Community participation in national health programs
community participation national health programs public health importance strategies
Community Participation in National Health Programs
Definition
"The process by which individuals and families assume responsibility for their own health and welfare and for those of the community, and develop the capacity to contribute to their and the community's development."
- Park's Textbook of Preventive and Social Medicine, p. 811-822
Historical Background
- Mere socialization of medicine (e.g., nationalization of health services as in UK 1946, Soviet Union) was found insufficient to ensure utilization of health services. Community participation was recognized as the missing element.
- The Declaration of Alma-Ata (1978) was the landmark document that formally embedded community participation as a pillar of global health policy, giving it "a new meaning and direction."
- It called on governments to formulate national policies and plans to launch Primary Health Care (PHC) as part of their national health systems.
- The Ottawa Charter (1986) further reinforced community participation as a core principle of health promotion.
Why Community Participation is Essential
- Universal coverage is impossible without it - no country can achieve PHC goals without involvement of local communities
- Local resource mobilization - manpower, money, and materials at the grassroots level
- Cultural acceptability - health workers from the community overcome cultural and communication barriers
- Equity - shifts the center of gravity of healthcare from urban elite to rural underserved populations
- Demedicalization of health - shifts health from being a service for people to a responsibility of people
- Sustainability - community-driven programs are more self-reliant and durable
"The war against disease and for health cannot be fought by physicians alone. It is a people's war in which the entire population must be mobilized permanently." - Henry Sigerist (medical historian)
Three Ways a Community Can Participate
| Mode | Description |
|---|---|
| Contribution | Providing facilities, manpower, logistic support, and possibly funds |
| Active involvement | Participating in planning, management, and evaluation of programs |
| Utilization | Joining in and using health services, especially preventive and protective measures |
- Park's Textbook, p. 1829
Community Participation in Primary Health Care (PHC)
- Social equity
- Nationwide coverage
- Self-reliance
- Intersectoral coordination
- Community participation in planning and implementation
Community Participation in India's National Health Programs
Key Community-Level Workers
| Worker | Program | Role |
|---|---|---|
| ASHA (Accredited Social Health Activist) | National Health Mission (NHM) | First point of contact; health education, referrals, maternal and child health |
| Anganwadi Worker | Integrated Child Development Services (ICDS) | Nutrition, immunization, pre-school education |
| Multipurpose Health Worker (MPHW) | PHC network | Comprehensive family health |
| Village Health Guide | Village Health Guides' Scheme (1977) | Community-based PHC, especially in rural areas |
| Trained Dai | MCH programs | Traditional birth attendance, safe delivery support |
National Programs Using Community Participation
- National Health Mission (NHM) - ASHA is the backbone of community outreach
- National Mental Health Programme (1982) - launched to ensure mental health care for the community at risk and underprivileged sections
- MCH/FP services - now integral parts of PHC with emphasis on community participation and intersectoral coordination (National Health Policy 2002, National Population Policy 2000)
- Disease control programs (TB, malaria, leprosy, STDs) - PHC framework with community participation, political support, and intersectoral coordination
- Health for All (HFA) by 2000 AD and now the Sustainable Development Goals (SDGs) - framed around community-based approaches
Levels of Health Care and Community Participation
| Level | Setting (India) | Community Element |
|---|---|---|
| Primary | PHC, subcentres | ASHA, Anganwadi, village health guides - direct community contact |
| Secondary | District hospital, CHC | First referral level; community feeds into this level |
| Tertiary | Medical colleges, AIIMS | Specialized; community referrals upstream |
Barriers to Community Participation
- Social fragmentation - caste and religious divisions (especially in India) obstruct complete participation
- Professional resistance - historically, the greatest resistance came from the medical profession itself, not the lay public
- Lack of community awareness - limited health literacy
- Political and administrative inertia - lack of genuine political will
- Cultural heterogeneity - no single standard pattern of community participation can be universally applied; flexibility of approach is essential
- Urban bias in health resource distribution - three-quarters of health budgets spent in cities, three-quarters of the population in rural areas
"Community participation has become an aphorism that is still awaiting genuine realization in many countries of the world." - Park's Textbook, p. 1831
"Deprofessionalization" of Medicine
- Educator
- Case-finder
- Preventive care provider
