biocbemical liver function tests
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough, well-structured response. Let me compile it.
Biochemical Liver Function Tests
The term "liver function tests" (LFTs) is a slight misnomer - many of the most commonly ordered tests (aminotransferases, alkaline phosphatase) do not actually measure a function of the liver. Rather, they detect liver cell damage or interference with bile flow. The preferred modern term is liver biochemical tests. No single test can fully assess the liver's total functional capacity; a battery of tests is required.
- Harrison's Principles of Internal Medicine 22E, p. 2677
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
1. Serum Bilirubin
Bilirubin is a breakdown product of the porphyrin ring of heme-containing proteins. It circulates in two forms:
| Fraction | Also Called | Solubility | Renal Excretion |
|---|---|---|---|
| Unconjugated | Indirect | Water-insoluble; bound to albumin | No |
| Conjugated | Direct | Water-soluble | Yes (bilirubinuria) |
Normal values: Total serum bilirubin 0.2-0.9 mg/dL (95th percentile); upper limit usually reported as 1-1.5 mg/dL. Conjugated bilirubin upper limit: 0.3 mg/dL.
Interpretation:
- Isolated unconjugated hyperbilirubinemia (<15% direct): Rarely due to liver disease. Causes include hemolytic disorders and genetic syndromes (Gilbert's, Crigler-Najjar). Work up for hemolysis; if negative, consider Gilbert's syndrome.
- Conjugated hyperbilirubinemia (>15% direct): Almost always implies liver or biliary tract disease. The rate-limiting step in bilirubin metabolism is transport into the bile canaliculi, not conjugation - so conjugated bilirubin can be elevated in any liver disease.
- In most liver diseases, both fractions are elevated.
- Bilirubinuria - because unconjugated bilirubin is bound to albumin and cannot be filtered, any bilirubin in urine is conjugated, indicating liver disease or obstructive jaundice.
Prognostic role: Bilirubin is a key component of the MELD score (Model for End-Stage Liver Disease), used to prioritize liver transplant candidates. High bilirubin in viral hepatitis correlates with greater hepatocellular damage; in alcoholic hepatitis it correlates with poor outcome.
2. Serum Aminotransferases (Transaminases)
Aminotransferases are sensitive markers of hepatocyte damage and are most useful in recognizing acute hepatocellular disease.
| Test | Full Name | Distribution | Notes |
|---|---|---|---|
| ALT | Alanine aminotransferase | Primarily liver | More specific for liver injury |
| AST | Aspartate aminotransferase | Liver, cardiac muscle, skeletal muscle, kidney, brain, pancreas, RBCs | Less specific |
-
Liver cell necrosis is not required for release - increased membrane permeability is enough.
-
In acute hepatitis, ALT levels can reach 500-5000 IU/L; ALT > AST is the typical pattern.
-
AST:ALT ratio >2 is characteristic of alcoholic hepatitis or cirrhosis.
-
In acute fulminant hepatic failure, AST and ALT may exceed 10,000 IU/L, with a disproportionate rise of AST over ALT.
-
Because ~80% of liver tissue must be destroyed before protein synthesis or ammonia metabolism fails, aminotransferases are often the first and only abnormal test in hepatitis.
-
Harrison's Principles of Internal Medicine 22E, p. 2678
-
Henry's Clinical Diagnosis and Management by Laboratory Methods
3. Alkaline Phosphatase (ALP)
ALP reflects cholestasis (impaired bile flow) rather than hepatocyte injury. It is located on the canalicular (bile duct) surface of hepatocytes.
Causes of elevated ALP:
- Intra- or extrahepatic cholestasis: elevation often >4× normal
- Infiltrative diseases (hepatic metastases, granulomata): elevation often >4× normal - ALP is the most sensitive marker of hepatic metastases
- Bone disease (Paget disease, osteoblastic activity) - bone origin
- Normal growth in children and pregnancy
Non-pathologic causes of elevated ALP:
- Normal childhood growth and pregnancy
- Ingesting a meal can raise ALP by 30% for up to 12 hours (intestinal isoenzyme)
- Oral contraceptives
Decreased ALP: Seen in hypophosphatasia, malnutrition, Wilson disease, theophylline therapy; hemolysis can falsely lower it.
Confirming hepatic origin: Use GGT or 5'-nucleotidase as adjuncts. If these are normal, the excess ALP is most likely of bone origin.
- Quick Compendium of Clinical Pathology 5th ed.
4. Gamma-Glutamyl Transferase (GGT)
- Located on biliary epithelial cells and hepatocyte limiting plates
- Highly sensitive indicator of hepatobiliary injury, principally biliary tract
- Used to confirm that an elevated ALP is of hepatic origin
- Not specific - elevated by many chemical exposures: warfarin, barbiturates, phenytoin, valproate, methotrexate
- Alcohol marker: GGT elevated in up to 70% of chronic alcoholics; levels correlate with alcohol consumption; can be elevated to 2-3× the upper limit of normal (ULN) in heavy drinkers
-
- Quick Compendium of Clinical Pathology 5th ed.
