Pleural effusion
Reading File
Finding Sources
Searching PubMed
"pleural effusion" diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, well-sourced overview of pleural effusion.
Pleural Effusion
Definition and Normal Physiology
A pleural effusion is an abnormal accumulation of fluid in the pleural space - the potential space between the visceral and parietal pleura. Under normal conditions, pleural fluid is produced from systemic capillaries at the parietal pleural surface and absorbed via pulmonary capillaries at the visceral surface. Approximately 1 L traverses the pleural space every 24 hours, but the net accumulation is only about 0.1-0.2 mL/kg body weight - clinically insignificant. Effusion develops when influx exceeds efflux.
- ROSEN's Emergency Medicine, p. 988-989
Causes
Transudates
Caused by elevated hydrostatic pressure or decreased oncotic pressure, with intact capillary permeability:
| Category | Examples |
|---|---|
| Elevated hydrostatic pressure | CHF, constrictive pericarditis, SVC obstruction, pulmonary embolism, renal failure, atelectasis |
| Decreased oncotic pressure | Hypoalbuminemia, nephrotic syndrome, cirrhosis with ascites, peritoneal dialysis, malnutrition |
| Miscellaneous | Myxedema, urinothorax |
Exudates
Caused by inflammation, infection, infiltration, or malignancy leading to increased capillary permeability:
- Infections: bacterial pneumonia (parapneumonic effusion), lung abscess, TB, viral illness, bronchiectasis
- Malignancy: metastatic lung cancer (40% of malignant effusions, 80% adenocarcinoma), breast cancer (2nd most common), non-Hodgkin lymphoma (most common in patients <30 years)
- Connective tissue disease: rheumatoid arthritis, SLE
- Abdominal/GI disorders: pancreatitis, subphrenic abscess, esophageal rupture
- Miscellaneous: pulmonary infarction, uremia, drug reactions, chylothorax
Note: Pulmonary embolism can cause both transudates (elevated pulmonary vascular pressure) and exudates (ischemia and pleural membrane inflammation).
- Fischer's Mastery of Surgery, p. 2428-2430; ROSEN's Emergency Medicine, p. 988-989
The most common causes in the US are congestive heart failure, malignancy, bacterial pneumonia, and pulmonary embolism. TB remains a leading cause in endemic regions.
Pathophysiology
Transudates are ultrafiltrates of plasma containing very little protein. CHF is the most common cause.
Exudates contain relatively high protein, reflecting intrinsic pleural abnormality. As exudative effusions are resorbed, fibrinous tissue left behind can cause ongoing inflammation and pleural adhesions.
Massive effusions (>1.5-2 L) are usually malignant but can also arise from heart failure. They restrict respiratory movement, compress lung parenchyma, and cause intrapulmonary shunting. In rare cases, a tension hydrothorax can develop with mediastinal shift and circulatory compromise.
