Squamous metaplasia
Reading File
Finding Sources
Searching PubMed
"squamous metaplasia" AND pathogenesis
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of squamous metaplasia from authoritative pathology and histology sources.
Squamous Metaplasia
Definition
Squamous metaplasia is the reversible replacement of one type of differentiated cell by stratified squamous epithelium in a location that normally contains a different epithelial type (usually columnar or transitional/urothelial). It is one of the most common forms of epithelial metaplasia and represents a cellular adaptive response to a sustained abnormal stimulus.
"Metaplasia is a reversible change in which one differentiated cell type (epithelial or mesenchymal) is replaced by another cell type. It often represents an adaptive response in which one cell type that is sensitive to a particular stress is replaced by another cell type that is better able to withstand the adverse environment."
- Robbins, Cotran & Kumar: Pathologic Basis of Disease
Schematic Diagram
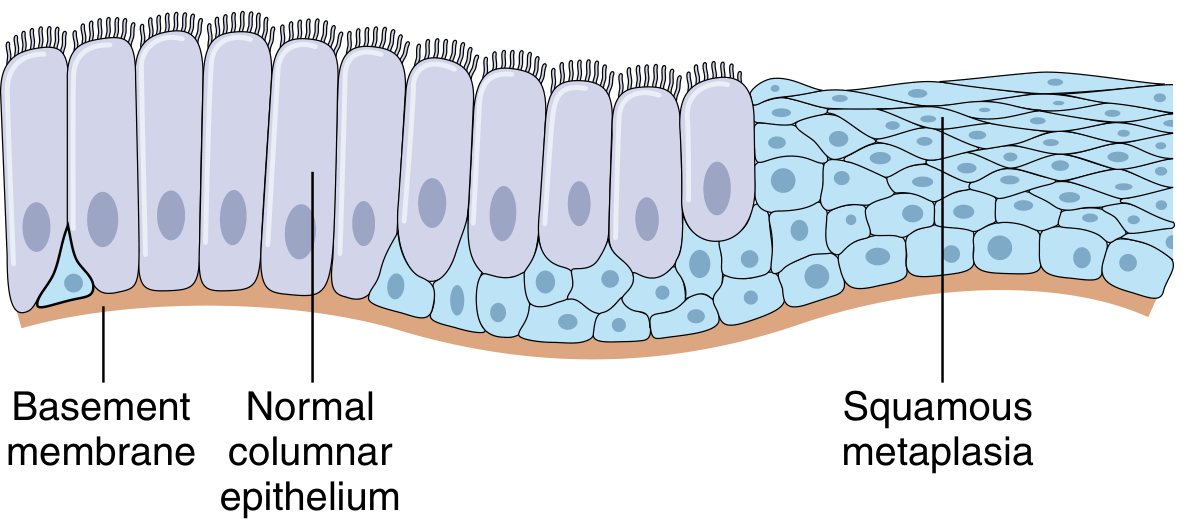
Columnar-to-squamous metaplasia: normal ciliated columnar cells (left) replaced by stratified squamous epithelium (right). - Robbins, Cotran & Kumar
Mechanism
Squamous metaplasia does not arise by direct transformation of one adult cell into another. Instead, it results from:
- Reprogramming of local tissue stem cells - Environmental signals (cytokines, growth factors, extracellular matrix components) alter gene expression in resident progenitor/stem cells, driving differentiation toward a squamous phenotype.
- Colonization by differentiated cells from adjacent areas (less common).
A key molecular mediator is retinoic acid (vitamin A). Retinoic acid regulates transcription via nuclear retinoid receptors, and both deficiency and excess of vitamin A can induce metaplastic change.
