One lung ventilation - MD Anaesthesia Pg Exam - 30 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have sufficient comprehensive data from Miller's, Barash, and Morgan & Mikhail to write a complete 30-mark MD Anaesthesia PG exam answer.
One-Lung Ventilation (OLV)
MD Anaesthesia PG Examination Answer (30 Marks)
1. INTRODUCTION (2 marks)
One-lung ventilation (OLV) is a technique in which only one lung is mechanically ventilated while the other is deliberately collapsed and non-ventilated. It is the cornerstone of thoracic anaesthesia, providing optimal surgical access to the thoracic cavity while maintaining adequate gas exchange. The principal challenge is the development of a large obligatory right-to-left intrapulmonary shunt from the non-ventilated lung, which can cause significant hypoxaemia.
2. INDICATIONS FOR OLV (4 marks)
Indications are classified as absolute and relative.
Absolute Indications (Lung Isolation - to protect the other lung)
| Category | Examples |
|---|---|
| Prevention of contamination | Infection/abscess, massive haemoptysis, bronchopleural fistula, bronchopulmonary lavage (pulmonary alveolar proteinosis) |
| Control of ventilation distribution | Bronchopleural or bronchocutaneous fistula, giant lung cyst/bulla, tracheobronchial disruption, severe hypoxaemia from unilateral lung disease |
| Single-lung transplantation | To independently manage each lung separately |
Relative Indications (Lung Separation - to improve surgical exposure)
- Thoracic aortic aneurysm repair
- Pneumonectomy, lobectomy, segmentectomy
- Video-assisted thoracoscopic surgery (VATS), robotic thoracic surgery
- Oesophageal surgery
- Anterior thoracic spine surgery
- Minimally invasive cardiac surgery
(Barash 9e, Miller's 10e)
3. PHYSIOLOGICAL CHANGES DURING OLV (6 marks)
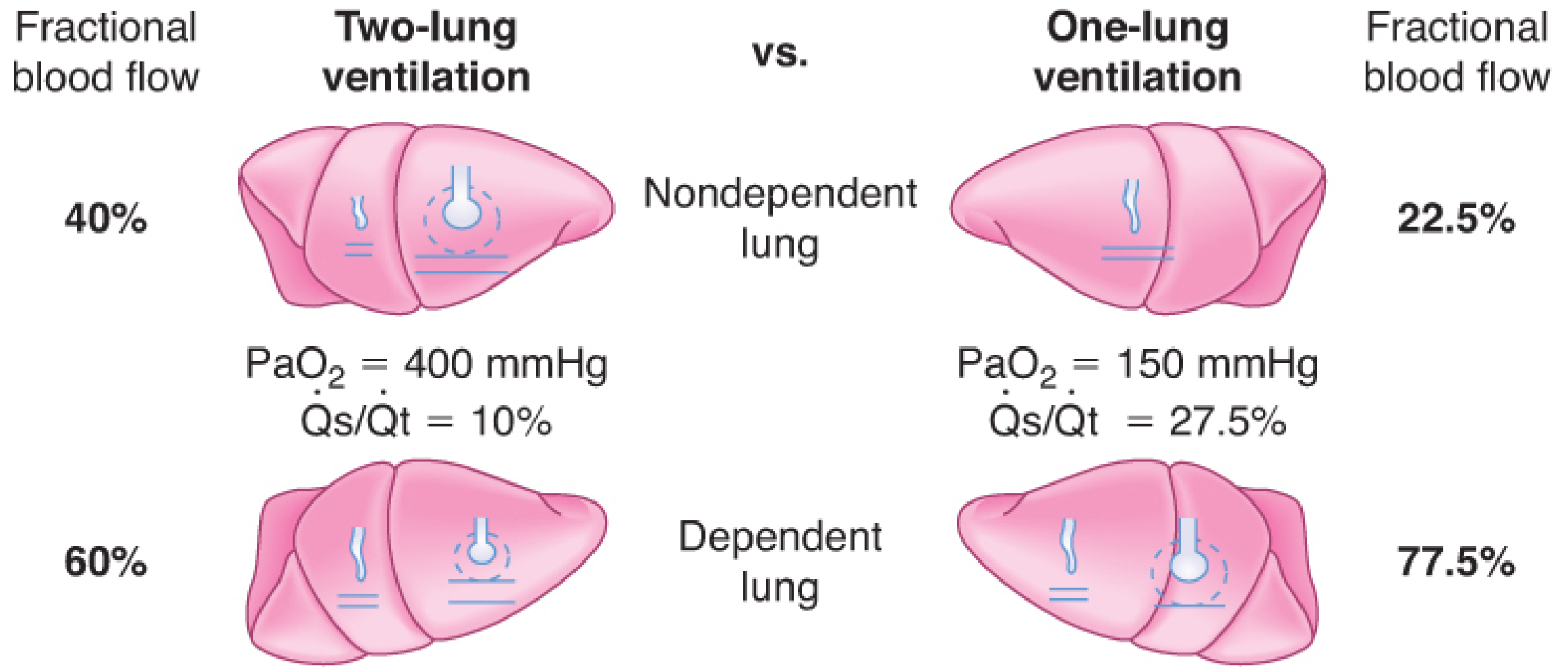
3a. Lateral Decubitus Position Effects (Two-Lung Ventilation)
In the lateral decubitus position with open chest:
- Ventilation preferentially goes to the dependent (lower) lung due to gravity and diaphragmatic mechanics
- Perfusion also preferentially goes to the dependent lung due to gravity (greater hydrostatic pressure)
- In the closed-chest lateral position, V/Q matching is relatively preserved
3b. Transition to OLV - The Shunt Problem
