Can u create me a gi case presentation in peadiatrics and explain me it with logical reason and Simplified understanding
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything I need to build a thorough, student-friendly case presentation. Here it is:
🏥 Paediatric GI Case Presentation
Acute Appendicitis in a School-Age Child
📋 THE CASE
Patient: Adam, 9-year-old boy
Setting: Paediatric Emergency Department, brought by his mother
🗣️ Chief Complaint
"My tummy has been hurting for 18 hours and it keeps getting worse."
📖 History of Presenting Illness
Adam woke up at midnight with a dull, poorly localised pain around his belly button. His mum thought it was a stomach bug. By morning, he had vomited twice and completely refused breakfast (anorexia). Over the next several hours, the pain gradually moved down and to the right side of his abdomen and became much sharper. He now refuses to walk normally and walks hunched over. He has a low-grade fever of 38.3°C. No diarrhoea. Last bowel movement was yesterday.
Key timeline:
- 0 hrs - Dull periumbilical pain
- 6 hrs - Nausea and vomiting
- 12 hrs - Pain shifts to right lower quadrant (RLQ)
- 18 hrs - Fever develops, pain is now sharp and constant
🔍 Past History & Social History
- No prior abdominal surgeries
- No known illnesses
- Up to date on vaccinations
- Normal diet and development
🩺 Physical Examination
| Finding | Result |
|---|---|
| Temperature | 38.3°C |
| Heart rate | 108 bpm (mildly elevated) |
| Respiratory rate | 20/min |
| BP | Normal |
| Abdomen | Guarding and tenderness at McBurney's point (RLQ) |
| Rebound tenderness | Positive (pain worse when pressure suddenly released) |
| Rovsing's sign | Positive (pressure on LEFT side causes pain on the RIGHT) |
| Child's posture | Lying still with right hip slightly flexed |
🧪 Investigations
Blood tests:
| Test | Adam's Result | Normal |
|---|---|---|
| WBC | 14,500 /mm³ | < 10,000 |
| Neutrophils | 82% | < 75% |
| CRP | 48 mg/L | < 5 |
Urine dipstick: Trace white cells (sterile pyuria - explained below)
Ultrasound (RLQ):
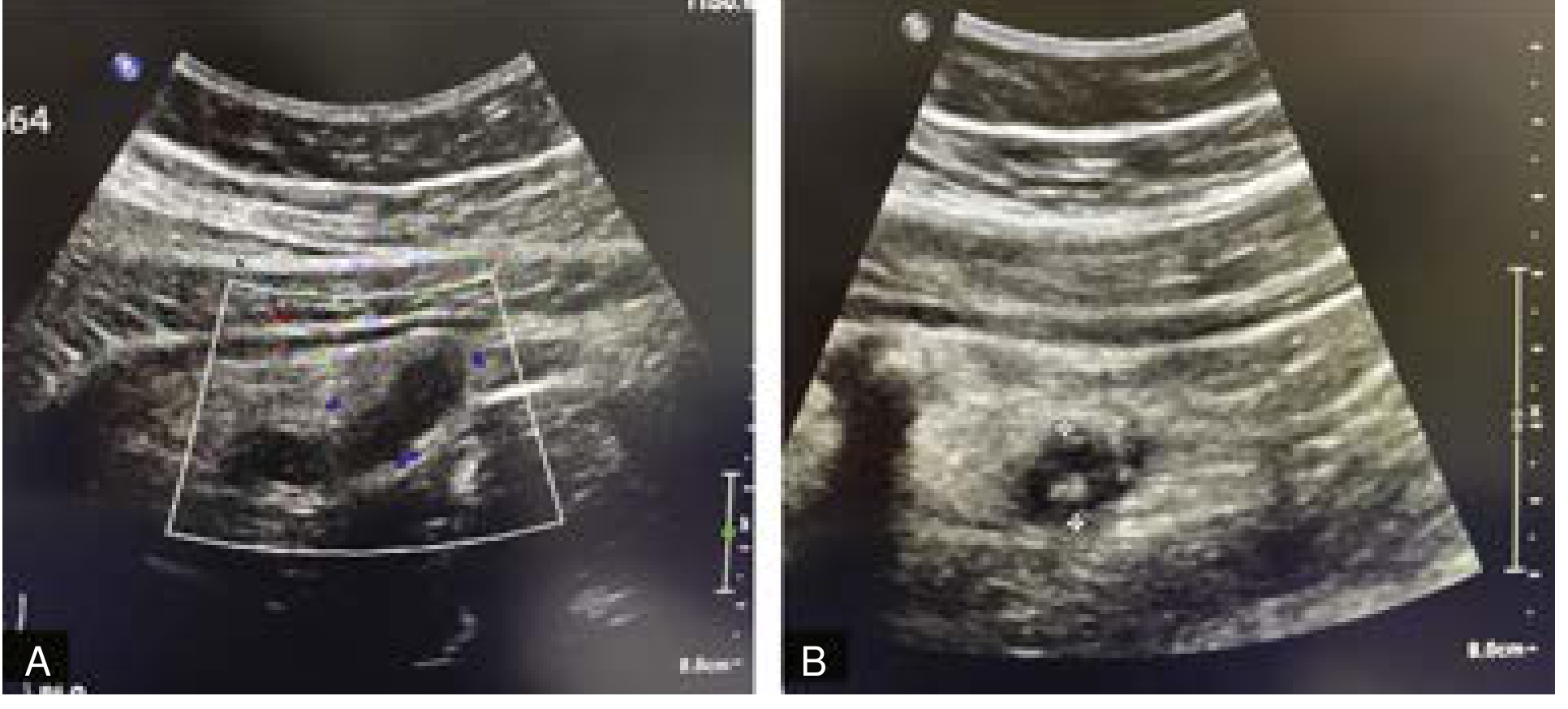
Ultrasound of the right lower quadrant showing a dilated, fluid-filled tubular structure with increased vascularity (A) and an echogenic focus consistent with an appendicolith (B) - classic findings of acute appendicitis.
- Appendix diameter: 8 mm (normal < 6 mm)
- Non-compressible with pressure
- Appendicolith (hardened stool pellet) visible
🎯 Diagnosis
Acute Appendicitis with Appendicolith
