE RESUSCITATION - IV access x2, IV fluids (RL/NS 1 litre fast), Blood: CBC, cross-match, coagulation, Urinary catheter (monitor output + note haematuria), O2 by face mask, NPO + antacid (sodium citrate), Antibiotics: Ampicillin + Metronidazole IV. Step 2 (orange box): ASSESS CAUSE - Vaginal examination: check presentation, position, station, CPD, Check fetal heart rate/CTG, Senior obstetrician evaluation. Step 3 (blue decision diamond): FETAL ALIVE OR DEAD? Branch 1 (ALIVE, left): Emergency Caesarean Section - most cases; Assisted vaginal delivery (only if criteria met: fully dilated, no CPD, head at outlet). Branch 2 (DEAD FETUS, right): Destructive procedures - Craniotomy (hydrocephalus/deeply impacted head), Decapitation (impacted shoulder), Evisceration (abdominal tumour). Step 4 (purple box): POST-DELIVERY CARE - Active management 3rd stage (Oxytocin 10IU), Check for PPH, Repair all lacerations, Antibiotics continued 5-7 days, Bladder catheter if haematuria (prevent fistula), NICU for baby. Professional clean medical decision flowchart with color coded boxes and arrows.
Medical diagram titled "COMPLICATIONS OF OBSTRUCTED LABOUR" showing two large panels side by side. Left panel "MATERNAL COMPLICATIONS" (red theme) subdivided: Immediate - Uterine rupture (most dangerous), PPH/Haemorrhage, Sepsis/Chorioamnionitis, Shock (hypovolaemic/septic), Bladder/rectal injury; Short-term - Endomyometritis, Wound infection post-CS, UTI, DVT/PE, Anaemia; Long-term - Obstetric fistula (VVF/RVF) from pressure necrosis, Pelvic floor injury/prolapse, Urinary/faecal incontinence, Foot drop (common peroneal nerve compression), Secondary infertility, Psychological trauma/PTSD. Right panel "FETAL/NEONATAL COMPLICATIONS" (blue theme): Birth asphyxia (HIE), Stillbirth/perinatal death, Caput succedaneum, Skull fracture/cephalhaematoma, Intracranial haemorrhage, Meconium aspiration syndrome, Neonatal sepsis, Brachial plexus injury. Bottom box: "OBSTETRIC FISTULA - Results from prolonged pressure of fetal head on bladder/rectum → ischaemic necrosis → VVF or RVF". Professional clean medical educational diagram.
Medical anatomical diagram showing "Bandl's Pathological Retraction Ring" - cross-sectional view of pregnant uterus in obstructed labour. Shows: Upper uterine segment (thick, bunched up, retracted, labeled in red with arrow). Bandl's retraction ring - visible groove/constriction band at junction of upper and lower segment at umbilicus level (labeled with prominent red arrow). Lower uterine segment (thin, over-stretched, ballooned, translucent appearance, labeled in orange). Fetal head deeply impacted in pelvis. Round ligaments (taut, visible, labeled). Bladder displaced upward (labeled in blue). Inset diagram showing the "hourglass" shape of the uterus. Caption text boxes: "Bandl's ring = PATHOLOGICAL retraction ring", "Normal retraction ring = physiological", "Bandl's at umbilicus = impending rupture", "TREAT AS EMERGENCY: IV Tocolytic (GTN 0.4mg SL) + Emergency CS". Educational anatomical illustration style.
OBSTRUCTED LABOUR
DNB Answer - Williams Obstetrics (Ch. 23), Recent Guidelines
DEFINITION
Williams Obstetrics Ch. 23: "Dystocia literally means difficult labour and is characterised by abnormally slow labour progress."