- ROSEN's Emergency Medicine, p. 989
Clinical Features
Symptoms:
- Pleuritic chest pain (sharp, worse with deep breathing) or ipsilateral shoulder pain from pleural inflammation
- Small effusions are typically asymptomatic
- Dyspnea generally does not develop until pleural fluid volume reaches at least 500 mL in adults
- Severity correlates with effusion size and underlying cause
Physical findings:
-
Diminished/absent breath sounds over the effusion
-
Dullness to percussion
-
Decreased tactile fremitus
-
Egophony and enhanced breath sounds at the superior border (overlying atelectatic lung)
-
A pleural friction rub may be present with isolated pleurisy
-
Massive effusions can cause hemodynamic compromise
-
ROSEN's Emergency Medicine, p. 989
Imaging
Chest X-ray
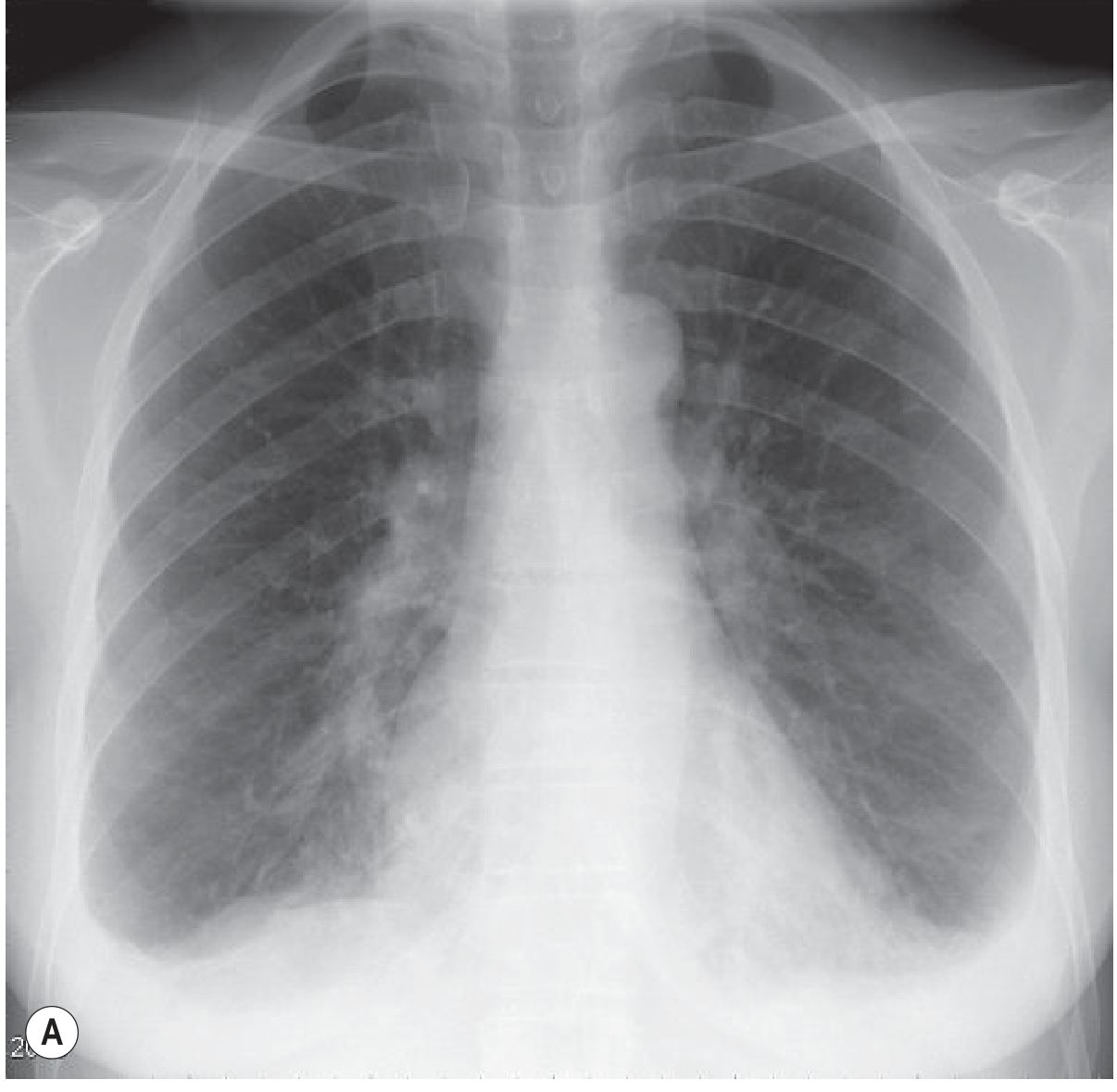
- Requires ~200 mL to be visible on upright PA film (blunting of costophrenic angle)
- Smaller amounts may be seen on the lateral projection in the posterior costophrenic gutter
- Classic appearance: blunting of costophrenic angle, concave upper meniscus (higher laterally), hemidiaphragm obscuration
- Large effusions completely opacify a hemithorax
- Supine films: fluid layers posteriorly - look for diffuse hazy opacity, apical capping, obscured diaphragm, widened minor fissure, paraspinal widening; costophrenic angles may appear clear
- Subpulmonary effusion: mimics "high hemidiaphragm," peaks more laterally than usual, straight medial segment
- Massive effusion with mediastinal shift towards the opposite side suggests no underlying collapse (in contrast to complete atelectasis, where shift is ipsilateral)