- Robbins, Cotran & Kumar: Pathologic Basis of Disease
Histology
Below is a photomicrograph of squamous metaplasia of the uterine cervix (H&E, x240). Note the island of stratified squamous epithelium surrounded on both sides by simple columnar epithelium:
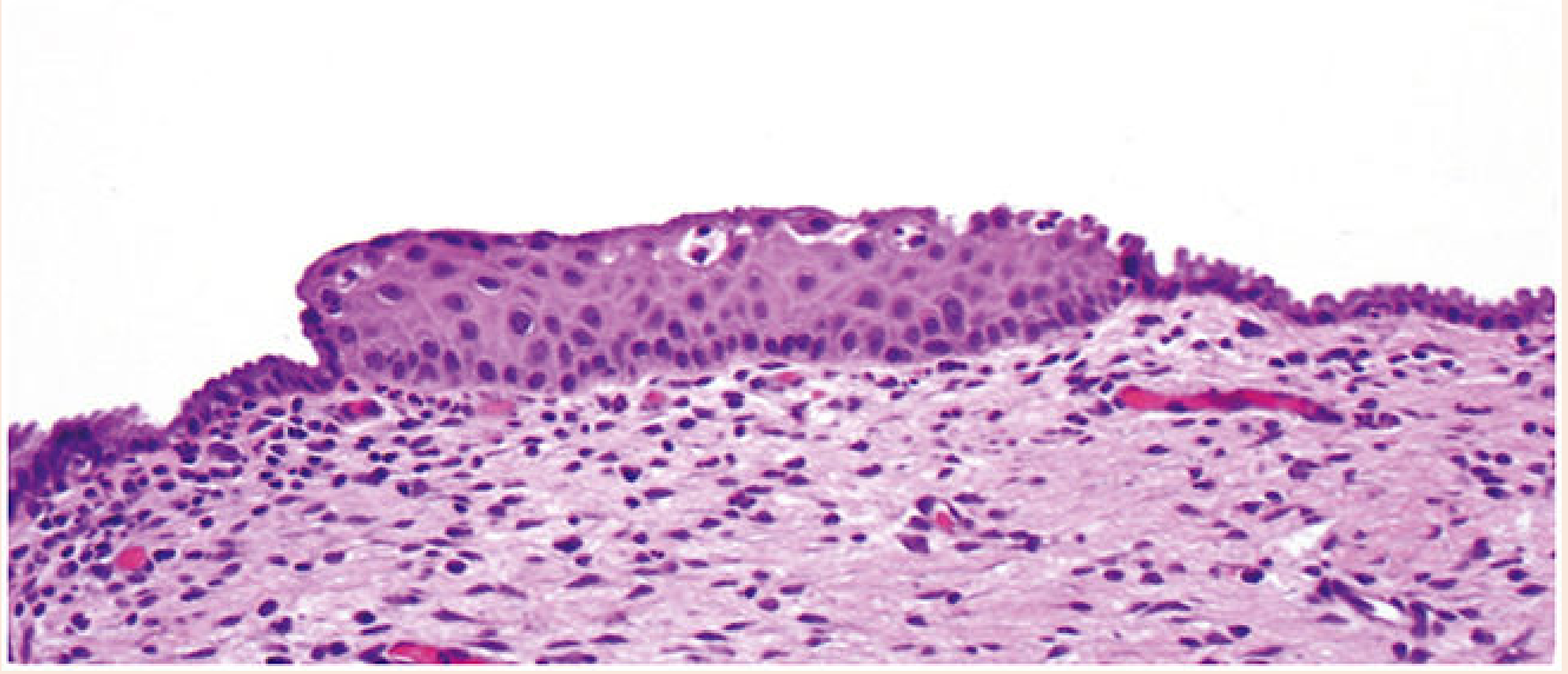
F5.1.1. Squamous metaplasia of the uterine cervix. - Histology: A Text and Atlas (Pawlina)
Common Sites and Causes
| Site | Stimulus/Cause | Notes |
|---|---|---|
| Respiratory tract (trachea, bronchi) | Chronic cigarette smoking, chronic coughing | Normal ciliated columnar cells replaced by stratified squamous; cilia and mucus secretion lost; risk of squamous cell carcinoma with persistent stimulation |
| Cervix (transformation zone) | Chronic irritation, HPV infection, normal physiological change | Columnar epithelium of ectocervix transforms to squamous; "ghost white" film on acetic acid application; most active during adolescence; site of cervical carcinogenesis |
| Urinary bladder (urothelium) | Chronic injury, bladder stones, schistosomiasis | Urothelium replaced by keratinizing or non-keratinizing squamous epithelium; extensive multifocal keratinizing squamous metaplasia is a precursor to squamous cell carcinoma |
| Lactiferous ducts (breast) | Cigarette smoking (>90% of cases), possibly vitamin A deficiency from tobacco toxins | Keratinizing squamous metaplasia extends into nipple duct; trapped keratin causes ductal dilation and rupture; presents as subareolar abscess (Zuska disease / recurrent subareolar abscess) |
| Excretory ducts (salivary glands, pancreas, bile ducts) | Stones causing chronic irritation and pressure | Normally secretory columnar epithelium replaced by squamous |
| Cornea/respiratory epithelium | Vitamin A (retinoic acid) deficiency | Can have serious functional consequences |
| Anal transformation zone | Similar process to cervix | Dysplastic changes can also occur here |
| Prostate | Diethylstilbestrol (DES) exposure | Requires intact stromal ESR1 signaling |
Key Concept: Adaptive but Costly
Squamous metaplasia trades function for durability:
- The new squamous epithelium is more resistant to physical stress and chemical insult
