Ways to increase testosterone and what test to be done if muscle mass is not gaining
Reading File
Finding Sources
Finding Sources
Searching the Web
how to increase testosterone naturally and tests for low testosterone muscle mass not gaining 2025
Searching PubMed
testosterone deficiency diagnosis treatment muscle
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from Harrison's, Goldman-Cecil, Tietz, and Smith & Tanagho Urology textbooks, plus web sources. Let me compile the full answer.
Testosterone: How to Increase It & What Tests to Order When Muscle Mass Isn't Gaining
Why Testosterone Matters for Muscle Mass
Testosterone is the primary anabolic hormone in men. Low testosterone (hypogonadism) directly causes decreased skeletal muscle mass and strength, reduced bone mineral density, decreased libido, fatigue, and changes in mood. Age-related decline starts around age 30-40 at roughly 0.5-2% per year. - Harrison's Principles of Internal Medicine 22E, p.3159; Tietz Textbook of Laboratory Medicine 7E, p.2358
Part 1: Evidence-Based Ways to Increase Testosterone
A. Lifestyle (Most Effective First)
| Intervention | Mechanism | Evidence |
|---|---|---|
| Weight loss / reduce body fat | Excess adipose tissue increases aromatase activity, converting testosterone to estrogen. Even 15-20 lbs of weight loss makes a significant difference. | Strong |
| Resistance training (weightlifting) | Stimulates acute testosterone release and long-term hormonal optimization. High-intensity compound lifts (squats, deadlifts) have the greatest effect. | Strong |
| Sleep 7-9 hours nightly | Sleep-restricted men (5 hrs/night) show a 10-15% drop in daytime testosterone within one week. Most testosterone is produced during deep sleep. | Strong |
| Reduce chronic stress / cortisol | Cortisol directly suppresses testosterone synthesis at the Leydig cell level. Mindfulness, exercise, and sleep all lower cortisol. | Moderate |
| Aerobic exercise | Improves insulin sensitivity and metabolic health, which supports the HPG axis. However, excessive endurance training (overtraining) can suppress testosterone. | Moderate |
B. Nutrition and Micronutrients
- Zinc - Direct role in testosterone synthesis. Zinc deficiency is linked to significantly lower testosterone; supplementation in deficient men restores levels. Food sources: oysters, red meat, pumpkin seeds, legumes.
- Vitamin D - Functions as a steroid hormone precursor. Low vitamin D is associated with lower testosterone. Sun exposure or supplementation (vitamin D3) can help if deficient.
- Magnesium - Supports free testosterone levels, especially in athletes. Found in leafy greens, nuts, whole grains.
- Healthy fats - Dietary fat (especially monounsaturated and saturated fat in moderate amounts) is the raw material for steroidogenesis. Extremely low-fat diets suppress testosterone.
- Avoid excessive alcohol - Alcohol is directly toxic to Leydig cells and suppresses testosterone production.
- Maintain caloric balance - Both severe caloric restriction and obesity lower testosterone.
C. Supplements with Some Evidence (not miracle cures)
- Ashwagandha (Withania somnifera) - Modest but consistent testosterone-increasing effect in multiple trials, likely via cortisol reduction.
- D-Aspartic acid - May briefly raise LH and testosterone; evidence is mixed.
- Fenugreek - Some evidence for maintaining testosterone and improving libido.
- Most commercial "T-boosters" - Little to no evidence. Be skeptical. Per Examine.com's analysis, they mostly boost libido without changing actual testosterone levels.
