Nephrotic Syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
I now have very comprehensive content. Let me compile the full response:
Nephrotic Syndrome
Definition
Nephrotic syndrome is a clinical constellation resulting from increased glomerular permeability. The diagnostic tetrad is:
| Feature | Threshold |
|---|---|
| Proteinuria | >3.5 g/day in adults (nephrotic range) |
| Hypoalbuminemia | Serum albumin <3 g/dL (often <2.5 g/dL) |
| Edema | Generalized, dependent pitting; anasarca |
| Hyperlipidemia | Total cholesterol usually >180 mg/dL; lipiduria |
Not all patients with >3.5 g/day proteinuria develop full syndrome - some sustain compensatory increases in hepatic albumin synthesis that normalize serum levels.
- Brenner and Rector's The Kidney
- Frameworks for Internal Medicine, p. 464
Pathophysiology
Glomerular Barrier Failure
Nephrotic syndrome occurs when glomerular charge and size selectivity are impaired. This selectivity is normally maintained by the glomerular basement membrane (GBM), endothelial cells, and podocytes (visceral epithelial cells). Injury to any of these components - especially podocyte foot process effacement - allows large molecules like albumin (MW ~69 kDa) to escape into the urine.
Edema: Two Mechanisms
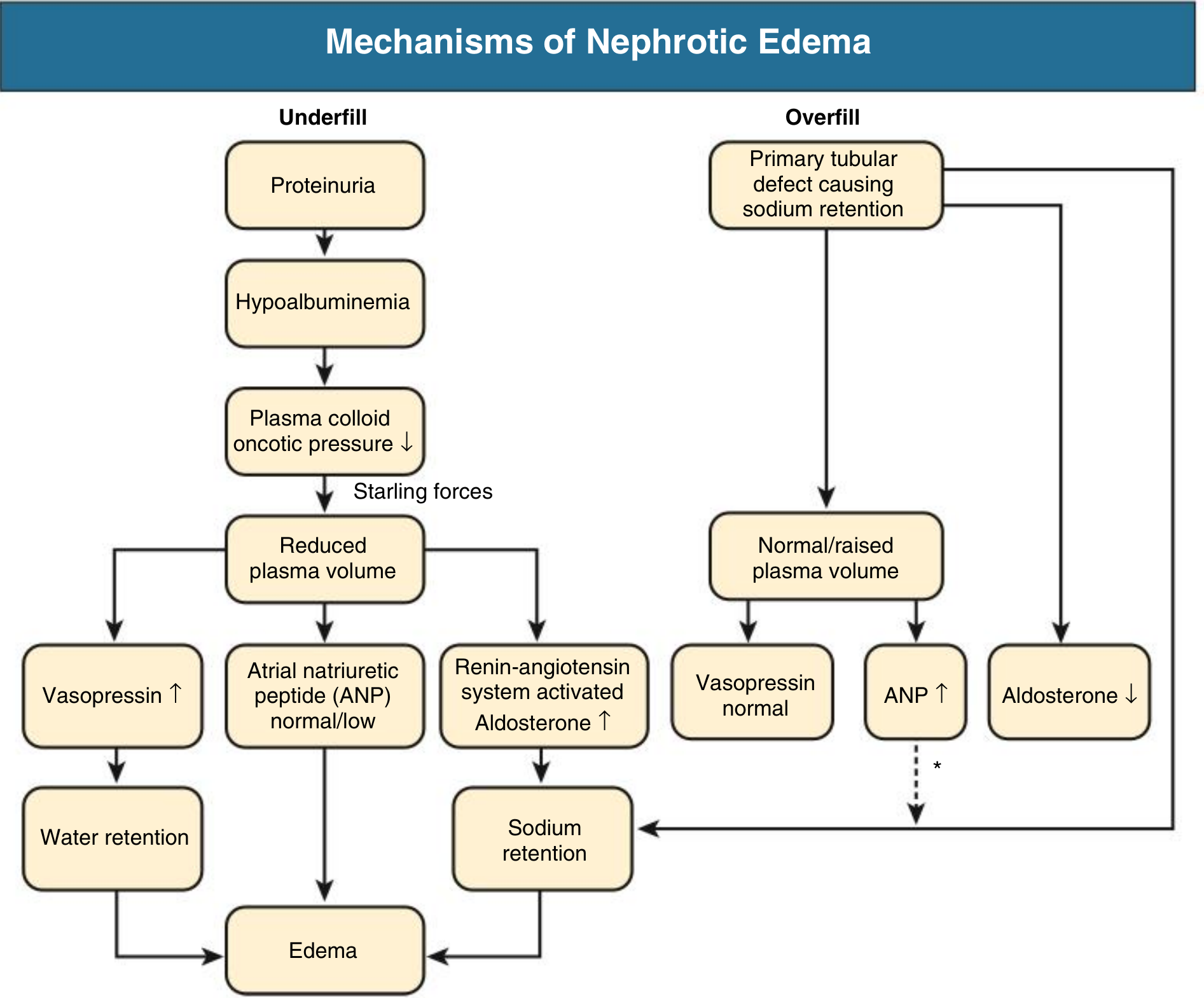
1. Underfill (classic): Proteinuria → hypoalbuminemia → reduced plasma oncotic pressure → fluid shifts to interstitium → reduced circulating volume → activation of RAS/aldosterone → sodium retention → worsening edema. Patients with minimal change disease typically follow this pattern with contracted plasma volume and elevated renin/aldosterone.