Ultrasound
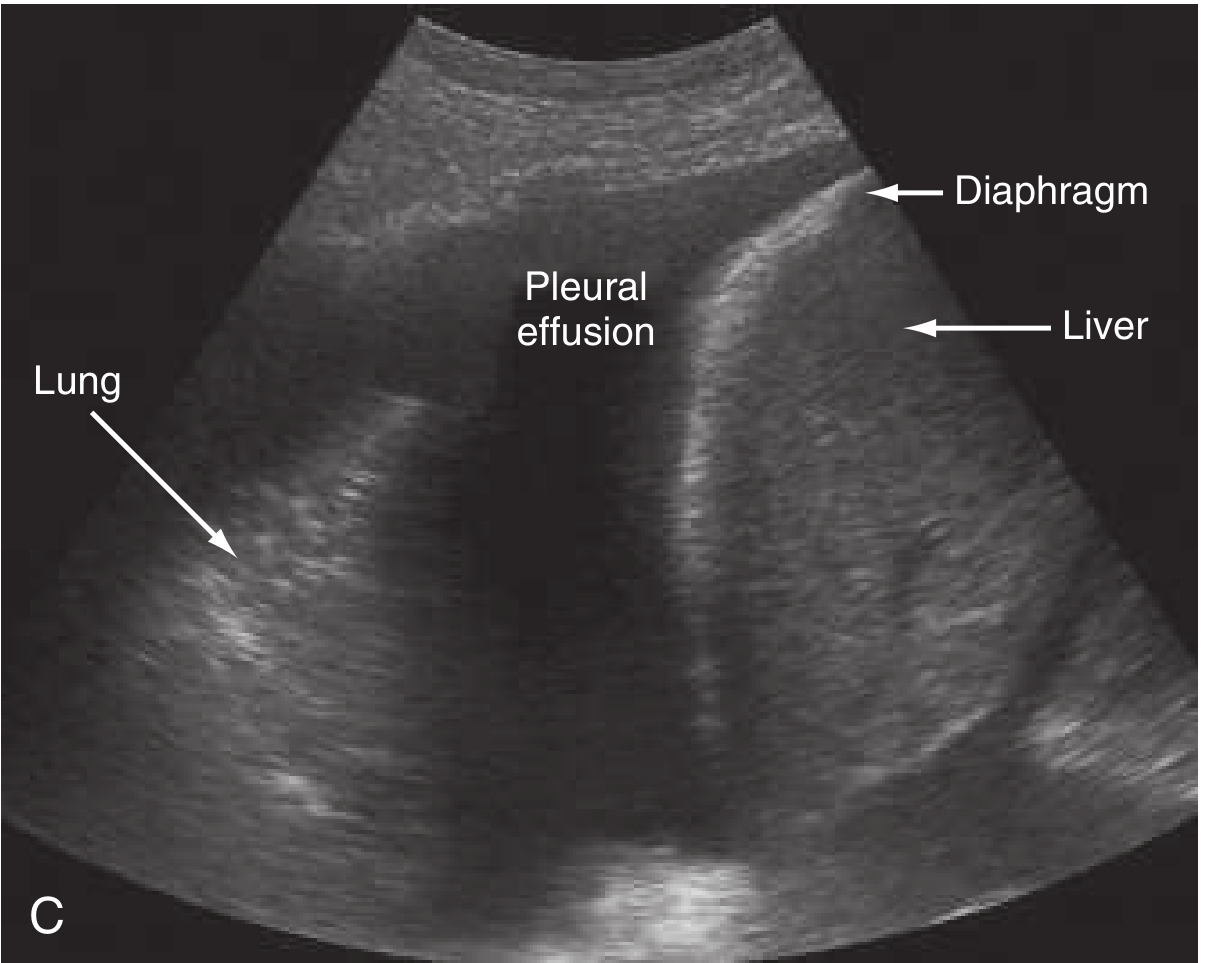
- More sensitive than CXR; can detect as little as 50 mL
- Transudates are typically anechoic
- Exudates/haemorrhagic effusions may be echogenic, with pleural thickening; may show homogeneous, complex, or septated patterns
- Distinguish from solid lesions by: shape change with breathing, septa/fibrous strands, movement of components
- Used for guidance of thoracentesis and biopsy
CT Scan
-
Detects as little as 3-5 mL - gold standard for small effusions
-
Distinguishes pleural from parenchymal disease; identifies underlying cause (malignancy, PE, pneumonia)
-
Essential for localizing loculated effusions before drainage
-
Differentiates empyema from lung abscess
-
Grainger & Allison's Diagnostic Radiology; ROSEN's Emergency Medicine, p. 989-990
Diagnostic Workup
When to Perform Thoracentesis
Most patients with an unexplained effusion should undergo diagnostic thoracentesis. Exceptions include clinically obvious transudates (e.g., bilateral effusions in known CHF) where it is unlikely to change management.
Pleural Fluid Analysis
Light's Criteria - the most widely accepted method for classifying transudates vs. exudates. A pleural effusion is an exudate if ANY one of the following is met:
| Criterion | Threshold |
|---|---|
| Pleural fluid protein / serum protein | >0.5 |
| Pleural fluid LDH / serum LDH | >0.6 |
| Pleural fluid LDH | >2/3 of upper limit of normal serum LDH |
Caveat: Light's criteria can misclassify up to 20% of transudates as exudates ("pseudo-exudates"). In these cases, a serum-to-pleural fluid albumin gradient >1.2 g/dL corrects the diagnosis back to transudate.