- Active phase of labour > 12 hours = prolonged labour (which, if unrelieved, becomes obstructed)
- Key distinction: Power alone does NOT cause obstruction - there must be a mechanical block
INCIDENCE
- Affects 3-6% of all labours globally
- Leading cause of maternal death in developing countries - contributes to >70% of maternal deaths as a contributing factor
- Most common cause of obstetric fistula worldwide
CAUSES - THE 3 Ps
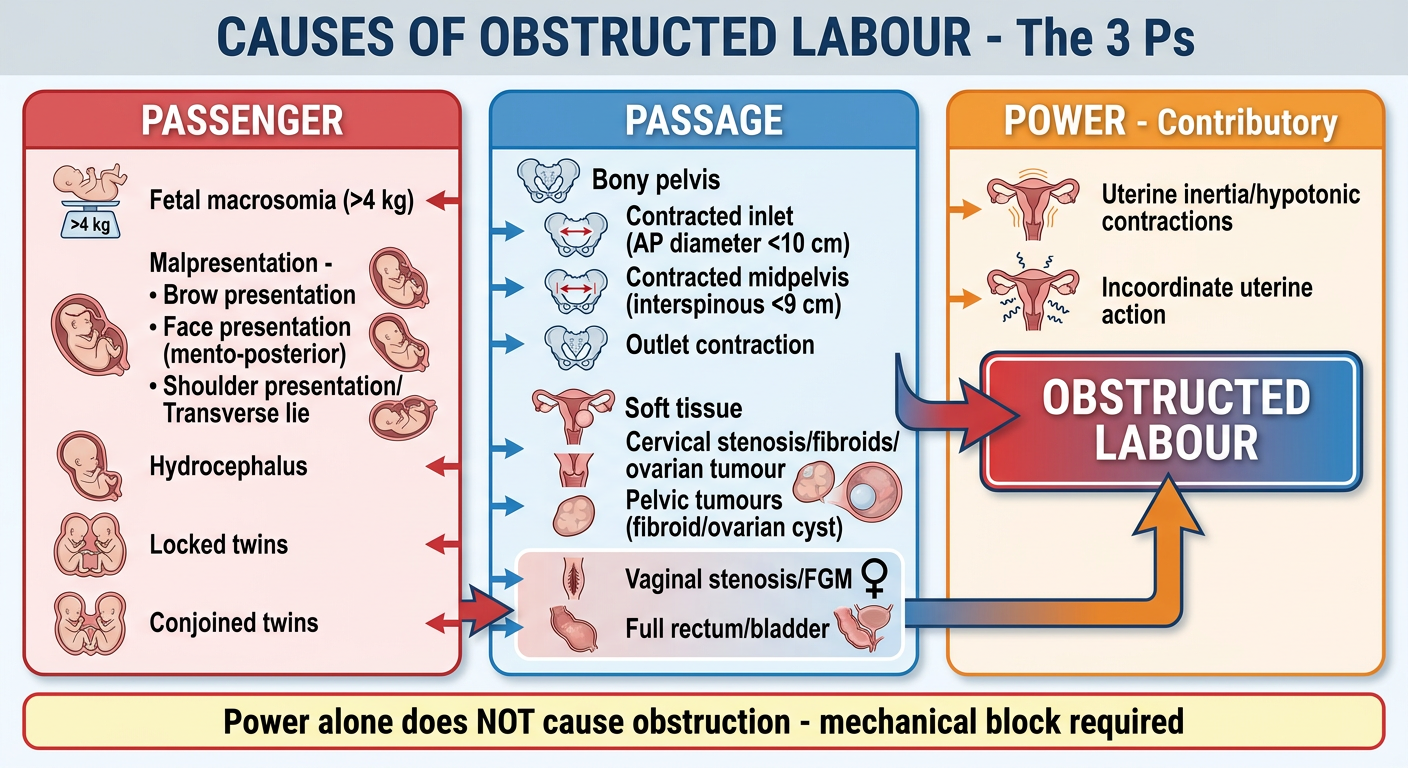
1. PASSENGER (Fetal Factors)
| Cause | Details |
|---|---|
| Macrosomia | Fetal weight >4 kg |
| Malpresentation | Shoulder/transverse lie (most dangerous), Brow presentation (always obstructs), Face (mento-posterior), Footling breech |
| Malposition | Deep transverse arrest, Persistent occipito-posterior |
| Fetal abnormalities | Hydrocephalus (large head), Conjoined twins, Abdominal tumours (Wilms', cystic hygroma) |
2. PASSAGE (Maternal Factors)
- Contracted inlet: AP diameter <10 cm, transverse <12 cm
- Contracted midpelvis: interspinous diameter <9 cm (most common site of arrest)
- Outlet contraction: interspinous <8 cm
- Causes: childhood malnutrition, rickets/osteomalacia, trauma (pelvic fracture), kyphoscoliosis
- Uterine fibroids in lower segment
- Ovarian cyst occupying pelvis
- Cervical stenosis (post-conization, carcinoma)
- Vaginal stenosis (FGM, post-repair, congenital)
- Full rectum or bladder (preventable!)
