KF ring
Reading File
Finding Sources
Searching Images
Kayser-Fleischer ring eye Wilson disease
Reading File
Reading File
Reading File
Kayser-Fleischer (KF) Ring
What is it?
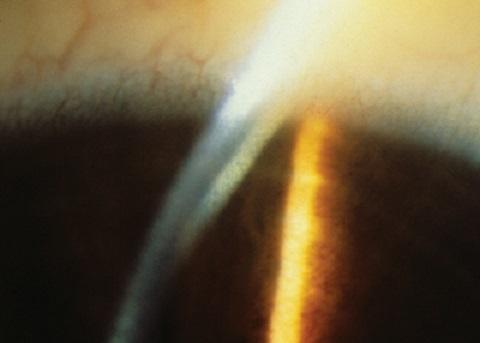
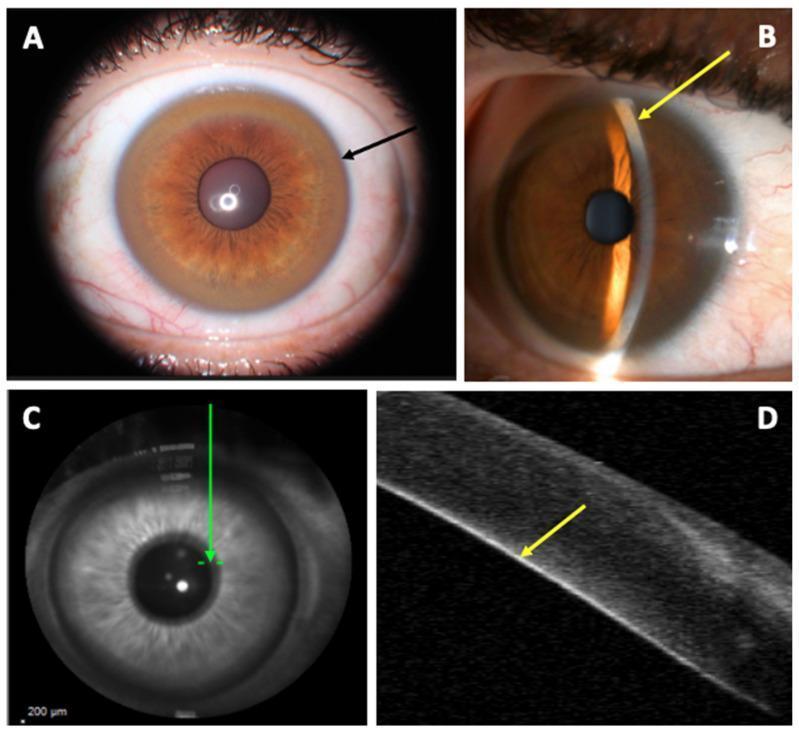
The Kayser-Fleischer ring is a 1–3 mm golden-brown, green, or reddish band at the corneal periphery caused by copper deposition in Descemet's membrane near the limbus. It is the pathognomonic ocular sign of Wilson disease (hepatolenticular degeneration — autosomal recessive mutation in the ATP7B gene on chromosome 13, impairing copper excretion).
Appearance & Location
- Color: yellow-brown, green, or reddish
- Location: peripheral cornea at the limbus, within Descemet's membrane
- First appears superiorly (may only be visible on gonioscopy early on), then inferiorly, and eventually forms a complete ring circumferentially
- Fluid streaming causes preferential copper accumulation at the superior and inferior poles before encircling the entire cornea
Detection
| Method | Notes |
|---|---|
| Slit-lamp examination | Gold standard; narrow slit beam shows deposition at Descemet's |
| Gonioscopy | Used when early ring not visible on slit lamp |
| Anterior-segment OCT | Detects early rings as linear hyperreflective material on Descemet's; useful when slit lamp is equivocal |
Rings are visible to the naked eye only when iris pigmentation is light and copper deposition is heavy.
Clinical Significance & Prevalence in Wilson Disease
| Clinical Presentation | KF Ring Prevalence |
|---|---|
| Neurological/psychiatric Wilson disease | >90–98% |
| Hepatic-only Wilson disease | 50–60% (may be absent in 40–60%) |
| Asymptomatic patients | Often absent |
A KF ring alone is not specific — it can rarely occur in other cholestatic liver diseases (primary biliary cholangitis/PBC, PSC, familial cholestatic syndromes, chronic active hepatitis, multiple myeloma), usually with normal serum ceruloplasmin.