- Counsellor
- Agent of social change
Intersectoral Coordination - The Necessary Partner
- Agriculture and animal husbandry
- Food and nutrition
- Industry and housing
- Education
- Public works and communication
Key Declarations and Milestones
| Year | Event | Significance |
|---|---|---|
| 1978 | Alma-Ata Declaration | Community participation enshrined as core of PHC |
| 1981 | Global Strategy - HFA by 2000 | 34th World Health Assembly adopted PHC globally |
| 1986 | Ottawa Charter | Health promotion through community action |
| 1997 | Jakarta Declaration | Reaffirmed community participation for health promotion |
| 2000 | Millennium Development Goals | Community-based approaches to health/poverty |
| 2015 | Sustainable Development Goals | SDG 3 (Good Health) with community-centered framework |
- Park's Textbook of Preventive and Social Medicine (primary source throughout)
Epidemiology of ebola
Ebola virus disease epidemiology 2024 2025 outbreaks WHO
"Ebola virus disease" epidemiology
Epidemiology of Ebola Virus Disease (EVD)
1. The Virus - Classification and Species
| Species | Human Disease | Notes |
|---|---|---|
| Zaire ebolavirus | Yes - highest fatality (50-95%) | Responsible for most major outbreaks |
| Sudan ebolavirus | Yes (~50% CFR) | 2025 Uganda outbreak caused by this |
| Bundibugyo ebolavirus | Yes | First identified 2007, Uganda |
| Tai Forest ebolavirus | Yes (single case) | Scientist infected from chimpanzee autopsy, survived, 1994 |
| Reston ebolavirus | No (non-pathogenic in humans) | From Philippine monkeys; asymptomatic antibodies found |
| Bombali ebolavirus | No known human disease | Identified in bats |
- Sherris & Ryan's Medical Microbiology, 8th Ed.; Goodman & Gilman's
2. Historical Discovery and First Outbreaks
- 1976 - Two simultaneous outbreaks:
- Northern Zaire (DRC): CFR ~90% (Zaire strain)
- Southern Sudan: CFR ~50% (Sudan strain)
- These were initially thought to be the same virus; later shown to be antigenically distinct
- 1967 - Marburg virus (sister filovirus) first described in Germany/Yugoslavia from African monkeys; foundational event for understanding filoviruses
- 1990 - Reston ebolavirus isolated from Philippine monkeys in a U.S. quarantine facility; non-pathogenic in humans
- 1994 - Tai Forest (Ivory Coast) strain identified; single scientist infected from chimpanzee autopsy, survived
3. Major Outbreaks - Chronology
The 2014-2016 West Africa Epidemic (Largest in History)
| Parameter | Data |
|---|---|
| Start | March 2014, Guinea |
| Countries primarily affected | Guinea, Liberia, Sierra Leone |
| Other countries affected | Nigeria, Senegal, Mali, Spain, USA, UK, Italy |
| Total estimated cases | 28,652 |
| Laboratory-confirmed cases | 15,261 |
| Deaths | 11,325 |
| CFR | ~70% (WHO estimate) |
| Duration | ~2 years (ended March 31, 2016) |
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025); Rosen's Emergency Medicine
2018-2020 DRC Outbreak (Second Largest)
| Parameter | Data |
|---|---|
| Cases | ~3,470 |
| Deaths | ~2,287 |
| CFR | ~66% |
| Complicating factors | Armed conflict, community distrust, remote terrain |
| New tools deployed | Ring vaccination (rVSV-ZEBOV), FDA-approved monoclonal antibodies |
Other DRC Outbreaks
- 2017: 8 cases, 4 deaths (CFR 61%)
- 2020: 138 cases, 55 deaths (CFR 42.3%)
2025 Outbreaks (Most Recent)
- DRC - 16th outbreak (declared September 4, 2025): Bulape Health Zone, Kasai Province; 64 cases (53 confirmed, 11 probable), 45 deaths, CFR 70.3% (as of November 2025) - a new spillover event from unknown reservoir
- Uganda (declared January 30, 2025): Sudan virus strain in Kampala - notable because no approved vaccine exists for Sudan strain
4. Geographic Distribution
- Outbreaks confined primarily to sub-Saharan Africa, especially the DRC (formerly Zaire)
- DRC has experienced the most outbreaks - 16 as of 2025
- Other affected countries: Uganda, Sudan, Gabon, Republic of Congo, Guinea, Liberia, Sierra Leone
- The DRC remains the epicenter due to high biodiversity, rainforest habitat, and contact with wildlife
5. Reservoir and Zoonotic Transmission
- Filoviruses are zoonotic - spillover from infected animals to humans initiates outbreaks
- Infected animals include: fruit bats, non-human primates (apes, monkeys), and duikers (antelope)
- The primary route of zoonotic transmission is unknown - contact with bat droppings, eating infected bush meat, or handling infected primates are suspected routes
- The Bombali ebolavirus species has been identified directly in bats without causing human disease
6. Mode of Transmission (Human-to-Human)
- Direct contact with blood or body fluids (urine, saliva, sweat, feces, vomit, breast milk, semen) of infected, sick, or deceased persons
- Sexual transmission (oral, vaginal, anal) - demonstrated epidemiologically
- Fomite transmission via contaminated needles, syringes, clothing, or bedding
- Unsafe burials - deceased EVD patients are highly infectious; traditional burial practices (washing/touching the body) have driven major transmission chains
- Nosocomial (healthcare-associated) transmission - a critical amplifier, especially in settings lacking PPE
Individuals are not contagious until they develop symptoms. This is an important epidemiological distinction that supports the feasibility of contact tracing.