2. Overfill (more common in practice): A primary tubular defect in the distal nephron causes sodium retention (possibly via proteolytic activation of ENaC by proteins that enter the tubular lumen). This leads to expanded plasma volume, suppressed RAS, and a tendency to hypertension rather than hypotension. Most nephrotic patients beyond MCD follow this pathway.
- Comprehensive Clinical Nephrology, 7th Ed., p. 240
Hypoalbuminemia
Urinary albumin loss is the primary driver. The liver responds by increasing albumin synthesis, but this compensatory mechanism is blunted in nephrotic syndrome. Protein synthesis is non-discriminating - large molecules not lost in urine (e.g., fibrinogen) actually increase in plasma, which has major clinical consequences for coagulation and lipid metabolism.
Hyperlipidemia and Lipiduria
Caused by a combination of:
- Increased hepatic lipoprotein synthesis (stimulated by reduced oncotic pressure)
- Abnormal transport of circulating lipid particles
- Decreased lipid catabolism
Lipiduria reflects increased GBM permeability to lipoproteins. The elevated lipids are visible on urinalysis as oval fat bodies (lipid-laden epithelial cells) and fatty casts.
Hypercoagulability
Loss of anticoagulant proteins in the urine (antithrombin III, protein C, protein S) combined with increased hepatic production of procoagulant proteins (fibrinogen, factors V and VIII) creates a strongly prothrombotic state. Thromboembolism affects 10-40% of nephrotic patients. The most common sites are renal veins and deep veins of the lower extremities. Membranous nephropathy has the highest risk of renal vein thrombosis.
Susceptibility to Infection
- Low serum IgG (lost in urine)
- Reduced complement activity
- Diminished T-cell function
- Risk of bacterial peritonitis from Streptococcus pneumoniae is particularly high in children
Causes and Classification

Primary (Idiopathic) Causes
| Disease | Key Features | Age | Steroids |
|---|---|---|---|
| Minimal Change Disease (MCD) | Normal LM; foot process effacement on EM only; selective proteinuria (mostly albumin); unknown pathogenesis | Children (most common), adults (15%) | Excellent response |
| Focal Segmental Glomerulosclerosis (FSGS) | Scarring of segments of some glomeruli; podocyte injury; circulating permeability factors; nonselective proteinuria | Adults; African-Americans disproportionately affected | Typically resistant |
| Membranous Nephropathy (MN) | In-situ immune complex formation; antibodies to podocyte antigens (PLA2R - most common, THSD7A, NELL-1); subepithelial deposits on EM | Adults (most common primary cause in whites) | Variable |
| Membranoproliferative GN (MPGN) | GBM thickening + mesangial hypercellularity; immune complex-mediated | Young adults | Poor |
| C3 Glomerulopathy | Excessive, dysregulated complement activation; dense deposit disease | Variable | Poor |
FSGS: FSGS is the most common cause of glomerular disease in Black patients (~50% of cases). Primary FSGS presents with nephrotic syndrome AND >80% foot process effacement on EM; secondary FSGS (from reduced renal mass, infections, drugs, genetic causes) shows <80% effacement and typically no nephrotic syndrome at onset.
FSGS is most frequently associated with thromboembolism among all nephrotic causes.
Secondary Causes
- Medications: Mercury, organic gold, penicillamine, NSAIDs, heroin, lithium, pamidronate, interferon-α, captopril, rifampin
- Systemic diseases: Diabetes mellitus (diabetic nephropathy - most common cause worldwide), SLE (Class V membranous lupus nephritis), amyloidosis, multiple myeloma
- Infections: Hepatitis B, hepatitis C, HIV, malaria, syphilis
- Malignancy: Paraneoplastic MN (solid tumors), Hodgkin lymphoma (associated with MCD)
- Hereditary: Mutations in podocyte genes (NPHS1, NPHS2/podocin, WT1, PLCE1, TRPC6, EMP2, CRB2)
Age-based predominance:
-
Children: MCD >> FSGS >> MN
-
Adults: MN >> FSGS >> MCD (in white adults); FSGS >> MN (in Black adults)
-
Brenner and Rector's The Kidney, Block 17
-
Comprehensive Clinical Nephrology, 7th Ed.