- Pelvic kidney, sacral tumour
3. POWER (Contributory only)
- Uterine hypotonia, incoordinate contractions
- Power alone NEVER causes obstruction but makes it worse
PATHOPHYSIOLOGY - WHAT HAPPENS IN THE UTERUS
Normal Retraction Ring (Physiological)
↓ (if obstruction continues)
Upper segment thickens, contracts harder
Lower segment becomes thin, over-distended
↓
BANDL'S PATHOLOGICAL RETRACTION RING forms
(visible/palpable groove at umbilicus level)
↓
Lower segment becomes paper-thin
↓
UTERINE RUPTURE (catastrophic)
Bandl's Retraction Ring
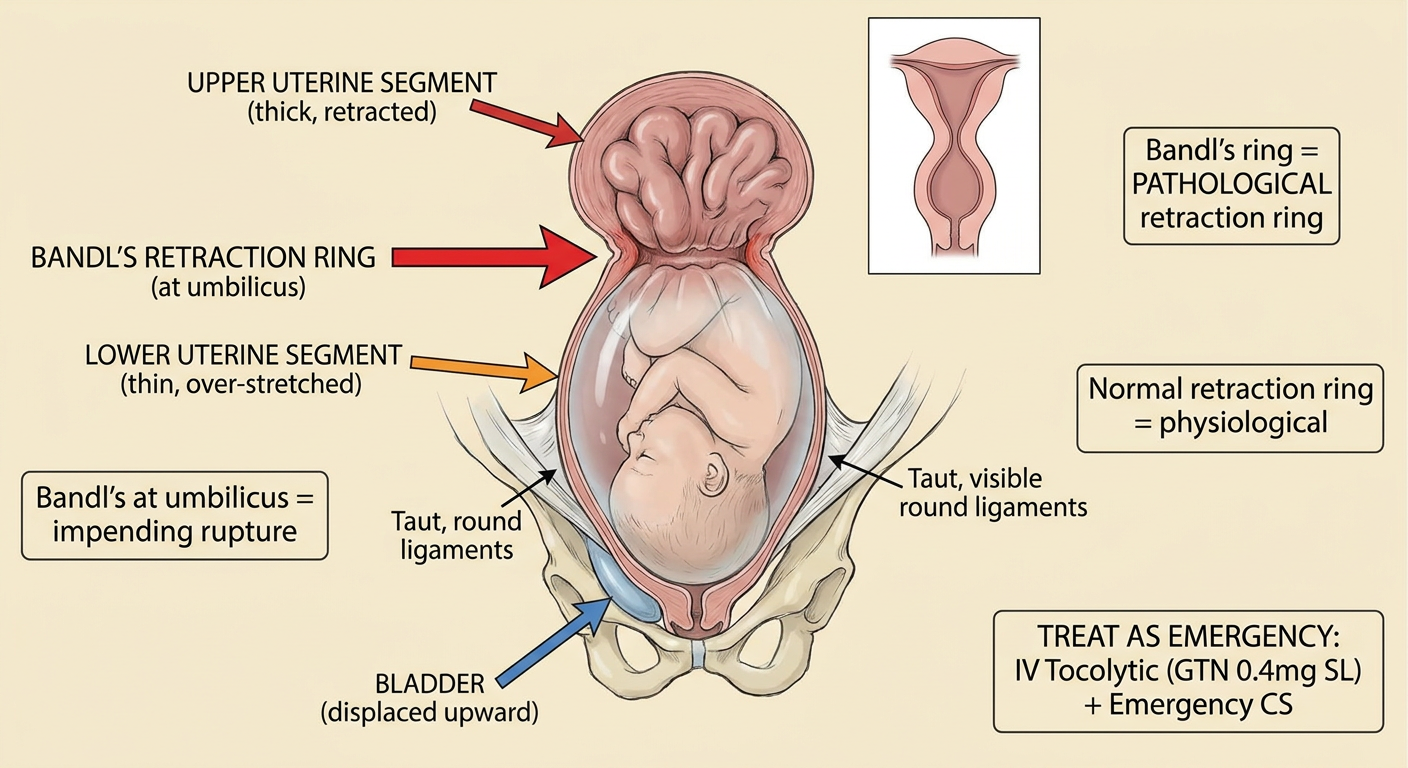
- Formed at the junction of upper and lower uterine segments
- Normally the physiological ring is at/below umbilicus - when it rises to the umbilicus, it is now PATHOLOGICAL (Bandl's ring)
- Represents impending uterine rupture - treat as emergency