5. 5'-Nucleotidase (5'-NT)
- An adjunct to ALP to confirm biliary/hepatic origin of ALP elevation
- More specific than ALP for liver disease
- If 5'-NT and GGT are within normal range, an elevated ALP is most likely of bone origin
- Used alongside GGT in biliary obstruction workup
6. Serum Albumin
- Synthesized exclusively by the liver
- Reflects hepatic synthetic function
- Half-life ~20 days, so levels fall slowly and are a marker of chronic rather than acute liver injury
- Reduced when >80% of liver tissue is destroyed (cirrhosis, fulminant hepatic failure)
- Hypoalbuminemia in liver disease also contributes to ascites (reduced oncotic pressure)
-
- Henry's Clinical Diagnosis and Management by Laboratory Methods
7. Prothrombin Time (PT) / INR
- Reflects synthesis of clotting factors I, II, V, VII, X - all made in the liver
- Factor VII has the shortest half-life (~6 hours), so PT is a sensitive marker of acute changes in hepatic synthetic function
- PT is prolonged in both acute and chronic liver disease
- Key differential: if PT corrects with parenteral vitamin K, the cause is cholestasis (fat malabsorption reducing vitamin K absorption), not hepatocellular failure; if it fails to correct, it suggests poor synthetic function (parenchymal disease)
- PT >5× control that fails to correct with vitamin K in acute hepatitis suggests poor prognosis
- Also used in MELD score
8. Serum Ammonia
- The liver is the only tissue that can metabolize ammonia via the urea cycle (Krebs-Henseleit cycle)
- Ammonia rises only when >80% of liver tissue is destroyed
- Elevated in cirrhosis and fulminant hepatic failure
- Causes hepatic encephalopathy
9. Total Protein and Serum Protein Electrophoresis (SPEP)
- Liver synthesizes >90% of serum proteins including all albumin
- Levels fall only in severe parenchymal disease (>80% destruction)
- In cirrhosis, gamma globulins are elevated (polyclonal) - reflecting immune activation
Patterns of LFTs in Disease
The following table (from Harrison's 22E, Table 348-1) summarizes key patterns:
| Disorder | Bilirubin | Aminotransferases | ALP | Albumin | PT |
|---|---|---|---|---|---|
| Hemolysis / Gilbert's | Elevated, indirect (unconjugated); <5 mg/dL | Normal | Normal | Normal | Normal |
| Acute hepatocellular necrosis (viral, ischemic, drug) | Both fractions elevated | >500 IU; ALT > AST | Normal to <3× | Normal | Usually normal; if >5× and not corrected by vitamin K - poor prognosis |
| Chronic hepatocellular disease | Both fractions elevated | Elevated, but usually <300 IU | Normal to <3× | Often decreased | Often prolonged; fails to correct with vitamin K |