D. Medical / Clinical Intervention (when lifestyle is insufficient)
If hypogonadism is confirmed, Testosterone Replacement Therapy (TRT) is evidence-based and increases lean muscle mass, maximal voluntary strength, and muscle power - Harrison's 22E, p.257. Forms include:
- Intramuscular injections (testosterone cypionate/enanthate) every 2-3 weeks
- Transdermal gels or patches (daily)
- Subcutaneous injections (weekly, lower peaks/troughs)
- Oral testosterone undecanoate (newer option)
The Endocrine Society recommends TRT only when there are consistent symptoms AND confirmed low testosterone AND no contraindications (prostate cancer history, poorly controlled heart failure). - Tietz Laboratory Medicine 7E, p.2357
Part 2: Tests to Order When Muscle Mass Is Not Gaining
When muscle gains plateau or seem inadequate despite training, a structured hormonal and metabolic workup is needed. Here is the clinical approach:
Step-by-Step Diagnostic Algorithm
First-Line Blood Tests
| Test | Why It's Ordered | Key Thresholds |
|---|---|---|
| Total serum testosterone (morning, fasting) | The primary screening test. Must be drawn between 7-11 AM (diurnal peak). | <230 ng/dL = likely deficient; <264 ng/dL = borderline; >350 ng/dL = unlikely to need TRT |
| SHBG (Sex Hormone Binding Globulin) | High SHBG can make total testosterone look normal when free/bioavailable testosterone is low. Elevated with aging, hyperthyroidism, liver disease. | Ordered alongside total T |
| Free testosterone (calculated or measured) | Order when total T is borderline (200-400 ng/dL) or SHBG is abnormal. Low free T with normal total T still causes symptoms. | Check if total T is borderline |
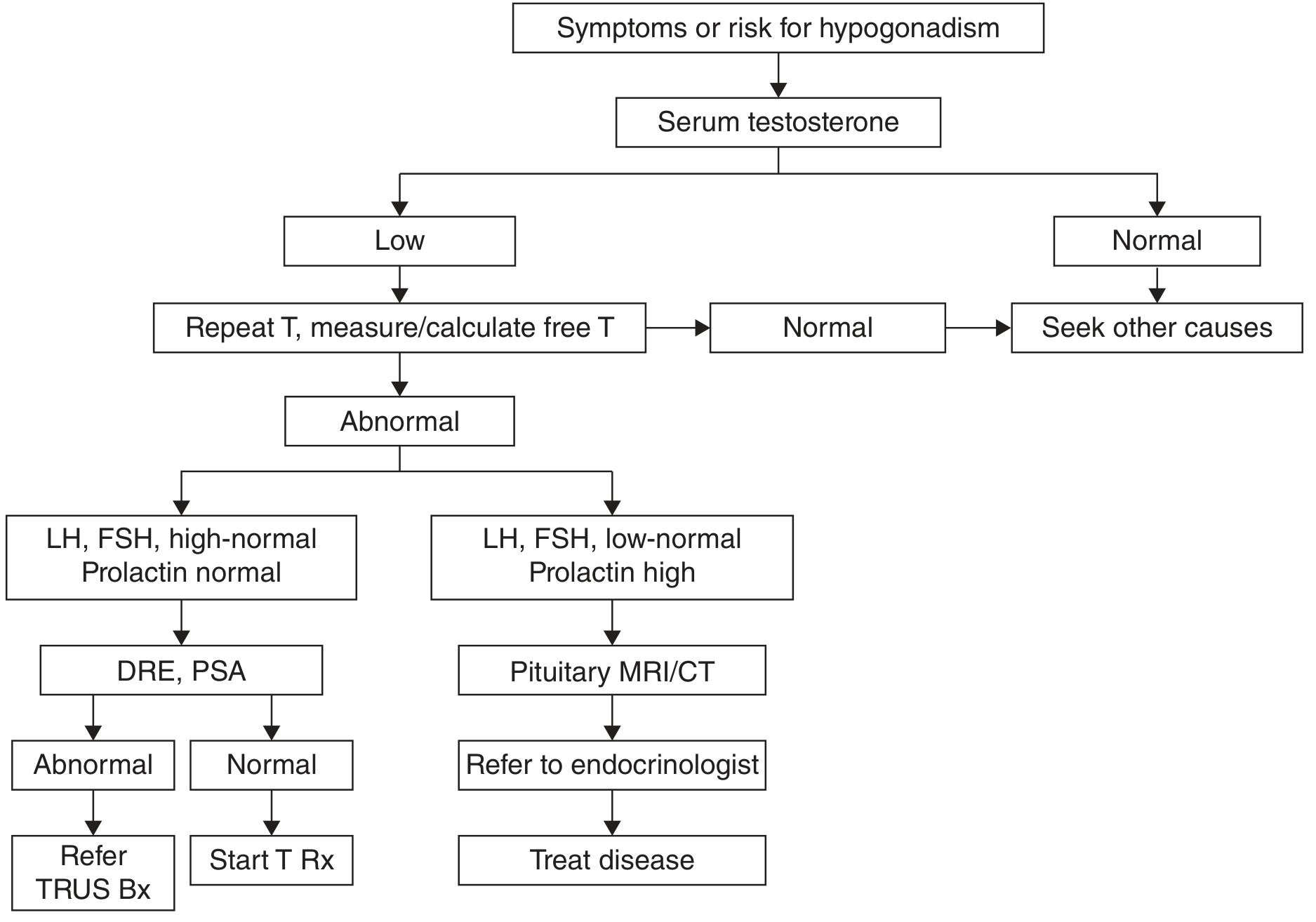
If first total T is low, repeat the test on a separate morning before diagnosing hypogonadism (transient illness or stress can lower T). - Tietz Laboratory Medicine 7E, p.2358
Second-Line Tests (if total T is confirmed low)
| Test | Purpose |
|---|---|
| LH (Luteinizing Hormone) | Differentiates primary vs. secondary hypogonadism. High LH + low T = primary (testicular failure, e.g., Klinefelter). Low/normal LH + low T = secondary (pituitary/hypothalamic problem). |
| FSH (Follicle-Stimulating Hormone) | Further characterizes gonadal axis function. |
| Prolactin | Order if total T < 150 ng/dL or if secondary hypogonadism is suspected. Elevated prolactin points to a pituitary adenoma (prolactinoma) that suppresses the HPG axis. |