- Queensland Clinical Guidelines (2025): Use bedside ultrasound to identify Bandl's ring in suspected obstructed labour
CLINICAL FEATURES
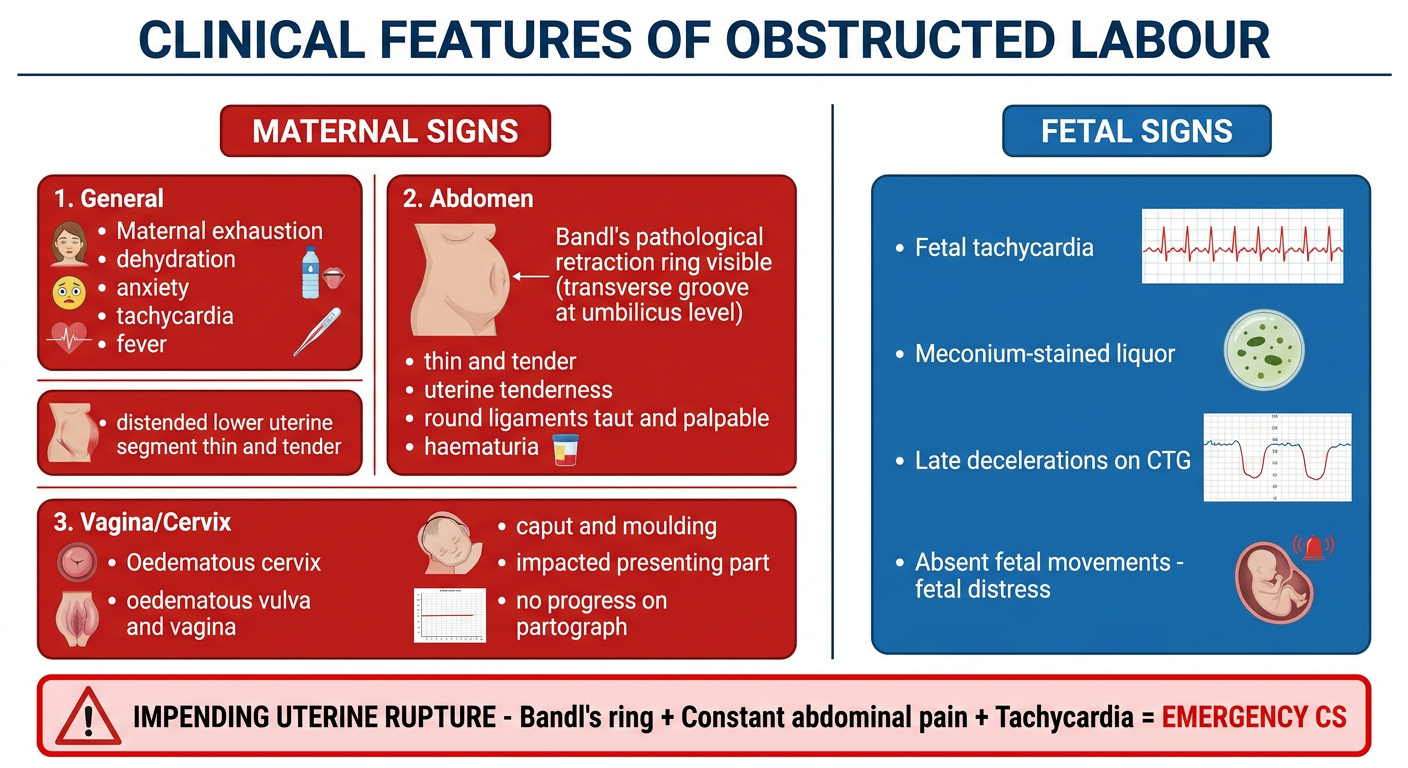
MATERNAL FEATURES
- Maternal exhaustion, dehydration, anxiety
- Tachycardia (>100 bpm), pyrexia if infection
- Dehydration: dry tongue, sunken eyes, oliguria
- Uterus continuously tense and tender (tonic contraction)
- Bandl's ring visible as transverse groove at or above umbilicus
- Lower segment is distended, thin, tender to touch
- Round ligaments taut and palpable bilaterally
- Haematuria (bladder compressed between fetal head and pubic symphysis)
- Fetal parts difficult to palpate
- Presenting part: deeply impacted, no descent
- Severe caput succedaneum (+++ to +++)
- Moulding (overlapping of fetal skull bones - grade 2-3)
- Cervix: oedematous, poorly applied, may not dilate further
- Vaginal walls: oedematous