| Alcoholic hepatitis / cirrhosis | Both fractions elevated | AST:ALT >2 | Normal to <3× | Often decreased | Often prolonged |
| Cholestasis (intra/extrahepatic obstruction) | Both fractions elevated (conjugated dominant) | Normal to moderate (<500 IU) | Elevated, often >4× | Normal (unless chronic) | Prolonged; corrects with vitamin K |
| Infiltrative disease (tumor, granuloma) | Usually normal | Normal to slight elevation | Elevated, often >4× (confirm with GGT or 5'-NT) | Normal | Normal |
| Cirrhosis (panhepatic) | Both elevated | Normal or low/mildly elevated | May be elevated | Low | Prolonged |
| Fulminant hepatic failure | Elevated | >10,000 IU; AST>ALT | Elevated | Markedly low | Markedly prolonged |
Diagnostic Algorithm for Abnormal Liver Tests
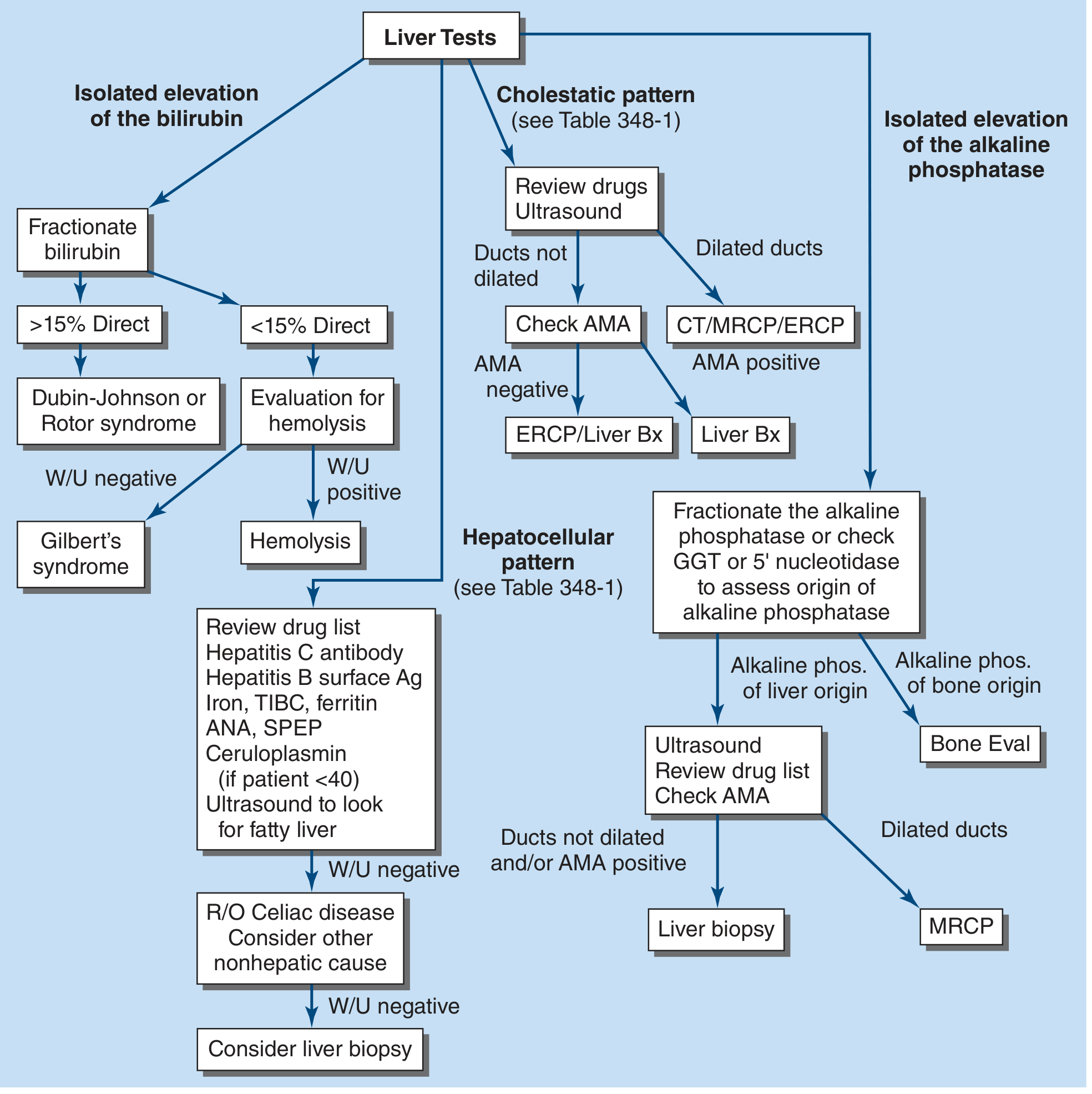
Figure from Harrison's Principles of Internal Medicine 22E: Algorithm for evaluation of abnormal liver tests. Ag, antigen; AMA, antimitochondrial antibody; ANA, antinuclear antibody; Bx, biopsy; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; GGT, gamma-glutamyl transpeptidase; MRCP, magnetic resonance cholangiopancreatography.
Key decision points:
- Isolated unconjugated bilirubin: Fractionate → hemolysis workup or Gilbert's syndrome
- Isolated conjugated bilirubin: Dubin-Johnson or Rotor syndrome if no other abnormality
- Hepatocellular pattern (high aminotransferases): Review drugs, check viral hepatitis serology, iron studies, ANA, ceruloplasmin (if <40 years), ultrasound for fatty liver
- Cholestatic pattern (high ALP + bilirubin): Ultrasound first - dilated ducts → CT/MRCP/ERCP; non-dilated → check AMA (antimitochondrial antibody for primary biliary cholangitis)
- Isolated ALP elevation: Fractionate or confirm hepatic origin with GGT/5'-NT; if bone origin → bone evaluation; if hepatic origin → ultrasound, review drugs, check AMA
Summary: Grouping the Tests by Function
| Category | Tests | What They Detect |
|---|---|---|
| Hepatocyte damage | AST, ALT, LDH | Cell injury/necrosis |
| Cholestasis/biliary | ALP, GGT, 5'-NT | Bile duct injury/obstruction |
| Hepatic synthetic function | Albumin, PT/INR, clotting factors | Functional reserve of the liver |
| Excretory function | Bilirubin (direct/indirect) | Uptake, conjugation, secretion |
| Detoxification | Ammonia | Urea cycle capacity |
A battery of tests covering all these categories is needed to characterize liver disease fully, since no single test captures the liver's diverse biochemical roles.
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 348
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Quick Compendium of Clinical Pathology 5th ed.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.