- But it loses key protective functions of the original epithelium (e.g., mucus secretion and ciliary clearance in the airways)
- It is therefore generally an undesirable adaptive change, not a beneficial one
Clinical Significance and Malignant Risk
Squamous metaplasia itself is not malignant. However:
- If the causative stimulus persists, metaplastic epithelium can undergo dysplastic transformation and progress to carcinoma in situ, and ultimately invasive squamous cell carcinoma.
- Classic example: chronic smokers develop squamous metaplasia in the bronchi -> squamous cell carcinoma of the lung
- Bladder schistosomiasis leads to squamous metaplasia -> squamous cell carcinoma of the bladder
- Cervical transformation zone metaplasia -> cervical dysplasia (CIN) -> cervical squamous cell carcinoma (especially with high-risk HPV)
"If the factors (i.e., tobacco smoking) that predispose to squamous metaplasia are not eliminated, the metaplastic epithelium may undergo malignant transformation. In this way, one of the two most common forms of cancer of the respiratory tract, squamous cell carcinoma, originates from squamous metaplastic cells."
- Histology: A Text and Atlas (Pawlina)
Reversibility
Squamous metaplasia is reversible if the causative stimulus is removed before dysplasia sets in. Once the irritant is eliminated, the epithelium can revert toward its original differentiated phenotype through normal stem cell-driven regeneration.
Squamous Metaplasia vs. Dysplasia
| Feature | Squamous Metaplasia | Dysplasia |
|---|---|---|
| Cell arrangement | Orderly, normal layering | Disorganized |
| Nuclear morphology | Normal | Pleomorphism, hyperchromasia |
| Mitoses | Normal (basal) | Abnormal, increased |
| Reversibility | Yes | Potentially |
| Malignant potential | Not intrinsically | Yes (precancerous) |
Sources:
- Robbins, Cotran & Kumar: Pathologic Basis of Disease (Pathologic Basis of Disease)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina)
- Pfenninger and Fowler's Procedures for Primary Care
Neoplastic and non Neoplastic diseases of the cervix
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a thorough, textbook-based overview of neoplastic and non-neoplastic diseases of the cervix.