Pediatric Appendicitis Score (PAS): 8/10 → High probability of appendicitis
🧠 LOGICAL EXPLANATIONS - "WHY DOES THIS HAPPEN?"
1. Why did the pain start at the belly button?
Think of it like this: the appendix is a hollow tube. When it first gets blocked, it swells up. That swelling stretches nerve fibres inside the appendix wall - these are called visceral nerves, and they are very bad at pinpointing exactly where the pain is coming from. So the brain registers the pain vaguely, somewhere in the middle of the abdomen - the belly button area. This is called visceral (referred) pain.
Analogy: It's like when you have a stomach ache - you can feel something is wrong but you can't point to exactly one spot.
2. Why did the pain move to the right lower quadrant?
As hours pass, the inflammation spreads outside the appendix wall and reaches the lining of the abdominal wall (the peritoneum). The peritoneum has somatic nerves that are very good at locating pain precisely. Now Adam can point to exactly where it hurts - McBurney's point, which is 2/3 of the way from the belly button to the right hip bone (anterior superior iliac spine). This migration of pain is a hallmark of appendicitis.
Analogy: It's like a small fire that starts inside a room (vague alarm) and then burns through the wall (you can now see exactly where the fire is).
3. Why did he stop eating (anorexia) and vomit?
When the appendix distends, it stimulates the vagus nerve, which triggers nausea and vomiting reflexes. Anorexia comes from the body's general inflammatory response (cytokines like IL-6 suppress appetite). These symptoms almost always appear before the pain moves to the RLQ - this sequence is important for diagnosis.
4. Why does he have a fever and high white blood cells?
The blocked appendix fills with bacteria (mainly E. coli and Bacteroides fragilis). The body mounts an immune response:
- WBC rises - the bone marrow sends out more neutrophils to fight infection
- Neutrophilia (>75%) - neutrophils are the "first responders" in bacterial infection
- CRP rises - the liver produces this as part of the acute phase response
- Fever - cytokines signal the hypothalamus to raise body temperature to kill bacteria
5. Why does he lie still with his hip bent?
The appendix sits near the iliopsoas muscle (a deep hip flexor muscle). When inflamed, it irritates this muscle. Bending the hip relaxes the psoas, reducing pain. This is called a positive psoas sign. Adam instinctively finds the least painful position.
