Stroboscopy 10 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, exam-ready 10-mark MS ENT answer on Stroboscopy:
Stroboscopy
Definition
Laryngeal stroboscopy is an endoscopic technique that uses a pulsed (stroboscopic) xenon light source synchronized to the fundamental frequency of vocal fold vibration to create an optical illusion of slow-motion or "frozen" vocal fold movement. It is the standard clinical tool for evaluating vocal fold vibratory patterns that cannot otherwise be visualized by the naked eye.
Principle (Talbot's Law)
The human retina can resolve only 5 images per second (Talbot's Law of visual persistence). An image presented for less than 0.2 seconds (1/5 s) persists on the retina and fuses with subsequent images to produce apparent motion.
The vocal folds vibrate at 75-1000 Hz (cycles/second) during phonation - far too fast for the retina to resolve. Stroboscopy overcomes this by:
- Illuminating the larynx with brief xenon light flashes of approximately 1/1000 second duration each
- A contact microphone (or electroglottograph) senses the fundamental frequency (F0) of phonation in real time and controls the rate of xenon light firing
- When the flash rate is slightly out of phase with the vibratory rate, successive images are captured from marginally different points in successive vibratory cycles - fused by the retina to produce apparent slow-motion vibration
- When the flash rate is exactly in phase with the vibratory rate, the same phase of each cycle is captured repeatedly - producing an apparent "frozen" or stationary image
Equipment
A complete stroboscopy system includes:
- Xenon light source (allows rapid on/off pulsing)
- Rigid endoscope (70° or 90°) - preferred for higher resolution, contrast and magnification; requires sustained vowel "ee"; OR flexible nasolaryngoscope - allows connected speech assessment
- Camera and lens (HD digital camera)
- Contact microphone or electroglottograph for F0 sensing
- Monitor and digital recording system
- Printer for still images
Technique
Rigid endoscope (most common for stroboscopy):
- Patient sits slightly forward from hips, neck and chin extended, tongue protruded
- Examiner grasps tongue in gauze gently
- Scope advanced under the uvula until larynx is visualized
- Patient phonates sustained "ee" at conversational pitch and loudness
- Stroboscopic sequences captured at different pitches and intensities
Parameters Assessed (Stroboscopic Checklist)
| Parameter | Normal Finding | Significance of Abnormality |
|---|---|---|
| Symmetry | Both folds mirror images, equal amplitude | Asymmetry = mass/tension difference |
| Amplitude | Lateral excursion = 1/3 to 1/2 of visible fold width | Reduced = stiffness, lesion, paralysis |
| Periodicity | Regular, consistent successive cycles (folds "freeze") | Aperiodic = hoarseness, mass lesion, paralysis |
| Mucosal wave | Smooth horizontal wave propagating from inferior to superior fold surface | Absent/reduced = scar, stiffness, submucosal lesion, carcinoma |
| Glottal closure | Complete in men; small posterior gap acceptable in women | Incomplete = paralysis, atrophy, sulcus vocalis, bowing |
| Vertical phase difference | Inferior lip leads superior lip in opening/closing | Lost = stiffness, scarring |
| Supraglottic activity | Minimal false cord compression | Excess = functional dysphonia, muscle tension |
Mucosal Wave - Key Concept
The mucosal wave has two components:
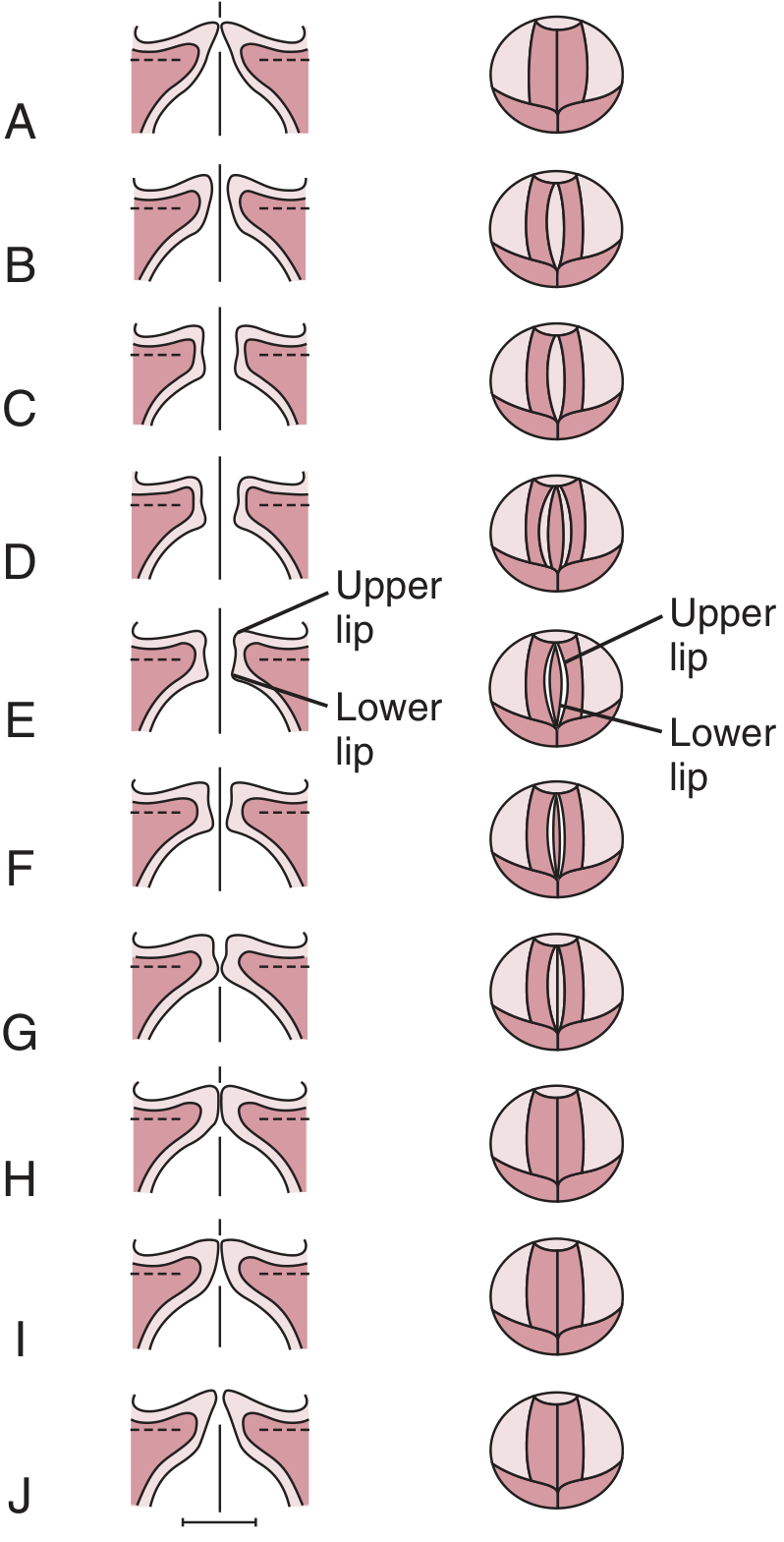