When the non-dependent (operative) lung is collapsed and non-ventilated, it continues to receive blood flow. This creates an obligatory right-to-left intrapulmonary shunt.
- During two-lung ventilation: Shunt fraction (Qs/Qt) ≈ 10% (5% per lung)
- During OLV: Shunt fraction rises to approximately 20-30%
- The non-dependent lung receives approximately 35-40% of total pulmonary blood flow
- This mixing of deoxygenated blood from the collapsed lung with oxygenated blood from the dependent lung widens the alveolar-arterial (A-a) O₂ gradient and causes hypoxaemia
3c. Hypoxic Pulmonary Vasoconstriction (HPV) - The Protective Mechanism
HPV is the intrinsic reflex vasoconstriction of pulmonary vessels in response to alveolar hypoxia. It is the most important compensatory mechanism during OLV.
- HPV reduces blood flow to the non-ventilated lung by approximately 50% of its baseline perfusion
- This reduces the effective shunt from ~40% (if no HPV) to ~20-25%
- HPV develops over minutes (biphasic: early rapid phase within minutes, sustained phase over hours)
Factors that inhibit HPV (worsen hypoxaemia during OLV):
- Volatile anaesthetic agents (dose-dependent; halothane > enflurane > isoflurane ≈ sevoflurane ≈ desflurane)
- Pulmonary hypertension
- Hypocapnia / alkalosis
- High cardiac output / increased mixed venous PO₂
- Vasodilators: nitroglycerin, nitroprusside, nitric oxide, phosphodiesterase inhibitors (milrinone), calcium channel blockers
- β-adrenergic agonists
- Hypothermia
Factors that improve/protect HPV:
- Almitrine (pulmonary vasoconstrictor - augments HPV)
- TIVA (propofol-based)
- Normocarbia / mild hypocarbia
- Appropriate cardiac output
Factors that decrease blood flow to the ventilated (dependent) lung (indirectly worsen OLV oxygenation):
- High mean airway pressure (excessive PEEP, high tidal volumes, intrinsic PEEP)
- Low FiO₂ to ventilated lung (causing HPV there too)
- Vasoconstrictors acting more on normoxic than hypoxic vessels (Morgan & Mikhail 7e, Miller's 10e)
3d. CO₂ Elimination During OLV
Elimination of CO₂ is relatively preserved during OLV, provided minute ventilation is maintained. Arterial CO₂ is usually not significantly altered, since CO₂ is much more diffusible than O₂. The main concern is hypoxaemia, not hypercarbia.