7. Incubation Period
- Range: 2 to 21 days (average 4-10 days)
- The 21-day period is used for surveillance and quarantine purposes
8. Case Fatality Rate (CFR)
- Overall range: 25% to 90% across outbreaks
- Average: ~50% (historically)
- Zaire strain: 50-95% (highest)
- Sudan strain: ~50%
- CFR varies significantly by:
- Quality of supportive care available
- Access to specific treatments (monoclonal antibodies)
- Timing of diagnosis
- Health system capacity
- In settings with quality supportive/critical care, outcomes are demonstrably better - affirming EVD is treatable even without antivirals
9. Clinical Features (Brief)
| Phase | Features |
|---|---|
| Early (days 1-5) | High fever, severe headache, myalgias, malaise, sore throat, vomiting, diarrhea |
| Later (days 5-10) | Hemorrhagic manifestations: spontaneous bleeding, ecchymosis, petechiae; erythematous maculopapular rash (desquamates) |
| Severe | Hypovolemia, metabolic derangements, shock, multiorgan failure |
10. Pathogenesis (Brief)
- Ebola infects and lyses monocytes, macrophages, dendritic cells, and reticuloendothelial cells
- Release of inflammatory cytokines damages vascular integrity - leading to hemorrhage and shock
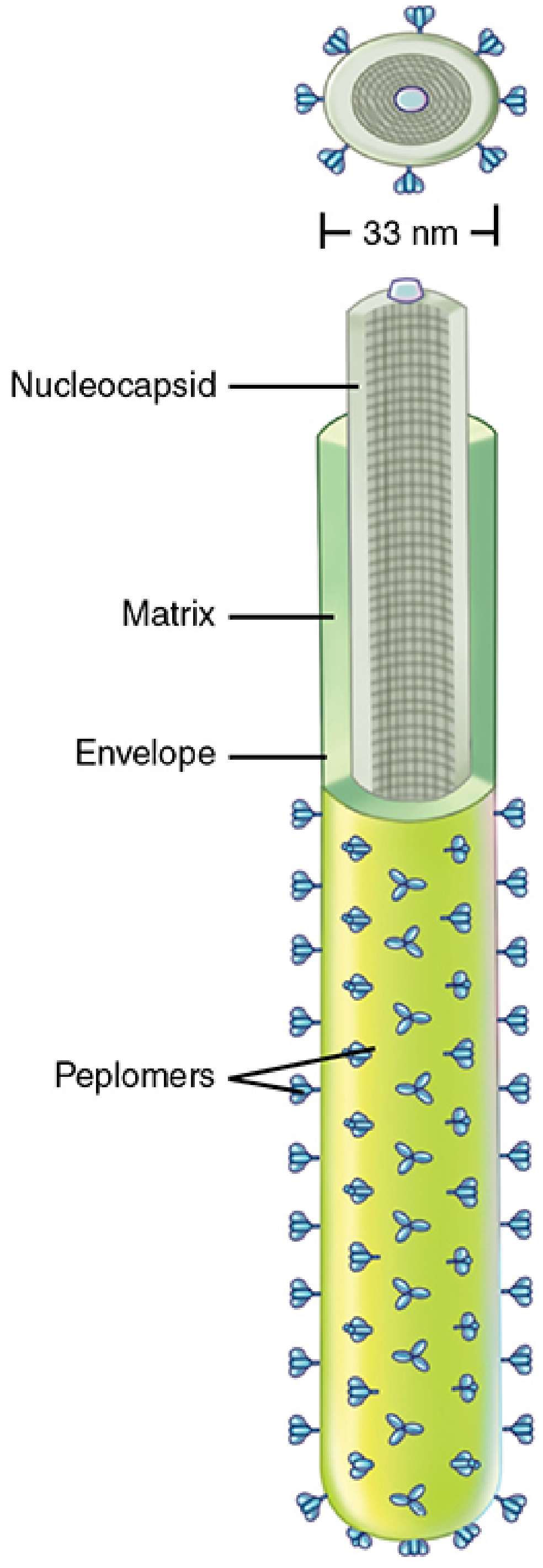
- The glycoprotein (GP) on the viral envelope mediates attachment and entry into host cells - it is the target of approved monoclonal antibody therapies
11. Diagnosis
- RT-PCR on plasma specimen: current gold standard
- Rapid antigen point-of-care test: 15-minute turnaround; good sensitivity/specificity compared to RT-PCR
- Laboratory findings: thrombocytopenia, anemia, coagulopathy, elevated transaminases, elevated creatinine, hypocalcemia, hypokalemia
- Testing should only be done for patients meeting both exposure history and clinical criteria
- Malaria testing (thick and thin blood smear) is mandatory - it is far more common in endemic areas
12. Prevention and Treatment
Vaccines