- No progress on repeat examination after 2-4 hours
FETAL FEATURES
- Fetal tachycardia (>160 bpm)
- Meconium-stained liquor
- Late decelerations / variable decelerations on CTG
- Absent fetal movements
ON PARTOGRAPH
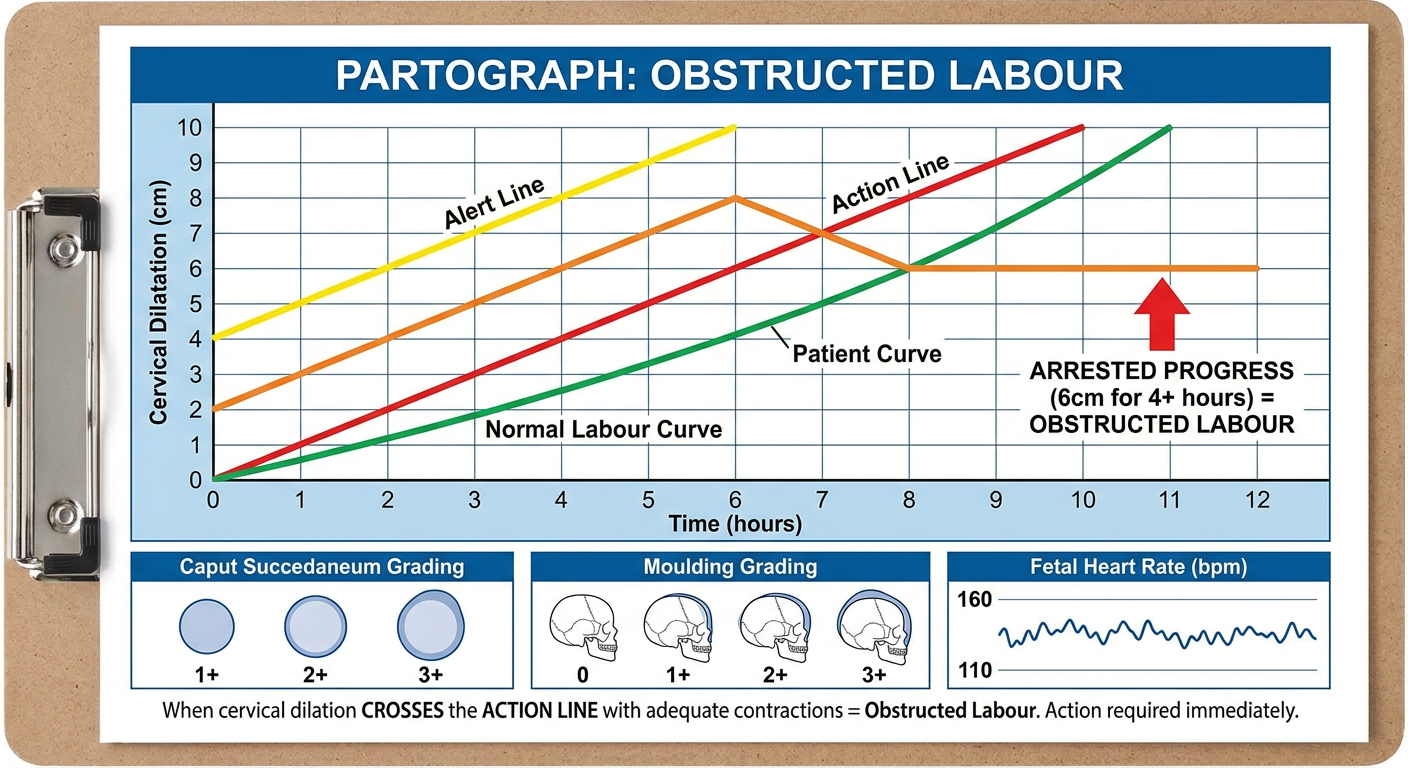
- Cervical dilation crosses the Alert Line → assess and plan
- Cervical dilation crosses the Action Line → MANDATORY intervention
- Alert line = expected minimum progress (1 cm/hour in active phase)
- Action line = 4 hours to the right of alert line
- WHO emphasises monitoring caput and moulding as signs of CPD - not just cervical dilation
DIAGNOSIS
- No progress in labour for ≥2 hours in active phase despite adequate contractions
- Signs of obstruction (Bandl's ring, caput, moulding, maternal exhaustion)
- Partograph: crossing the action line
- CBC (anaemia, leukocytosis)
- Blood group and crossmatch
- Blood glucose, electrolytes, renal function