Diseases of the Cervix: Neoplastic and Non-Neoplastic
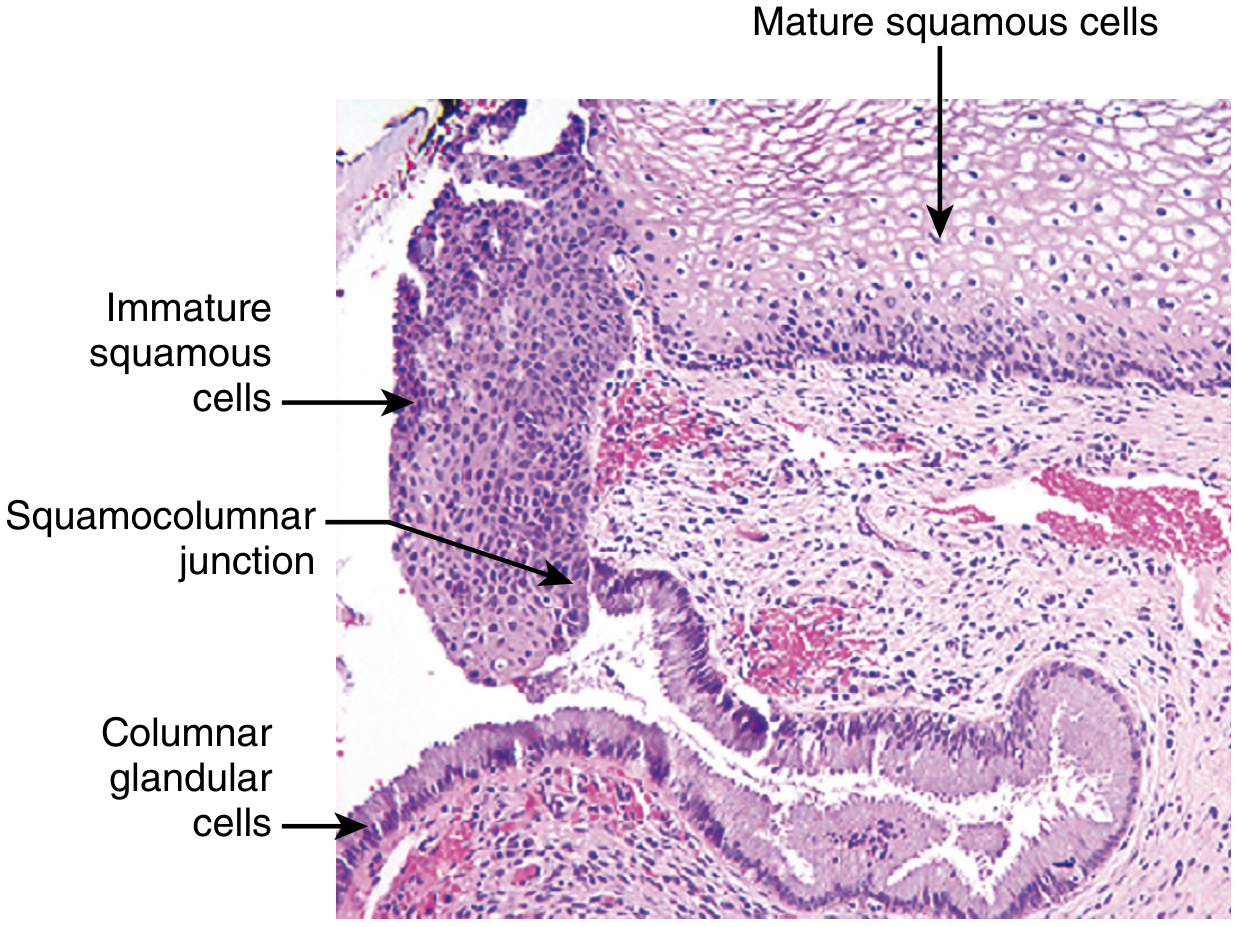
ANATOMY REVIEW (Context)
The cervix has two distinct epithelial zones:
- Ectocervix - covered by mature stratified squamous epithelium; visible on vaginal examination
- Endocervical canal - lined by columnar, mucus-secreting epithelium
- Squamocolumnar junction (SCJ) - the meeting point; its position varies with age and hormonal status
- Transformation zone (TZ) - the area where columnar epithelium undergoes squamous metaplasia; this is the most HPV-susceptible region and the site where virtually all precancerous and cancerous lesions arise
NON-NEOPLASTIC DISEASES
1. Cervicitis
Etiology
Cervicitis is extremely common. It can be infectious or noninfectious. Normal flora (streptococci, staphylococci, enterococci, E. coli, Candida) are frequently present. Sexually transmitted organisms causing significant disease include:
| Organism | Notes |
|---|---|
| Chlamydia trachomatis | Most common STI pathogen; up to 40% of STI clinic cervicitis cases |
| Neisseria gonorrhoeae | Causes acute purulent cervicitis |
| Herpes simplex virus 2 (HSV-2) | Maternal-infant transmission during birth can be fatal to neonate |
| Trichomonas vaginalis | Common; identified on Pap test |
| Mycoplasma/Ureaplasma | Associated with upper genital tract disease |
| HPV (certain types) | Also causes condyloma and neoplastic changes |
Pathogenesis
Estrogen at menarche promotes glycogen accumulation in squamous cells. Shed cells provide substrate for lactobacilli, which maintain vaginal pH <4.5 via lactic acid and H₂O₂ production. Disruption of this environment (alkaline pH from bleeding, intercourse, douching, or antibiotics) allows overgrowth of pathogens.