- rVSV-ZEBOV (Ervebo) - FDA-approved 2019; live attenuated recombinant VSV vector expressing Zaire ebolavirus glycoprotein; single IM dose; deployed using ring vaccination strategy in DRC 2018-2020
- Indicated for persons 18+ who are: outbreak responders, workers at Ebola treatment centers, or BSL-4 lab workers
- Only covers Zaire strain - no approved vaccine for Sudan or other strains (a major gap in the 2025 Uganda outbreak)
Specific Treatments (FDA-approved for Zaire ebolavirus)
- Inmazeb (atoltivimab + maftivimab + odesivimab) - cocktail of 3 recombinant human IgG1 mAbs targeting Zaire GP
- Ebanga (ansuvimab) - single mAb targeting Zaire GP
Infection Control
- Strict PPE (full barrier precautions)
- Safe burial practices
- Isolation of suspected/confirmed cases
- Contact tracing and quarantine (21-day window)
- Decontamination of fomites
13. Factors Driving Outbreaks
- Weak health systems - inadequate PPE, no running water, no labs
- Unsafe burials - cultural practices involving contact with the deceased
- Healthcare amplification - poor infection control
- Community mistrust - of health workers and authorities; impedes surveillance
- Armed conflict - hampers response in DRC (2018-2020)
- Lack of vaccines for non-Zaire strains - especially Sudan strain
- Delayed diagnosis - nonspecific early presentation
- Urban spread - 2014-2016 marked the first major urban epidemic
A 2025 systematic review and meta-analysis (PMID 41219638) from Uganda found that diagnostic delays and slow response timeliness significantly increased outbreak-level case-fatality ratios.
Summary Table
| Feature | Details |
|---|---|
| Family | Filoviridae |
| Genus | Ebolavirus |
| Genome | ssRNA, negative-sense |
| Human-pathogenic species | Zaire, Sudan, Bundibugyo, Tai Forest |
| Natural reservoir | Fruit bats (probable, unconfirmed) |
| Transmission | Contact with body fluids; unsafe burials; nosocomial |
| Incubation | 2-21 days (avg. 4-10 days) |
| CFR | 25-90% (avg. ~50%) |
| Largest outbreak | 2014-2016 West Africa: 28,652 cases, 11,325 deaths |