- Vertical phase: the inferior lip (lower mass) leads the superior lip (upper mass) in its movement away from and back to midline, seen on the medial surface of the fold
- Horizontal phase: described stroboscopically as a "ripple of light across the superior surface" - reflects pliability of the superficial lamina propria mucosa
Lesions that stiffen the mucosa (scar, carcinoma infiltrating the lamina propria) reduce or abolish the mucosal wave. Small lesions confined to the superficial lamina propria (vocal nodules, small cysts) may reduce and asymmetrize the wave but preserve some propagation.
Indications
- Dysphonia - any unexplained voice change
- Vocal fold lesions - to characterize mass, nodules, polyps, cysts, sulcus vocalis
- Vocal fold paralysis/paresis - assess residual vibration and mucosal wave
- Laryngeal carcinoma - assess depth of infiltration (lost mucosal wave implies subepithelial invasion)
- Professional voice users - baseline assessment and interval monitoring
- Post-phonosurgery - monitor tissue healing
- Functional dysphonia / muscle tension dysphonia
- Presbylaryngis / vocal fold atrophy
Advantages
- Changes clinical diagnosis in 30-47% of patients previously assessed with continuous light flexible endoscopy alone
- Provides additional diagnostic detail in a further 32%
- Detects submucosal lesions (scar, sulcus) that appear normal on continuous-light exam
- Video recording allows interval comparison over days/weeks/years
- Documents response to behavioral, medical, or surgical treatment
- Non-invasive; does not usually require topical anesthesia (rigid scope)
Limitations
- Requires periodic, sustained phonation at adequate loudness - not possible with very hoarse/breathy/severely dysphonic patients
- Not suitable for aperiodic vibration (aphonia), very short phonation segments, or whisper
- High-speed digital videolaryngoscopy (LHSV at ~4000 frames/sec) is superior for aperiodic vibrations and short phonation bursts - but stroboscopy remains the clinical standard
- Subjective interpretation - examiner training required; inter-rater variability exists
- Rigid scope limits assessment to sustained vowels - flexible scope preferred for connected speech
- Cannot assess pharyngeal motion or abduction/adduction (continuous light endoscopy is better for these)
Clinical Correlations
| Condition | Stroboscopic Finding |
|---|---|
| Vocal nodule/polyp | Reduced, asymmetric amplitude and mucosal wave at lesion site; glottal gap at lesion |
| Vocal fold scar | Absent or markedly reduced mucosal wave, adynamic segment |
| Sulcus vocalis | Adynamic segment, incomplete closure, reduced/absent wave |
| Vocal fold paralysis | Absent/minimal vibration on paralyzed side; incomplete closure |
| Early glottic carcinoma | Lost mucosal wave - suggests subepithelial infiltration |
| Functional dysphonia | Excessive supraglottic constriction, variable closure patterns |
Summary
Stroboscopy is an indispensable tool in the laryngologist's armamentarium. By exploiting Talbot's Law and using a xenon strobe synchronized to vocal fold F0, it converts imperceptibly rapid mucosal vibration into apparent slow motion, enabling detailed assessment of symmetry, amplitude, periodicity, mucosal wave, and glottal closure. These parameters guide diagnosis and management of virtually all disorders causing dysphonia.
(Cummings Otolaryngology: Head and Neck Surgery, 7th Ed., Chapter 58 - Laryngeal Stroboscopy)
This is a shared conversation. Sign in to Orris to start your own chat.