Clinical Features
- Purulent or mucopurulent vaginal discharge
- May cause abnormal Pap test results due to reactive epithelial changes
- Treatment: empiric antibiotics active against chlamydia and gonococcus; nucleic acid amplification tests (NAATs) on vaginal fluid
2. Endocervical Polyp
- Common benign exophytic growths arising from the endocervical canal
- Range from small sessile lesions to large masses protruding through the cervical os
- Histology: fibrous stroma covered by mucus-secreting endocervical glands with inflammation
- Clinical significance: may cause irregular vaginal spotting/bleeding, raising suspicion of a serious lesion; however, they have no malignant potential
- Treatment: simple curettage or surgical excision is curative
NEOPLASTIC DISEASES
Overview: The HPV-Carcinogenesis Axis
Virtually all cervical carcinomas are caused by oncogenic (high-risk) HPV strains. The transformation zone, with its large areas of immature metaplastic squamous epithelium, is particularly vulnerable to HPV infection.
Key HPV Biology
- HPV-16: accounts for ~60% of cervical cancer cases
- HPV-18: accounts for ~10% of cases
- Low-risk types (6, 11): cause condyloma acuminatum, not cancer
Molecular Mechanism of HPV Carcinogenesis
HPV carcinogenesis depends on two viral oncoproteins:
- E7 - binds and promotes proteasomal degradation of RB (retinoblastoma protein); also binds and inhibits p21 and p27 (CDK inhibitors) → cell cycle progression despite DNA damage
- E6 - binds and promotes proteasomal degradation of p53 (in high-risk HPVs only); also upregulates telomerase → cellular immortalization
In most cancers, HPV DNA integrates into the host genome, which:
- Disrupts the HPV gene that negatively regulates E6/E7 → increased E6/E7 expression
- Increases genomic instability → acquisition of additional pro-oncogenic mutations