Additional pleural fluid tests:
| Test | Significance |
|---|---|
| pH <7.2 | Infection/inflammation; typically parapneumonic |
| pH <7.0 | Strongly suggests empyema or esophageal rupture - indicates tube thoracostomy |
| pH <7.3 | Parapneumonic effusion, malignancy, rheumatoid effusion, TB, systemic acidosis |
| Glucose <60 mg/dL | Lupus, TB, malignancy, esophageal perforation |
| Glucose <30 mg/dL | Rheumatoid arthritis, empyema |
| Elevated amylase | Pancreatitis, esophageal leak (salivary amylase), malignancy |
| Triglycerides elevated | Chylothorax |
| ADA elevated | Tuberculosis |
| Bloody fluid (Hct >50% peripheral blood) | Hemothorax (trauma, spontaneous tumor rupture) |
| Calretinin positive | Mesothelioma |
| Cytology | Malignant effusion (sensitivity independent of fluid volume) |
Routine tests should include: pH, protein, LDH, albumin, amylase, glucose, triglycerides, ADA, culture, cell count, and cytology.
Despite full investigation, etiology remains unknown in up to 25% of cases.
- Fischer's Mastery of Surgery, p. 2430; ROSEN's Emergency Medicine, p. 990
Simple vs. Complex (Loculated) Effusions
- Simple/free-flowing: layers dependently on supine or decubitus imaging; generally transudative
- Complex/loculated: walled off by adhesions or fibrous tissue; unilocular or multilocular; most commonly infectious or malignant
- Loculated effusions within interlobar fissures can mimic a mass lesion ("pseudotumour" or "vanishing tumour" when transudative)
Management
The primary treatment is always treatment of the underlying cause.