| Thyroid function (TSH, free T4) | Hypothyroidism causes fatigue, weight gain, poor muscle gain, and can lower testosterone indirectly. |
| IGF-1 (Insulin-like Growth Factor-1) | Screens for growth hormone deficiency, which also impairs muscle anabolism. |
| Cortisol (morning) | Chronic hypercortisolism (Cushing's syndrome) causes muscle wasting and suppresses testosterone. |
| CBC (Complete Blood Count) | Baseline hemoglobin/hematocrit before starting TRT; hypogonadism causes anemia. |
| Fasting glucose / HbA1c + Fasting insulin | Insulin resistance and metabolic syndrome lower testosterone. |
| Comprehensive metabolic panel (CMP) | Liver disease raises SHBG and increases aromatization; kidney disease affects protein metabolism. |
| Lipid panel | Cardiovascular risk assessment, important if TRT is considered. |
Additional Tests in Specific Scenarios
| Scenario | Additional Test |
|---|---|
| Suspected pituitary cause (low LH/FSH + low T + high prolactin) | MRI of pituitary gland |
| Low bone density suspected | DXA (DEXA) scan of hip and spine for bone mineral density |
| Men >45 years, before TRT | PSA (Prostate-Specific Antigen) + Digital Rectal Exam |
| Suspected adrenal issue | DHEA-S (Dehydroepiandrosterone sulfate) |
| Nutritional gaps suspected | 25-OH Vitamin D, Zinc, Magnesium levels |
- Smith & Tanagho General Urology 19E, p.753-754; Goldman-Cecil Medicine 2E, p.372-374
Quick Summary
To increase testosterone naturally:
- Lose excess body fat
- Lift weights (resistance training)
- Sleep 7-9 hours
- Fix deficiencies: zinc, vitamin D, magnesium
- Reduce alcohol, chronic stress
- Eat adequate healthy fats and calories
Tests to run when muscle isn't gaining:
- Start: Fasting morning total testosterone + SHBG
- If low T confirmed: LH, FSH, prolactin, TSH, IGF-1, cortisol, CBC, fasting glucose/insulin, CMP, lipid panel
- Imaging if needed: Pituitary MRI (if secondary hypogonadism), DEXA scan (bone density)
If testosterone is actually normal and muscle still isn't growing, the problem likely lies elsewhere - inadequate protein intake, poor sleep, overtraining, or another hormonal issue (thyroid, growth hormone, insulin resistance). A sports medicine physician or endocrinologist can guide the full workup.
This is a shared conversation. Sign in to Orris to start your own chat.