6. What is Rovsing's sign and why is it positive?
When you press the LEFT side of the abdomen, you push intestinal contents toward the right. This increases pressure at the inflamed appendix, causing pain on the RIGHT. It confirms the pain source is truly in the RLQ, not just referred from elsewhere.
7. Why does the urine show white cells if it's not a urine infection?
The inflamed appendix lies very close to the ureter and bladder. The nearby inflammation "leaks" into the urinary space, causing a small number of white cells to appear in the urine without any actual infection - this is called sterile pyuria. This can mislead doctors into thinking it's a urinary tract infection, so it's important to interpret it in context.
8. Why is ultrasound used instead of CT scan in children?
Children's bodies are still developing, and radiation from CT scans increases the lifetime risk of cancer. Ultrasound uses sound waves (zero radiation) and in experienced hands has ~78% sensitivity and 83% specificity for appendicitis. CT is reserved for cases where ultrasound is inconclusive - if used, low-dose techniques are preferred. MRI is another radiation-free option.
Sources: Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11e
📊 PEDIATRIC APPENDICITIS SCORE (PAS)
This scoring tool helps decide how likely appendicitis is:
| Feature | Points | Adam's score |
|---|---|---|
| Nausea/vomiting | 1 | ✅ 1 |
| Anorexia | 1 | ✅ 1 |
| Fever ≥38°C | 1 | ✅ 1 |
| Migration of pain | 1 | ✅ 1 |
| WBC > 10,000 | 1 | ✅ 1 |
| Neutrophilia >75% | 1 | ✅ 1 |
| RLQ tenderness | 2 | ✅ 2 |
| Pain with hopping/coughing | 2 | ✅ 2 (positive rebound) |
| TOTAL | 10 | 8/10 = HIGH RISK |
A score of ≥7 strongly suggests appendicitis. Adam scores 8.
💊 MANAGEMENT
Step 1 - Immediately
- IV access + IV fluids (Adam is dehydrated from vomiting and not eating)
- Nil by mouth (NBM/NPO) - he may need surgery
- IV analgesia - giving pain relief does NOT mask the diagnosis and is the humane approach
- Broad-spectrum IV antibiotics - e.g., piperacillin-tazobactam to cover bowel organisms
Step 2 - Definitive Treatment
Laparoscopic appendectomy (keyhole surgery) - the gold standard.
Why laparoscopic and not open?
- Smaller cuts = less pain post-operatively
- Faster recovery - many children go home the same day
- Lower infection rates
- Despite a smaller working space in children, conversion to open surgery is rarely needed
Step 3 - If Perforated (Complicated)
If Adam had presented later with a ruptured appendix:
- Antibiotics continued for at least 5 days post-operatively (APSA guidelines)
- If there is an abscess, interventional radiology drain placement first, then interval appendectomy in 6-8 weeks
⚠️ DIFFERENTIAL DIAGNOSES TO EXCLUDE
| Condition | Key Distinguishing Feature |
|---|---|
| Mesenteric adenitis | Lymph nodes swollen after a viral illness; no peritonism |
| Urinary tract infection | Dysuria, positive urine culture |
| Meckel's diverticulitis | Similar presentation; diagnosed intra-operatively |
| Crohn's disease | Chronic symptoms, perianal disease, raised calprotectin |
| Constipation | Hard stool palpable, relieved by laxatives |
| Testicular torsion (boys) | Scrotal pain/swelling - always examine the scrotum! |
🔑 KEY TEACHING POINTS - REMEMBER THESE
- Pain migration (periumbilical → RLQ) is the classic hallmark of appendicitis
- Anorexia + vomiting BEFORE pain migration = classic sequence
- Appendicitis is the most common acute surgical emergency in children
- In children, ultrasound first (never CT as first line)
- Children perforate faster than adults - don't delay!
- PAS score ≥7 = high probability → go to theatre
- A positive urine dip does NOT rule out appendicitis (sterile pyuria can occur)
- Always examine the genitalia in boys to exclude testicular torsion
Sources: Current Surgical Therapy 14e (Elaa Mahdi & Pegoli), Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.