4. TECHNIQUES FOR OLV (5 marks)
Four techniques can be used:
4a. Double-Lumen Endobronchial Tube (DLT) - Most Commonly Used
Characteristics:
- Two lumens: a longer endobronchial lumen (enters main bronchus) + a shorter endotracheal lumen (terminates in lower trachea)
- Two cuffs: endobronchial cuff + endotracheal cuff
- Designed specifically for left or right bronchus
- Available sizes: 35F, 37F, 39F, 41F (French); 28F and 32F for smaller patients
Left-sided vs Right-sided DLT:
- Left-sided DLT is preferred in most cases because the left main bronchus is longer (4-5 cm) and there is less risk of occluding the left upper lobe bronchus
- Right-sided DLT is used when left bronchial intubation is contraindicated (e.g., left pneumonectomy, left mainstem bronchus tumour, left main bronchus stenosis, thoracic aortic surgery compressing left main bronchus). It has a modified cuff with a ventilation slot for the right upper lobe
DLT Size Selection (based on patient parameters - Miller's 10e):
- Tracheal width on CXR or CT correlates with appropriate DLT size
- Generally: males ≥170 cm → 41F; males <170 cm → 39F; females ≥160 cm → 37F; females <160 cm → 35F
Advantages of DLT:
- Easy placement
- Can ventilate one or both lungs
- Can suction either lung
- Rapid switching between one- and two-lung ventilation
- Ability to apply CPAP/PEEP selectively
4b. Bronchial Blockers
Types include:
- Univent tube: Single-lumen ETT with a movable endobronchial blocker in a side channel; blocker is advanced under fiberoptic guidance
- Arndt wire-guided endobronchial blocker (Cook Critical Care): Guide wire loop snares FOB, directs blocker into desired bronchus
- Cohen Flexitip bronchial blocker: Flexion at tip directed using a wheel mechanism
- EZ-Blocker: Y-shaped, self-positioning at the carina
Advantages:
- Single-lumen tube remains in place (no tube change needed post-operatively)
- Useful in patients with difficult airways, tracheostomy
- Can be directed to specific lobar bronchi for selective lobar collapse
Disadvantages:
- More difficult to position (FOB required)
- Risk of displacement during surgery
- Limited suctioning capacity
- Not ideal for lung isolation (low-volume high-pressure cuffs less effective at preventing contamination)
4c. Endobronchial Intubation with Single-Lumen Tube
A conventional ETT can be advanced into a mainstem bronchus, but this is largely a historical/emergency technique with major limitations (no ability to ventilate both lungs, high risk of lobar collapse).
4d. Tubeless Techniques
Spontaneous breathing anaesthesia or high-frequency jet ventilation without intubation; reserved for specific VATS procedures.
(Morgan & Mikhail 7e, Barash 9e)
5. CONFIRMATION OF CORRECT DLT PLACEMENT (3 marks)
Clinical Method (3-step auscultation protocol for left-sided DLT):
Step 1 - Both cuffs deflated, ventilate through both lumens: Bilateral breath sounds confirm tracheal position.
Step 2 - Inflate tracheal cuff, clamp bronchial lumen connector, ventilate through tracheal lumen only: Breath sounds only on left side confirm bronchial lumen is in left main bronchus.
Step 3 - Unclamp both lumens, inflate bronchial cuff, clamp tracheal lumen, ventilate through bronchial lumen: Breath sounds only on left side (no right upper lobe sounds = correct; if right upper lobe sounds heard = tube not far enough into left bronchus).