| Most affected country | DRC (16 outbreaks as of 2025) |
| Approved vaccine | Ervebo (Zaire only) |
| Approved treatment | Inmazeb, Ebanga (Zaire only) |
| Most recent outbreaks | DRC (Sep 2025), Uganda (Jan 2025) |
Create a flashcard of epidemiology of ebola for a quick revision
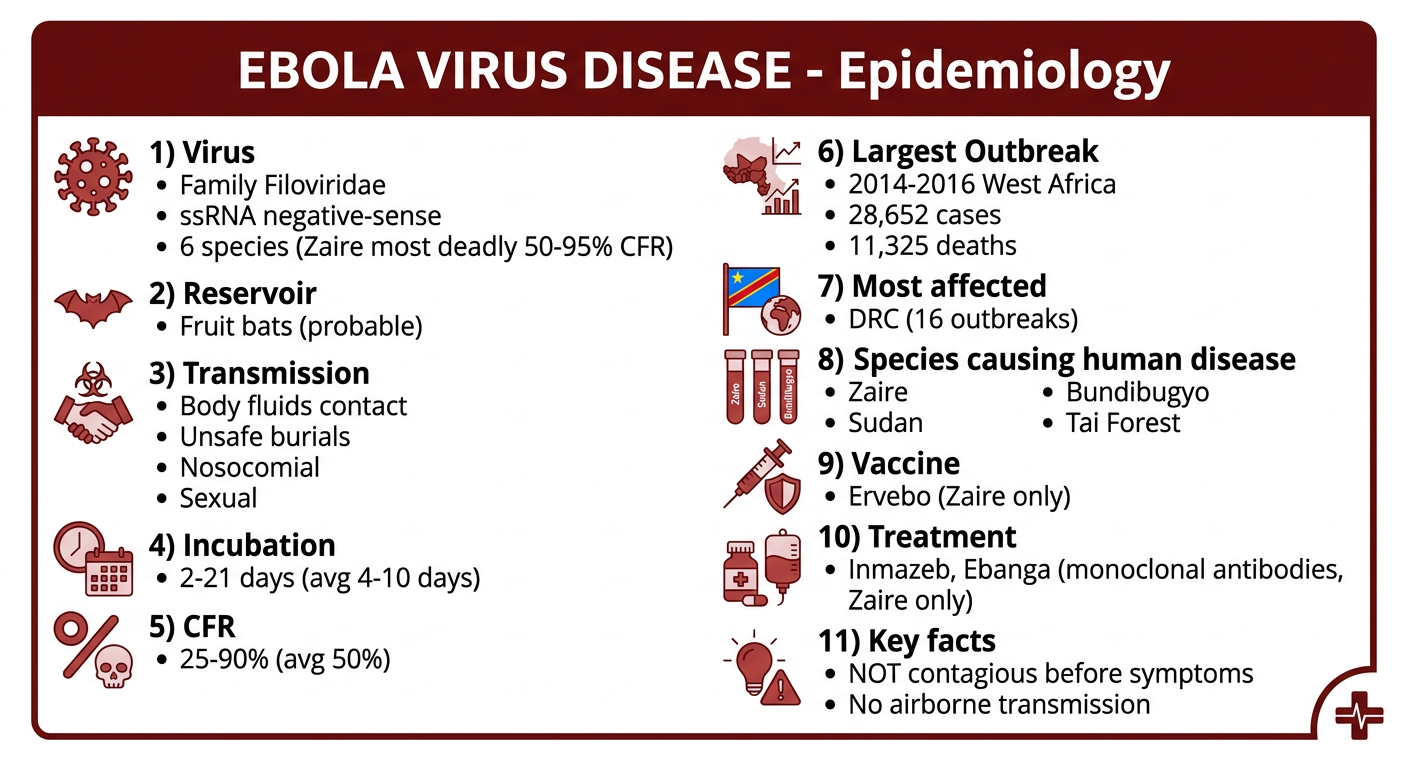
Medical flashcard for quick revision on Epidemiology of Ebola Virus Disease. Clean, professional medical study card design with a dark red and white color scheme. Title at top: "EBOLA VIRUS DISEASE - Epidemiology". Organized sections with icons or bullet points covering: 1) Virus: Family Filoviridae, ssRNA negative-sense, 6 species (Zaire most deadly 50-95% CFR). 2) Reservoir: Fruit bats (probable). 3) Transmission: Body fluids contact, unsafe burials, nosocomial, sexual. 4) Incubation: 2-21 days (avg 4-10 days). 5) CFR: 25-90% (avg 50%). 6) Largest Outbreak: 2014-2016 West Africa - 28,652 cases, 11,325 deaths. 7) Most affected: DRC (16 outbreaks). 8) Species causing human disease: Zaire, Sudan, Bundibugyo, Tai Forest. 9) Vaccine: Ervebo (Zaire only). 10) Treatment: Inmazeb, Ebanga (monoclonal antibodies, Zaire only). 11) Key facts: NOT contagious before symptoms; no airborne transmission. Modern clean medical infographic style with clear typography, color-coded sections, easy to read at a glance.
- Virus - Filoviridae family, negative-sense ssRNA, 6 species
- Reservoir - Fruit bats (probable)
- Transmission - Body fluids, unsafe burials, nosocomial, sexual
- Incubation - 2-21 days (avg 4-10)
- CFR - 25-90% (avg ~50%); Zaire strain highest (up to 95%)
- Biggest outbreak - 2014-2016 West Africa: 28,652 cases, 11,325 deaths
- Most outbreaks - DRC (16 outbreaks as of 2025)
- Human-pathogenic species - Zaire, Sudan, Bundibugyo, Tai Forest
- Vaccine - Ervebo (Zaire only, ring vaccination strategy)
- Treatment - Inmazeb & Ebanga (monoclonal antibodies, Zaire only)
- Key rule - NOT infectious before symptom onset (supports contact tracing)