Co-factors that aid progression: cigarette smoking, immunocompromise (immune surveillance plays a role in clearing HPV)
3. Squamous Intraepithelial Lesion (SIL) / Cervical Intraepithelial Neoplasia (CIN)
Classification - Two Systems in Use
| Two-tier (Bethesda) | Three-tier (CIN) | Biology |
|---|---|---|
| LSIL (Low-grade SIL) | CIN I | Productive HPV infection; koilocytic change; mild dysplasia confined to lower 1/3 of epithelium |
| HSIL (High-grade SIL) | CIN II | Dysplasia occupying lower 2/3 of epithelium; reduced viral replication; high proliferation |
| HSIL (High-grade SIL) | CIN III / CIS | Full-thickness epithelial involvement; carcinoma in situ; highest malignant potential |
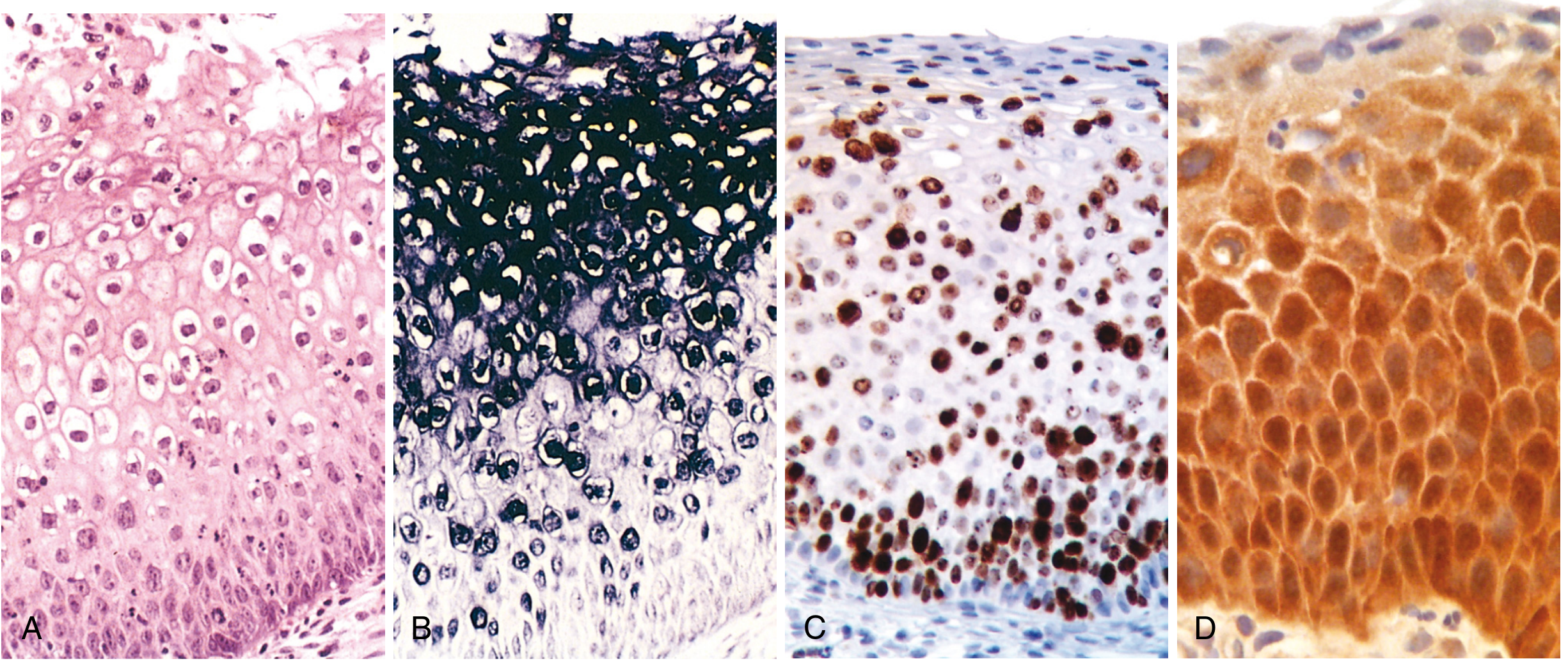
Morphology
- LSIL/CIN I: Dysplastic changes in the lower 1/3 of epithelium + koilocytic change (nuclear enlargement, perinuclear "halos") in superficial layers - indicates productive HPV replication
- HSIL/CIN II-III: Immature atypical cells extend into the upper 2/3 or full thickness; nuclear pleomorphism, hyperchromasia, increased mitoses; koilocytic change absent or minimal
Natural History (2-year follow-up data)
| Lesion | Regress | Persist | Progress |
|---|---|---|---|
| LSIL (CIN I) | 60% | 30% | 10% to HSIL |
| HSIL (CIN II/III) | 30% | 60% | 10% to carcinoma (over 2-10 years) |
- LSIL is NOT considered premalignant - majority regress spontaneously
- HSIL is precancerous - arrested maturation, high proliferation, integration of virus
- ~20% of HSIL develops de novo, not from preexisting LSIL
- Progression to invasive carcinoma, when it occurs, takes decades on average
Diagnosis and Screening
- Pap (Papanicolaou) test: cells scraped from transformation zone; most successful cancer screening test ever developed; has reduced cervical cancer mortality by 75% in the US