Fiberoptic Bronchoscopy (Gold Standard)
FOB is the most reliable method and should be used routinely after DLT placement:
- Through the tracheal (right) lumen: should see carina with blue bronchial cuff visible just below the carina in the left main bronchus (not herniated over)
- Through the bronchial (left) lumen: should see left upper and left lower lobar orifices
Malposition Problems (6 types - Barash 9e):
- DLT directed to opposite main bronchus
- DLT advanced too far into one bronchus
- DLT not advanced far enough (bronchial lumen above carina)
- Right upper lobe orifice occluded by right-sided DLT
- Left upper lobe orifice obstructed by left-sided DLT
- Herniation of bronchial cuff over carina
6. VENTILATORY MANAGEMENT DURING OLV (4 marks)
Lung-Protective Ventilation Strategy
Earlier recommendations used the same tidal volumes as two-lung ventilation. Current evidence strongly recommends lung-protective ventilation:
| Parameter | Recommendation |
|---|---|
| Tidal volume (TV) | 4-6 mL/kg predicted body weight (NOT actual body weight) |
| FiO₂ | Start at 1.0; can reduce once haemoglobin saturation is stable |
| Respiratory rate | Adjusted to maintain normocarbia (PaCO₂ 35-45 mmHg) |
| PEEP | 5-8 cmH₂O to prevent dependent lung atelectasis (individualized based on FRC and compliance) |
| Peak airway pressure | Keep <35 cmH₂O |
| Plateau pressure | Keep <25 cmH₂O |
| Driving pressure | Keep <14 cmH₂O (Driving pressure = Plateau - PEEP) |
Rationale for low tidal volumes: The ventilated lung receives the entire cardiac output, making it susceptible to volutrauma/barotrauma. High tidal volumes can cause hyperperfusion injury to the dependent lung AND ischaemia-reperfusion injury to the non-ventilated lung upon re-expansion.
PEEP in OLV:
- PEEP improves oxygenation when the dependent lung FRC is below optimal
- Excessive PEEP increases dependent lung pulmonary vascular resistance, redirecting blood to the non-ventilated lung and worsening shunt
- Optimal PEEP is titrated to lowest driving pressure (individualised)
(Miller's 10e, Barash 9e, Morgan & Mikhail 7e)
7. MANAGEMENT OF HYPOXAEMIA DURING OLV (4 marks)
Hypoxaemia typically develops within 10-30 minutes of initiating OLV, reaching its nadir at 20-30 minutes. HPV gradually increases and oxygenation may stabilise or improve over 2 hours.
Step-wise Management (Miller's Box 49.12):
Immediate/Severe desaturation (SpO₂ <85% or precipitous fall):
- Resume two-lung ventilation - reinflate non-ventilated lung, deflate bronchial cuff. This is the first priority and necessitates temporary interruption of surgery.