Other Ocular Finding: "Sunflower" Cataract
Copper deposition under the anterior lens capsule produces a ring/stellate yellow-brown opacity. It does not impair vision and, like the KF ring, resolves with chelation therapy.
Differential Diagnosis of Peripheral Corneal Rings
- Arcus senilis: White/gray lipid ring, separated from limbus by 1 mm of clear cornea; initially appears superiorly/inferiorly
- Chalcosis: Copper from a retained intraocular foreign body; deposition is more diffuse
- KF-like ring: Rare in PBC, PSC, multiple myeloma — ceruloplasmin usually normal
Diagnostic Workup (when KF ring is seen)
- Serum ceruloplasmin (low in Wilson disease) and serum copper
- 24-hour urine copper (elevated)
- Liver biopsy if needed
- MRI brain — T2 hyperintensities in putamen, thalamus, midbrain, pons, cerebellum
Treatment & KF Ring Fate
Lifelong systemic therapy leads to resorption of the corneal copper and clearing of KF rings:
- Chelation: D-penicillamine or trientine (note: penicillamine can cause acute neurological worsening in 20–50% of neurological WD)
- Zinc salts: Reduce gut copper absorption; used for presymptomatic patients or maintenance
- Liver transplantation: For fulminant hepatic failure or refractory disease
Sources: Wills Eye Manual; Sleisenger & Fordtran's GI and Liver Disease; Bradley & Daroff's Neurology in Clinical Practice
NBIA
Finding Sources
Searching Images
NBIA neurodegeneration brain iron accumulation MRI eye of the tiger
Reading File
Reading File
Neurodegeneration with Brain Iron Accumulation (NBIA)
Formerly known as Hallervorden-Spatz disease
Overview
NBIA is a group of inherited neurodegenerative disorders characterized by pathological iron accumulation in the basal ganglia (particularly the globus pallidus and substantia nigra). Clinical features include progressive dystonia, parkinsonism, spasticity, neuropsychiatric abnormalities, and often retinal degeneration. Onset is typically in childhood but adult-onset cases occur.
Key Subtypes & Genetics
| Subtype | Gene | Chromosome | Key Features |
|---|---|---|---|
| PKAN (Pantothenate Kinase-Associated Neurodegeneration) — most common, ~50% | PANK2 | 20 | Childhood dystonia, gait disorder, rigidity, dysarthria, spasticity, dementia, retinitis pigmentosa, optic atrophy; "Eye of the Tiger" sign on MRI |
| PLAN (PLA2G6-Associated Neurodegeneration) | PLA2G6 | 22q13.1 | Axial hypotonia, spasticity, bulbar dysfunction, ataxia, dystonia; or adult-onset levodopa-responsive dystonia-parkinsonism |
| MPAN (Mitochondrial Membrane Protein-Associated Neurodegeneration) | C19orf12 | — | Juvenile-onset levodopa-responsive parkinsonism, progressive dystonia-parkinsonism, optic atrophy, axonal motor neuropathy |