- HPV DNA testing: highly sensitive; most useful in women ≥30 years (negative test at this age confers ~5-year low risk); less useful <30 due to high HPV prevalence
- Colposcopy + biopsy: for abnormal Pap/HPV results
- HPV vaccination: Quadrivalent (types 6, 11, 16, 18) and 9-valent vaccines; recommended at ages 11-12; 81% drop in HPV infections and 40% reduction in SIL reported with vaccination
4. Invasive Cervical Carcinoma
Epidemiology
- 4th most common cancer in females worldwide (~604,000 new cases in 2020; >50% fatal)
-
85% of cases in resource-limited countries (lack of screening)
- Peak age: ~45-50 years (10-15 years after peak of SIL at ~30 years)
- US: 75% mortality decline since screening began; >50% of invasive cancers occur in unscreened women
Histologic Subtypes
| Type | Frequency | HPV | Notes |
|---|---|---|---|
| Squamous cell carcinoma | ~80% | High-risk HPV | Keratinizing or non-keratinizing |
| Adenocarcinoma | ~15% | High-risk HPV | From adenocarcinoma in situ; proportion increasing |
| Adenosquamous carcinoma | Rare | High-risk HPV | Mixed malignant glandular + squamous; shorter progression time |
| Small cell neuroendocrine carcinoma | <5% | High-risk HPV | Very poor prognosis; resembles small cell carcinoma of lung |
| Gastric-type HPV-independent adenocarcinoma | Rare | HPV-negative | Frequent STK11 and TP53 mutations; associated with Peutz-Jeghers syndrome |
Morphology
- Develops in the transformation zone
- Gross: fungating (exophytic) or infiltrating masses; "barrel cervix" when encircling the cervix
- Squamous cell carcinoma: nests and tongues of malignant squamous cells invading stroma; desmoplastic stromal response; keratinizing tumors form keratin pearls
- Adenocarcinoma: malignant endocervical glands with large hyperchromatic nuclei, mucin-depleted cytoplasm (dark appearance vs. normal pale endocervix)
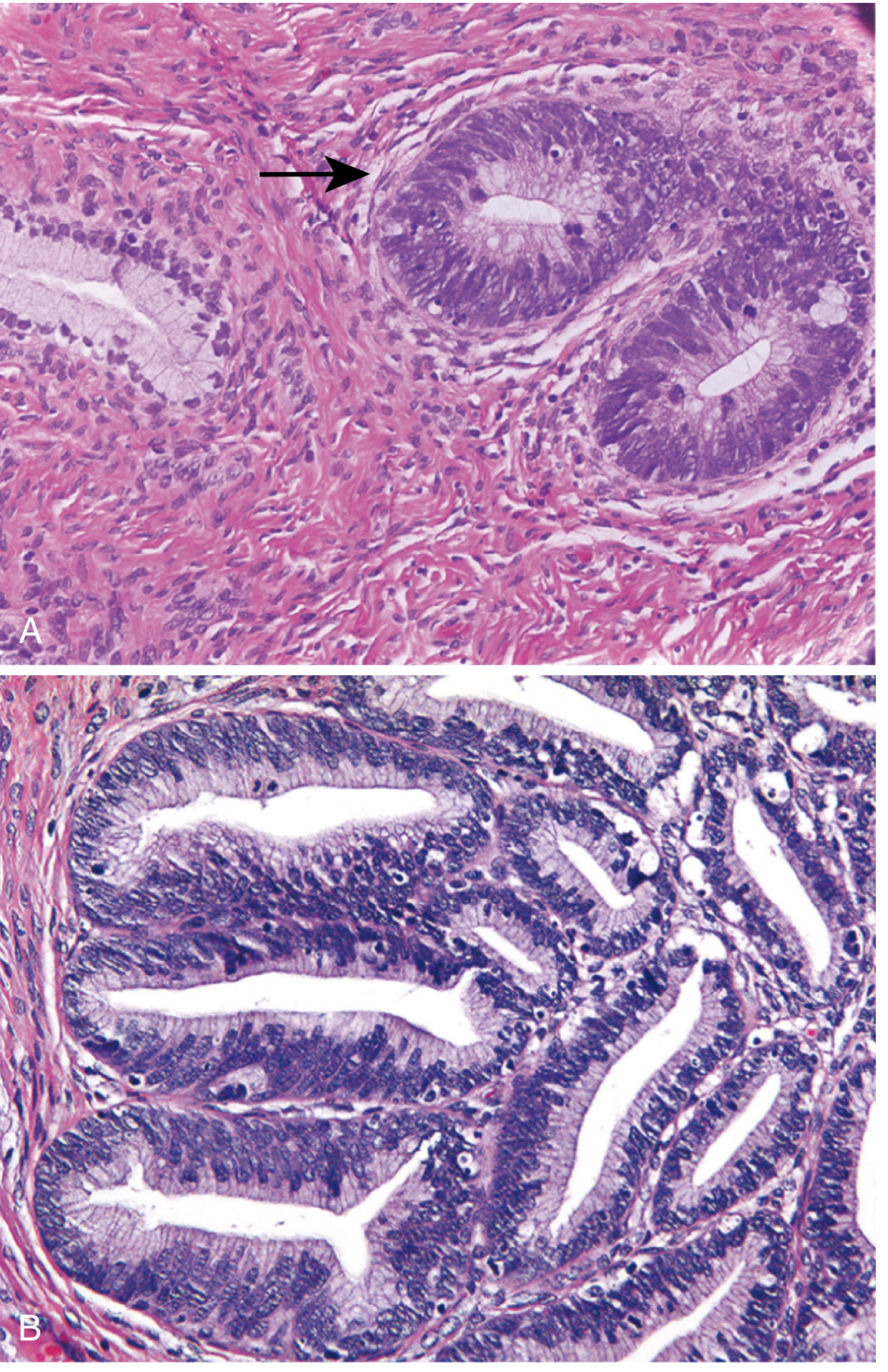
Spread