Emergent/Urgent Indications for Drainage
- Massive effusion (>1.5-2 L) causing respiratory or hemodynamic compromise
- Empyema - requires timely chest tube drainage (small-bore pigtail catheters, 14 Fr, are now first-line per AATS guidelines; traditional large-bore 28-40 Fr tubes are also used)
- Esophageal rupture
- Tension hydrothorax
Approach by Type
| Effusion Type | Management |
|---|---|
| Transudative | Treat underlying cause (diuresis for CHF, albumin for nephrotic syndrome, etc.); thoracentesis if symptomatic relief needed |
| Parapneumonic (uncomplicated) | Antibiotics; monitor closely; drain if pH <7.2, glucose <60, or positive culture |
| Empyema | Chest tube drainage + antibiotics; intrapleural fibrinolysis (tPA/DNase) for complicated infections; surgery if fibrinolysis fails |
| Malignant | Therapeutic thoracentesis for symptomatic relief; recurrent effusions - chemical/mechanical pleurodesis or indwelling pleural catheter (IPC); pleuroperitoneal shunt in selected cases |
| Chylothorax | Dietary fat restriction, octreotide; surgery if persistent |
| Hemothorax | Chest tube; thoracotomy for massive or persistent bleeding |
Note on limits during thoracentesis: Removing >1.5 L at one time risks re-expansion pulmonary edema. Stop drainage if the patient develops chest tightness or cough.
- ROSEN's Emergency Medicine, p. 990-991; Fischer's Mastery of Surgery, p. 2431
Special Notes
-
Hypoxemia in pleural effusion is generally mild and results from a mildly elevated shunt (~6.9%). Large right-sided effusions can have hemodynamic effects similar to tamponade via direct compression of the right ventricle. Thoracentesis may not consistently improve PaO2 and can occasionally worsen it due to increased V/Q mismatch in previously atelectatic regions being reperfused.
-
An unexplained pleural effusion should always raise suspicion for malignancy and requires follow-up.
-
Murray & Nadel's Textbook of Respiratory Medicine; ROSEN's Emergency Medicine
Sources: Murray & Nadel's Textbook of Respiratory Medicine | ROSEN's Emergency Medicine (7th ed.) | Fischer's Mastery of Surgery (8th ed.) | Grainger & Allison's Diagnostic Radiology | Quick Compendium of Clinical Pathology (5th ed.)
Meaning of exudates and transudates with image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Now I have everything needed - clear pathological definitions from Robbins, diagnostic criteria from multiple sources, and two excellent diagrams. Let me compose the full answer.
Transudates and Exudates
The Core Distinction
Both transudates and exudates are extravascular fluids - fluid that has escaped from blood vessels into a body cavity or tissue. The fundamental difference is the mechanism by which they form:
| Transudate | Exudate | |
|---|---|---|
| Protein content | Low (protein-poor) | High (protein-rich) |
| Mechanism | Osmotic or hydrostatic imbalance across vessel wall | Increased vascular permeability due to inflammation |
| Capillary permeability | Normal (intact) | Increased/damaged |
| Nature | Ultrafiltrate of blood plasma | Active inflammatory secretion |
| Cells | Little or none | May contain leukocytes, cell debris, sometimes RBCs |
| Appearance | Clear, straw-colored | Cloudy, turbid, or bloody |
From Robbins & Kumar Pathologic Basis of Disease (the gold-standard pathology definition):
"A transudate is a fluid with low protein content (most of which is albumin) and little or no cellular material. It is essentially an ultrafiltrate of blood plasma produced as a result of osmotic or hydrostatic imbalance across the vessel wall without an increase in vascular permeability."
"An exudate is an extravascular fluid that has a high protein concentration and may contain cellular debris or blood cells. Its presence implies the existence of an inflammatory process that has increased the permeability of small blood vessels."
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 84
Mechanism - Why Does Each Form?
Transudate: A Pressure/Oncotic Problem
Fluid leaks out because the balance of forces pushing fluid out of (or keeping it in) capillaries is disturbed - but the capillary wall itself is intact.
Two main mechanisms:
- Increased hydrostatic pressure - higher pressure inside capillaries pushes fluid out (e.g., heart failure raising venous back-pressure)
- Decreased oncotic (colloid osmotic) pressure - normally, plasma proteins (especially albumin) pull water back into capillaries. When albumin is low (nephrotic syndrome, liver disease, malnutrition), this "pulling force" is lost and fluid leaks out
The capillary wall remains structurally normal - it simply cannot keep up with the altered pressures.