- Urine: haematuria (bladder compression)
- CTG: fetal distress
- Ultrasound: presentation, estimated fetal weight, amniotic fluid, identify Bandl's ring (Queensland 2025)
- X-ray pelvimetry: rarely done now; CT pelvimetry if genuine CPD suspected
MANAGEMENT
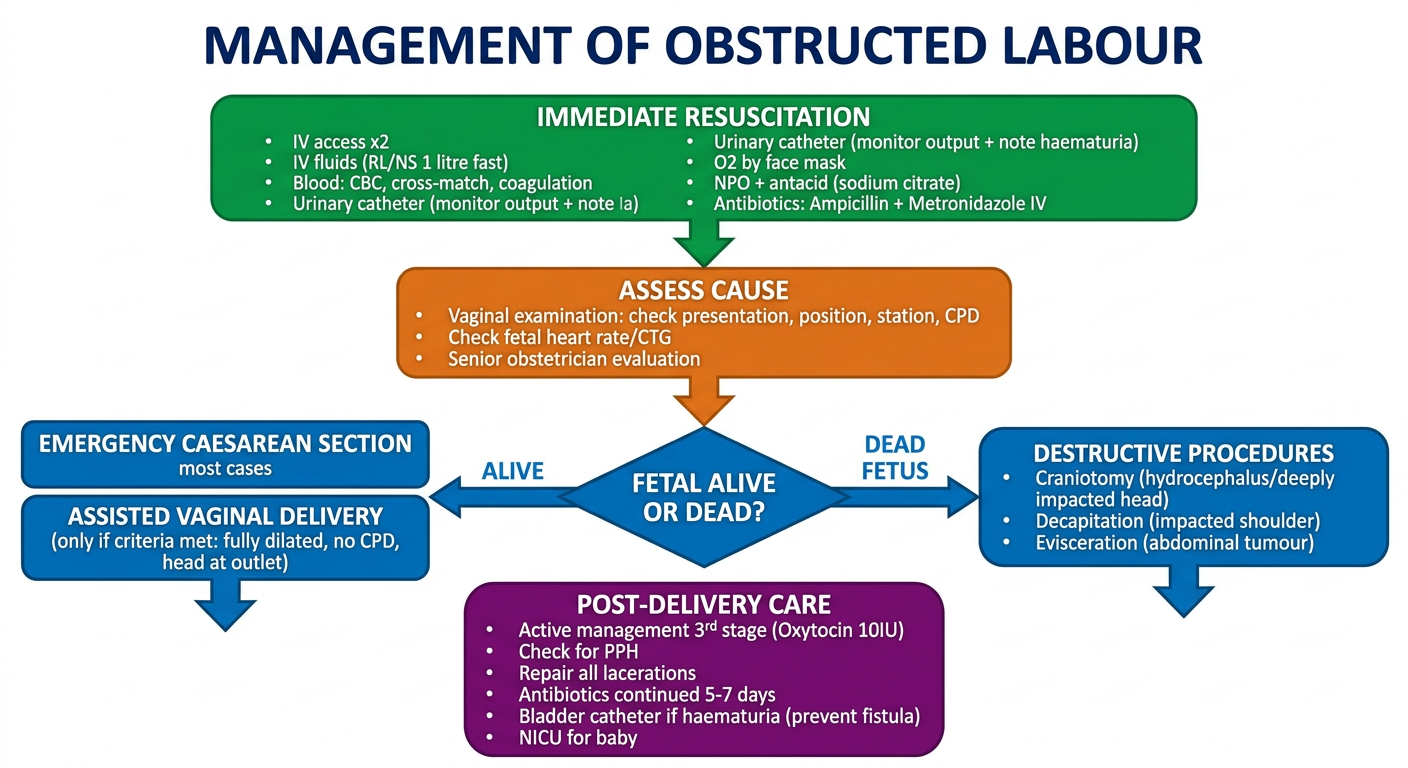
STEP 1: IMMEDIATE RESUSCITATION (ALWAYS FIRST)
A - Airway + O₂ by face mask 8-10 L/min
B - Breathing assessment
C - Circulation:
→ IV access x2 (large bore 16G)
→ IV fluids: Ringer's Lactate 1L fast (correct dehydration)
→ Blood: CBC, cross-match 2 units, coagulation
→ Urinary catheter (strict I/O; note haematuria)
D - Drugs:
→ Antibiotics: Ampicillin 2g IV + Metronidazole 500mg IV
→ Antacid: Sodium citrate 30 mL orally (aspiration prevention)
→ NPO
E - Evaluate fetus: CTG, fetal heart rate
STEP 2: ASSESS AND DECIDE
- Is fetus alive or dead?
- What is the presentation?