Gradual desaturation (systematic approach):
- Confirm FiO₂ = 1.0 - Ensure oxygen delivery is maximal
- Check DLT/blocker position - Fiberoptic bronchoscopy to rule out malposition (this is a very common cause)
- Optimise cardiac output - Maintain adequate CO; neither too low (falls SvO₂) nor too high (inhibits HPV). Avoid inotropes (dopamine worsens PaO₂ at supranormal CO)
- Reduce volatile agent to <1 MAC (or switch to TIVA with propofol) - minimises HPV inhibition
- Apply CPAP to non-dependent/non-ventilated lung - 2-5 cmH₂O with 100% O₂; this is very effective, allows oxygen absorption through the non-ventilated lung without fully re-inflating it
- Apply PEEP to ventilated lung - 5-10 cmH₂O if not already applied (only if FRC is low)
- Recruitment manoeuvre to ventilated (dependent) lung - brief sustained inflation to recruit collapsed alveoli
- Selective partial ventilation strategies:
- Intermittent reinflation of non-ventilated lung (HPV more effective after repeated hypoxic exposure)
- Intermittent positive airway pressure (IPAP) to non-ventilated lung via filter device
- Selective lobar collapse only (blocker placed in ipsilateral lobe bronchus while rest of lung is ventilated)
- Surgical ligation of pulmonary artery (pneumonectomy cases) - eliminates shunt entirely
- Almitrine (pulmonary vasoconstrictor) - augments HPV; combination with inhaled NO improves oxygenation without systemic hypotension
- ECMO - last resort in refractory hypoxaemia
8. CHOICE OF ANAESTHETIC AGENTS (2 marks)
Volatile Anaesthetics:
- At ≤1 MAC, modern volatile agents (isoflurane, sevoflurane, desflurane) cause only ~20% inhibition of HPV - equivalent to a net 4% increase in Qs/Qt
- This is clinically insignificant in most patients
- Volatile agents have anti-inflammatory effects, reducing post-thoracotomy cytokine release
- Avoid nitrous oxide (N₂O): increases risk of post-thoracotomy atelectasis (51% vs 24% with air/O₂), raises pulmonary artery pressure, inhibits HPV, and can expand bullae/blebs
TIVA (Total Intravenous Anaesthesia):
- Propofol-based TIVA does not inhibit HPV and is preferred when:
- HPV preservation is critical (pre-existing pulmonary hypertension)
- Patient has received bleomycin (risk of oxygen toxicity)
- FiO₂ needs to be limited
- Addition of dexmedetomidine to volatile anaesthesia improves OLV oxygenation
Induction agents:
- Propofol or ketamine: both diminish bronchospasm (important as thoracic patients often have reactive airways)
- Avoid barbiturates, benzodiazepines, etomidate, or opioids alone for induction (no bronchodilatory effect)
- Sevoflurane: most potent bronchodilator among volatile agents
9. SPECIAL SITUATIONS (2 marks)
DLT or Bronchial Blocker?
- DLT is preferred when lung isolation is required (contamination risk): more reliable seal, better suctioning
- Bronchial blocker preferred for:
- Difficult airway (avoids tube change post-operatively)
- Tracheostomy patients
- Patients requiring post-operative ventilation (avoid tube change from DLT to SLT)
- Selective lobar collapse
- Paediatric patients (<12 years) - appropriate small-size blockers
Patient with Pre-existing Pulmonary Disease:
- Emphysema patients paradoxically tolerate OLV well (auto-PEEP from obstructed airways maintains FRC in dependent lung)
- Patients with good pre-operative spirometry tend to have worse OLV oxygenation (more collapse in dependent lung)
- Trauma patients with dependent lung contusion are particularly high risk
10. SUMMARY TABLE: KEY POINTS AT A GLANCE
| Feature | Key Fact |
|---|---|
| Shunt during OLV | 20-30% (vs 10% in two-lung) |
| HPV blood flow reduction | ~50% of non-ventilated lung flow |
| Preferred DLT | Left-sided in majority of cases |
| DLT confirmation standard | Fiberoptic bronchoscopy (gold standard) |
| Tidal volume during OLV | 4-6 mL/kg predicted body weight |
| First step in desaturation | Resume two-lung ventilation |
| Best intervention for ongoing desaturation | CPAP to non-ventilated lung + check DLT position |
| Volatile agents at 1 MAC | Only ~20% HPV inhibition; clinically acceptable |
| Avoid | N₂O, high tidal volumes, excessive PEEP |
| CO₂ during OLV | Usually maintained; hypoxaemia is the main concern |
References:
- Miller's Anesthesia, 10th Edition (Elsevier, 2020) - Chapter 49: Anesthesia for Thoracic Surgery
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition - Chapter 25: Thoracic Anesthesia
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Edition - Chapter 38: Anesthesia for Thoracic Surgery
This is a shared conversation. Sign in to Orris to start your own chat.