Exudate: An Inflammatory Problem
In inflammation, chemical mediators (histamine, bradykinin, leukotrienes, prostaglandins) cause vasodilation and increased vascular permeability - endothelial cell junctions loosen, gaps form, and the capillary wall becomes "leaky." Large molecules like proteins and even blood cells can now pass through freely. The result is protein-rich fluid flooding the tissue or cavity.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 84
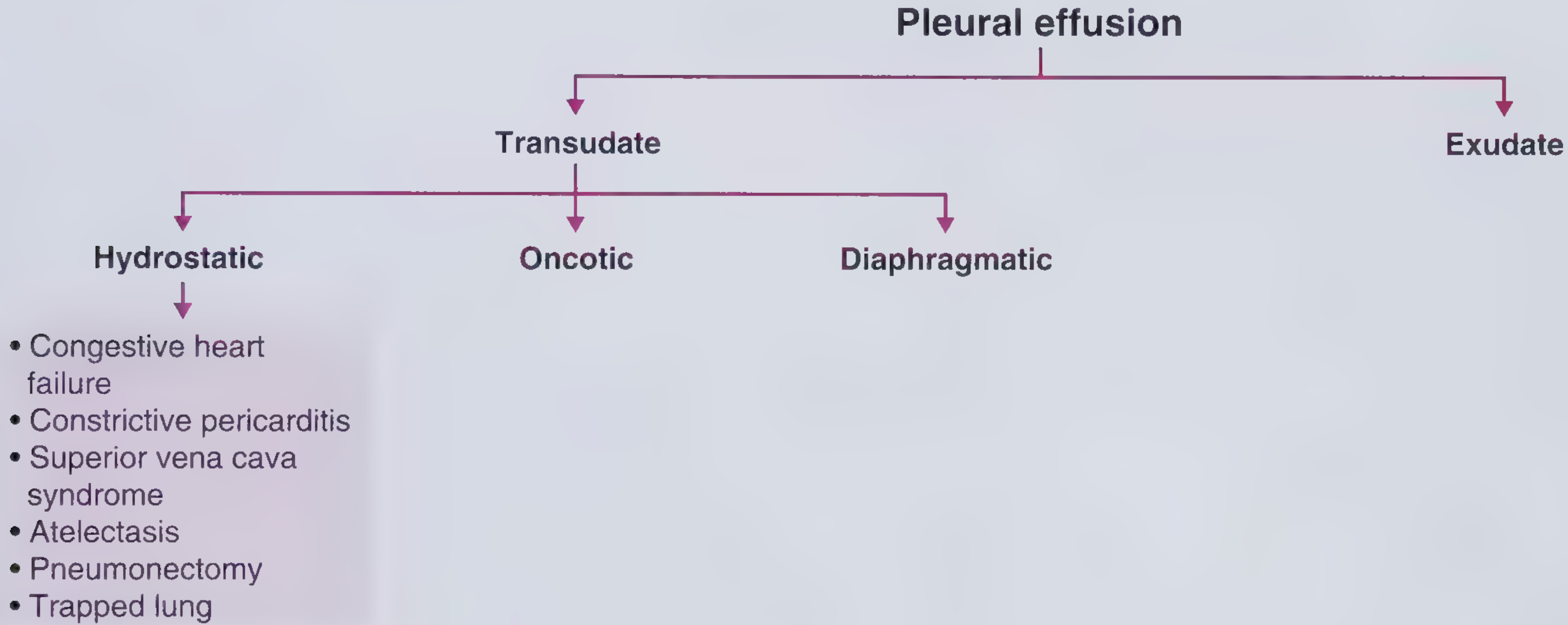
Classification Diagram
Common Causes
Transudates
| Mechanism | Causes |
|---|---|
| Increased hydrostatic pressure | Congestive heart failure, constrictive pericarditis, SVC obstruction, atelectasis, trapped lung, pneumonectomy |
| Decreased oncotic pressure | Nephrotic syndrome, cirrhosis with ascites, hypoalbuminemia, malnutrition, peritoneal dialysis |
| Diaphragmatic defects | Meigs syndrome (ovarian fibroma + ascites + effusion), peritoneal dialysis |
The three leading causes of transudates are: CHF, cirrhosis, and nephrotic syndrome. Transudates are usually bilateral because they arise from systemic conditions.