- Is vaginal delivery possible? (Full dilatation + vertex at outlet + no severe CPD)
- Is uterine rupture present or imminent?
STEP 3: DEFINITIVE MANAGEMENT
A. LIVE FETUS (Most Cases) - Emergency Caesarean Section
- CS is the treatment of choice for most cases of obstructed labour with live fetus
- Indications: CPD, malpresentation, fetal distress, Bandl's ring
- Special considerations in CS for obstructed labour (covered in detail in previous answer)
- Cervix fully dilated (10 cm)
- Head at +2 to +3 station (outlet)
- No significant CPD
- No Bandl's ring or uterine rupture
- Fetus not in severe distress
B. DEAD FETUS (Destructive Operations)
| Operation | Indication |
|---|---|
| Craniotomy | Hydrocephalus / deeply impacted dead fetus |
| Decapitation | Impacted shoulder presentation (dead fetus) |
| Evisceration | Fetal abdominal tumour causing obstruction |
| Cleidotomy | Fetal shoulder too wide (division of clavicle) |
| Pubiotomy/Symphysiotomy | Rarely done; contracted pelvis |
Note: Destructive operations require fully dilated cervix, dead fetus, and MUST be performed by experienced hands under anaesthesia
C. SHOULDER DYSTOCIA (Special Case - Live Fetus)
HELPERR Mnemonic:
H - Call for Help
E - Evaluate for Episiostomy
L - Legs: McRoberts manoeuvre (hyperflexion of thighs)
P - Suprapubic Pressure (NOT fundal)
E - Enter (Rubin II / Woods screw internal rotation)
R - Remove posterior arm
R - Roll to all-fours (Gaskin manoeuvre)
STEP 4: POST-DELIVERY CARE
- Active management of third stage: Oxytocin 10 IU IV immediately at delivery
- Check for and repair all lacerations
- Continue IV antibiotics 5-7 days (high infection risk)
- Bladder catheter for 10-14 days if haematuria present (prevents VVF formation)
- Neonatologist present at delivery; NICU admission if needed
- Monitor for PPH, urine output, wound infection
- DVT prophylaxis: LMWH + compression stockings
- Debrief patient and family
COMPLICATIONS
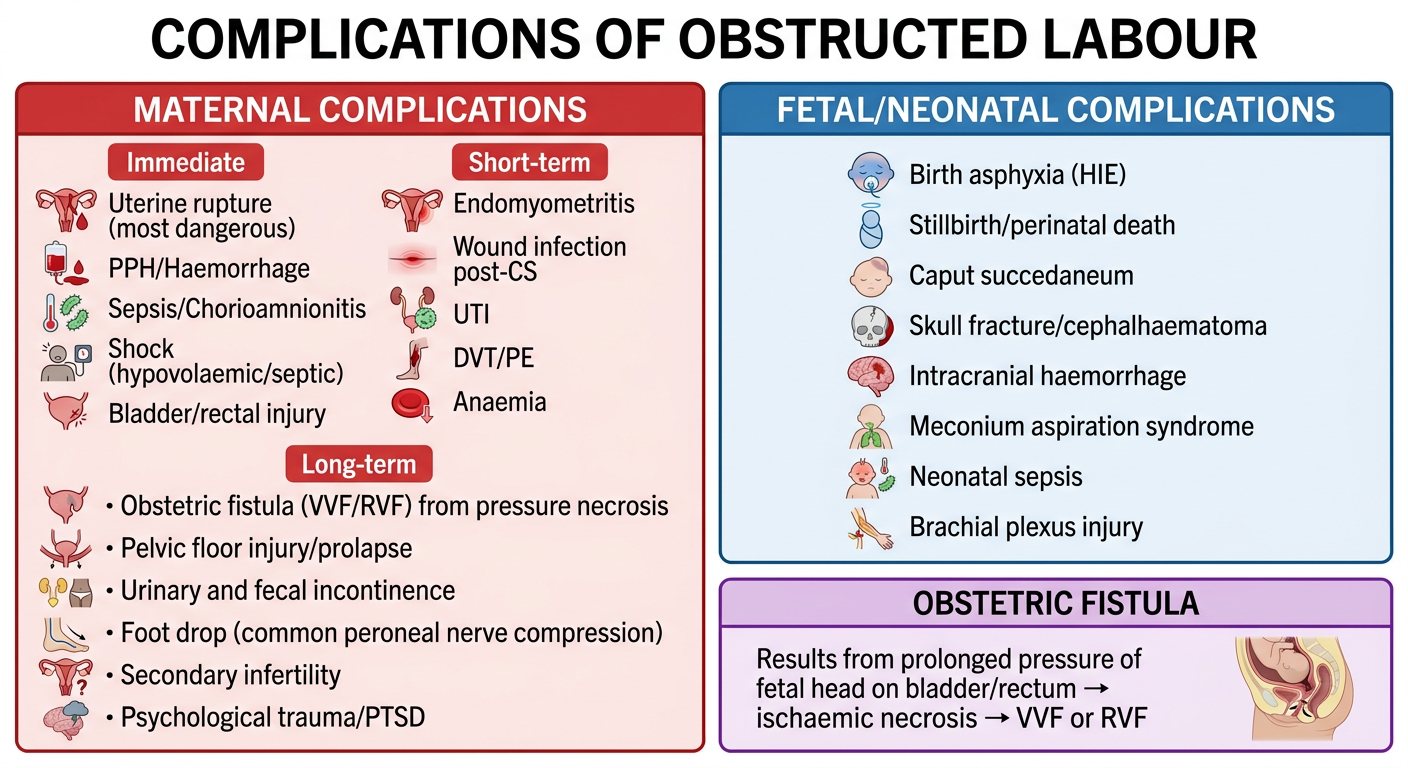
MATERNAL COMPLICATIONS
- Uterine rupture (most dangerous - 5-10% mortality)
- Haemorrhage/PPH (uterine atony due to exhausted uterus)
- Shock (hypovolaemic or septic)
- Bladder/bowel injury
- Puerperal sepsis / chorioamnionitis
- Endomyometritis
- Wound infection
- UTI
- DVT / Pulmonary embolism (RCOG: #1 cause of maternal death in UK)
- Anaemia
| Complication | Mechanism |
|---|---|