- Direct extension: paracervical soft tissue, urinary bladder, ureters (hydronephrosis), rectum, vagina
- Lymphovascular invasion: pelvic and para-aortic lymph nodes
- Distant metastases: liver, lungs, bone marrow
Staging (FIGO/Robbins)
| Stage | Description |
|---|---|
| Stage 0 | Carcinoma in situ (CIN III / HSIL) |
| Stage I | Confined to cervix |
| Ia | Microscopic invasion only |
| Ia1 | Stromal invasion ≤3 mm depth |
| Ia2 | Invasion >3 mm but ≤5 mm |
| Ib | Clinically visible, confined to cervix; >Ia2 |
| Stage II | Beyond cervix but not to pelvic wall; upper 2/3 of vagina involved |
| Stage III | Lower 1/3 vagina; extends to pelvic wall; hydronephrosis; pelvic/para-aortic LN involvement |
| Stage IV | Beyond true pelvis; bladder/rectal mucosa involvement; distant metastases |
Prognosis
- Superficially invasive SCC (Ia1): 5-year survival ~100%
- Tumors extending beyond pelvis: <20% 5-year survival
- Neuroendocrine carcinoma and gastric-type HPV-independent adenocarcinoma: very poor prognosis
- Risk of LN metastasis: <1% for tumors <3 mm depth; >10% for invasion >3 mm
Treatment
- Ia1: cone biopsy (excision) may be sufficient
- Ia2 / Ib: radical hysterectomy + pelvic lymph node dissection
- Advanced (Stage II-IV): radiation + cisplatin-based chemotherapy
Summary: Spectrum of Cervical Disease
Normal cervix
↓ HPV infection (especially in transformation zone)
↓
LSIL (CIN I) — productive infection, koilocytes → 60% REGRESS
↓ (persistent high-risk HPV)
HSIL (CIN II/III) — arrested maturation, full-thickness dysplasia → 30% regress; 10% progress
↓ (over years to decades)
Microinvasive carcinoma (Stage Ia)
↓
Invasive carcinoma (Stages Ib-IV)
Sources:
- Robbins, Cotran & Kumar: Pathologic Basis of Disease - Chapter 22 (Female Genital Tract)
- Robbins & Kumar: Basic Pathology - Chapter 17 (Female Genital System)
This is a shared conversation. Sign in to Orris to start your own chat.