| Neuroferritinopathy | FTL | — | Adult-onset, choreiform/dystonic movements |
| Aceruloplasminemia | CP (ceruloplasmin) | — | Anemia, iron overload, diabetes, dystonia, akinetic-rigid syndrome |
| BPAN (Beta-propeller Protein-Associated) | WDR45 | X-linked | Childhood seizures → adult parkinsonism-dementia; "halo sign" on T1 MRI |
| Kufor-Rakeb | ATP13A2 | — | Juvenile parkinsonism, supranuclear gaze palsy |
| Others | FA2H, COASY, DCAF17 | — | Various |
Pathology of PKAN (Classic NBIA)
- Gross: Brown discoloration of the globus pallidus interna (GPi) and substantia nigra pars reticulata (SNr) — from iron deposition
- Microscopic: Neuronal loss, gliosis, loss of myelinated fibers, axonal spheroids (swellings)
- Mechanism: PANK2 encodes pantothenate kinase, a key regulatory enzyme in coenzyme A synthesis. Its dysfunction leads to cysteine accumulation, which chelates iron and generates free radicals
MRI — The "Eye of the Tiger" Sign (PKAN)

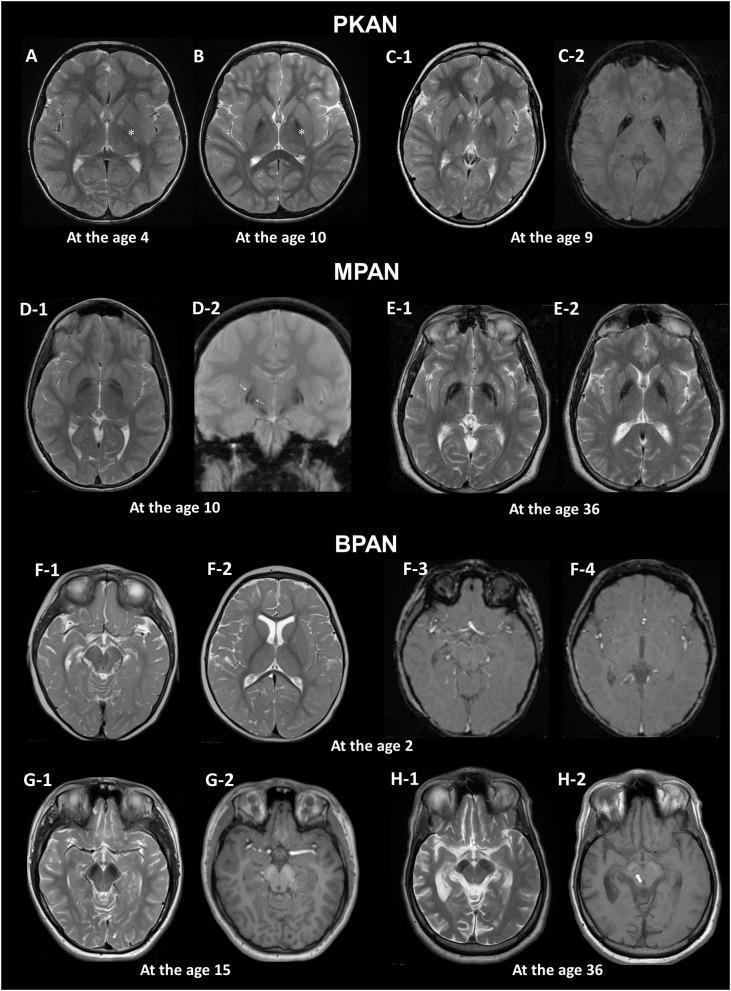
On T2-weighted MRI:
- Central hyperintensity in the anteromedial globus pallidus (gliosis, vacuolization, neuronal loss)
- Surrounded by a rim of hypointensity in the lateral globus pallidus (iron deposition)
- Together resembling the eye of a tiger
- Best seen on T2, GRE, or SWI sequences*
⚠️ The "eye of the tiger" sign is pathognomonic for PKAN, but not all NBIA subtypes show this pattern. Different subtypes have characteristic distributions (e.g., BPAN shows a T1 "halo sign" in substantia nigra; neuroferritinopathy and Kufor-Rakeb affect putamen/caudate).
Clinical Course of PKAN
- Typical PKAN: Childhood onset (mean age ~3–4 yrs), rapid progression → death in early childhood
- Atypical PKAN: Later onset (teen or adult), slower progression, speech difficulty prominent, psychiatric features
- Features: dystonia → rigidity → spasticity → dementia → retinitis pigmentosa/optic atrophy
Diagnosis
- MRI brain (T2/T2*/SWI): Eye of the tiger sign (PKAN) or subtype-specific iron distribution
- Genetic testing: PANK2 sequencing first; gene panel if negative
- Ophthalmology: retinitis pigmentosa assessment
- EMG/NCS: axonal neuropathy in some subtypes
Treatment
- No disease-modifying therapy established
- Iron chelation (deferiprone): may slow progression — not yet definitively proven
- Fosmetopentanat (phosphopantothenic acid prodrug): replenishes phosphopantothenic acid in PKAN; early reports show regression of symptoms
- Symptomatic: anticholinergics, baclofen, botulinum toxin, deep brain stimulation (DBS) for dystonia
- Levodopa: useful in PLAN and MPAN subtypes with parkinsonism
Sources: Bradley & Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22E (2025)
Complicated HSP
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.