| Obstetric Fistula (VVF/RVF) | Prolonged compression of bladder/rectum between fetal head and pubic bone → ischaemic necrosis → fistula (develops 5-10 days post-delivery) |
| Foot drop | Common peroneal nerve compression from prolonged lithotomy/squatting |
| Pelvic organ prolapse | Pelvic floor damage |
| Urinary/faecal incontinence | Sphincter and pelvic floor injury |
| Secondary infertility | Pelvic adhesions, uterine scar, Asherman's |
| Psychological trauma / PTSD |
Williams Obstetrics Ch. 23: "Because of impaired circulation, necrosis may result and become evident several days after delivery as vesicovaginal, vesicocervical, or rectovaginal fistulas."
FETAL/NEONATAL COMPLICATIONS
- Perinatal asphyxia / HIE (hypoxic-ischaemic encephalopathy)
- Stillbirth / perinatal death
- Caput succedaneum (scalp oedema)
- Skull fracture / cephalhaematoma
- Intracranial haemorrhage
- Meconium aspiration syndrome
- Neonatal sepsis (from chorioamnionitis)
- Brachial plexus injury
- Cerebral palsy (long-term)
PREVENTION
| Level | Measure |
|---|---|
| Primary | Nutrition, delay marriage/pregnancy until pelvis mature, prevent FGM |
| Secondary | Antenatal care: detect CPD, malpresentation; plan delivery in high-risk women |
| Tertiary | Partograph monitoring in ALL labours (WHO mandate), early referral, timely CS |
QUICK REVISION BOX
| Feature | Details |
|---|---|
| Definition | Failure of descent despite adequate contractions - mechanical block |
| Most common cause | CPD (contracted midpelvis in developed, bony contracted pelvis in developing world) |
| Hallmark sign | Bandl's ring + haematuria + maternal exhaustion |
| Diagnostic tool | Partograph (action line crossing) |
| Treatment of choice (live fetus) | Emergency Caesarean Section |
| Treatment (dead fetus) | Destructive operations |
| Most feared complication | Uterine rupture |
| Long-term complication | Obstetric fistula (VVF) |
| Prevention tool | Partograph + early referral |
KEY REFERENCES
- Williams Obstetrics 26th Ed, Ch. 23 - Abnormal Labour (Cunningham, Leveno et al.)
- Creasy & Resnik's Maternal-Fetal Medicine - Complications of Cesarean Delivery
- Queensland Clinical Guidelines: Prolonged and/or Obstructed Labour (2025)
- WHO IMPAC Guidelines - Managing Complications in Pregnancy and Childbirth
- RCOG Green Top Guideline No. 45 - Birth After Previous Caesarean Birth
- MSF Medical Guidelines - Obstructed Labour Management