Exudates
| Category | Examples |
|---|---|
| Infections | Bacterial pneumonia (parapneumonic), empyema, TB, viral illness |
| Malignancy | Lung cancer, breast cancer, lymphoma, mesothelioma |
| Connective tissue disease | Rheumatoid arthritis (pH <7.2, glucose <30, LD >700), SLE |
| Abdominal | Pancreatitis (elevated amylase), subphrenic abscess, esophageal rupture |
| Vascular | Pulmonary embolism (can be either, but usually exudate) |
| Other | Uremia, drug reactions, Dressler syndrome, asbestos |
Exudates are more often unilateral due to a localized process.
- Henry's Clinical Diagnosis and Management by Laboratory Methods; Quick Compendium of Clinical Pathology (5th ed.)
Diagnostic Approach to Pleural Effusion
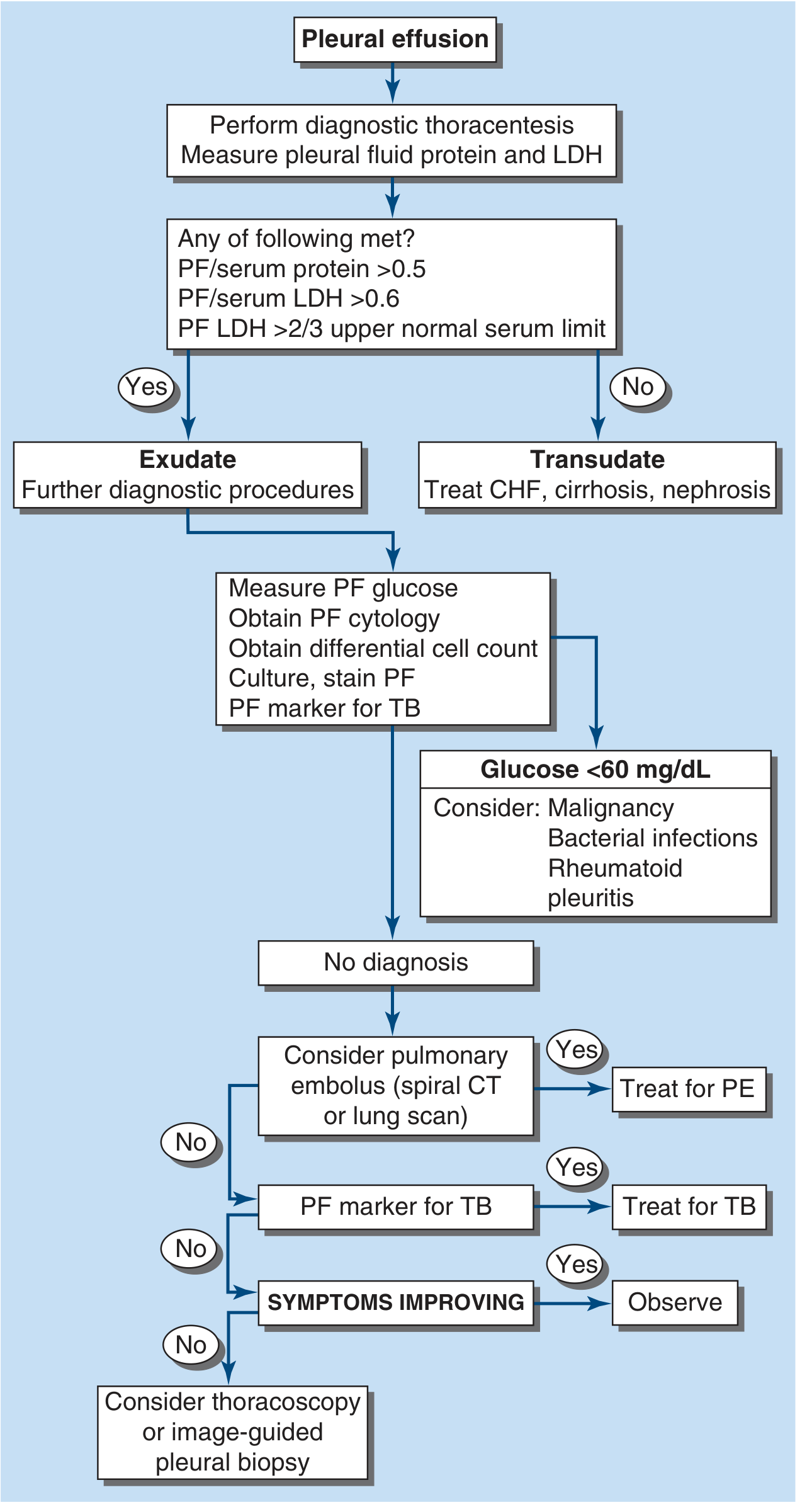
Light's Criteria - Distinguishing Exudate from Transudate
The standard laboratory method. A pleural effusion is classified as an exudate if ANY ONE of the three criteria is met:
| Criterion | Cut-off |
|---|---|
| Pleural fluid protein / serum protein | > 0.5 |
| Pleural fluid LDH / serum LDH | > 0.6 |
| Pleural fluid LDH | > 2/3 upper limit of normal serum LDH |
If none of the criteria are met → Transudate (no further fluid analysis needed; treat the underlying cause)
If any one is met → Exudate (further workup required: glucose, cytology, differential cell count, culture, Gram stain, TB markers)
Sensitivity ~98%, Specificity ~80%. The main pitfall: up to 25% of true transudates can be misclassified as exudates ("pseudoexudates") - most often when a patient with CHF has been diuresed, raising protein and LDH concentrations in the fluid.
Correction for pseudoexudates: If Light's criteria suggest exudate but the clinical picture strongly suggests CHF:
-
Serum albumin - pleural albumin > 1.2 g/dL → confirms transudate
-
Serum protein - pleural protein > 3.1 g/dL → confirms transudate
-
Pleural fluid NT-proBNP > 1500 pg/mL → confirms CHF-related transudate
-
Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis; Roberts and Hedges' Clinical Procedures in Emergency Medicine
Additional Fluid Markers That Help Identify the Cause
Once identified as an exudate, these markers narrow the differential:
| Finding | Suggests |
|---|---|
| WBC >100,000/mm³, pH <7.2, glucose low, bacteria | Empyema |
| Lymphocyte predominance, low/absent mesothelial cells, elevated ADA | Tuberculosis |
| Bloody, elevated amylase, abnormal cytology | Malignancy |
| Elevated amylase (salivary type), very low pH | Esophageal rupture |
| Elevated amylase (pancreatic type), left-sided | Pancreatitis |
| Elevated triglycerides, milky appearance | Chylothorax |
| pH <7.2, glucose <30, LD >700 | Rheumatoid arthritis |
| Eosinophilia (>10%) | Blood/air in pleural space, drug reactions |
In Simple Terms (Summary)
- Transudate = "plumbing problem" - the capillary wall is normal but the pressures are wrong (too much pressure pushing fluid out, or not enough protein pulling it back in). Fluid is thin and watery, low in protein.
- Exudate = "inflammation problem" - the capillary wall has been made leaky by disease/injury. Fluid is thick and protein-rich, often containing white cells or debris.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Harrison's Principles of Internal Medicine 22E | Henry's Clinical Diagnosis and Management by Laboratory Methods | Quick Compendium of Clinical Pathology (5th ed.) | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.