Clinical Features
Symptoms: Peripheral edema (often anasarca), foamy urine, fatigue, dyspnea
Signs:
- Generalized pitting edema, periorbital edema (especially in children, worse in the morning)
- Ascites, pleural effusions
- Hypertension
- Muehrcke's lines (paired white transverse bands of the nails - sign of hypoalbuminemia)
- Eruptive xanthomata, xanthelasma (from hyperlipidemia)
Laboratory Evaluation
| Test | Finding |
|---|---|
| Urine protein | >3.5 g/24 hr; spot urine protein:creatinine ratio >3.5 (correlates with 24-hr collection) |
| Urine microscopy | Oval fat bodies, fatty casts, lipiduria (no RBC casts - distinguishes from nephritic) |
| Serum albumin | <3 g/dL |
| Lipid panel | Elevated LDL, total cholesterol, triglycerides |
| Serum creatinine | Variable |
| Serum sodium | May be low (pseudohyponatremia from hypertriglyceridemia) |
| Serum calcium | Total low (bound to albumin); ionized calcium usually normal |
| Coagulation studies | Elevated fibrinogen, reduced antithrombin III |
| Complement | Check C3, C4 (low in MPGN, lupus nephritis) |
| Serology | ANA/anti-dsDNA (SLE), anti-PLA2R (membranous nephropathy), hepatitis B/C, HIV, SPEP |
Kidney Biopsy: Not routinely done in children on first presentation (MCD assumed). Biopsy is indicated in:
- Adults (all cases where diagnosis unclear)
- Infants
- Persistent hematuria, hypocomplementemia, or elevated creatinine
- Steroid resistance or dependence
Complications
| Complication | Mechanism |
|---|---|
| Venous thromboembolism (DVT, renal vein thrombosis, PE) | Loss of antithrombin III, protein C and S; raised fibrinogen |
| Arterial thrombosis (MI, stroke) | Rare but described |
| Infections (cellulitis, peritonitis, sepsis) | Low IgG, reduced complement, T-cell dysfunction |
| AKI | Volume depletion, renal vein thrombosis, sepsis |
| Malnutrition / growth failure | Protein loss, steroid therapy |
| Accelerated atherosclerosis | Dyslipidemia |
| Drug toxicity | Altered pharmacokinetics (e.g., furosemide bound to albumin; hypoalbuminemia enlarges volume of distribution of many drugs) |
Management
General / Supportive
- Sodium restriction (<2 g/day) and fluid restriction
- Diuretics: Loop diuretics (furosemide 1-2 mg/kg) for edema; note that hypoalbuminemia reduces furosemide binding to plasma proteins and alters its pharmacokinetics. IV albumin (0.5-1 g/kg) followed by furosemide may be needed for profound hypoalbuminemia, but iso-oncotic albumin infusion alone does not reliably induce negative sodium balance.
- ACE inhibitors or ARBs: Reduce proteinuria, combat coagulopathy, dyslipidemia, edema, and slow progression - considered cornerstone anti-proteinuric therapy regardless of cause
- Statins: For hyperlipidemia (HMG-CoA reductase inhibitors)
- Anticoagulation: For thromboembolism (therapeutic) or prophylaxis in high-risk cases (e.g., serum albumin <2.5 g/dL, MN with heavy proteinuria) - prophylactic anticoagulation remains controversial
- Vaccinations: Pneumococcal vaccine (23-valent) especially in children; avoid live vaccines during immunosuppression
- Low-salt diet (<2 g/day)
Disease-Specific Immunosuppression
| Cause | First-Line | Second-Line |
|---|---|---|
| MCD | Oral corticosteroids (prednisone 1 mg/kg/day or 2 mg/kg/day in children, max 60 mg/day) | Cyclosporine, cyclophosphamide, tacrolimus, rituximab |
| FSGS (primary) | High-dose corticosteroids (often for 3-6 months) | Calcineurin inhibitors (cyclosporine/tacrolimus - best evidence for steroid-resistant FSGS), rituximab |
| Membranous nephropathy | Watch-and-wait for spontaneous remission (30-40%); treat persistent nephrotic syndrome or declining renal function | Rituximab (now preferred); cyclophosphamide + steroids (Ponticelli protocol); calcineurin inhibitors |
| MPGN / C3G | Treat underlying cause; steroids, MMF | Variable |
| Secondary | Treat underlying disease | - |
Steroid-resistant nephrotic syndrome (no remission after 8 weeks of adequate steroids in children) - calcineurin inhibitors (cyclosporin A or tacrolimus) are the best initial alternative.
Common second-line agents: Cyclosporine, cyclophosphamide, mycophenolate mofetil (MMF), tacrolimus, rituximab
ED Disposition
- Admit: Severe edema, pleural effusions/respiratory compromise, systemic infection, thrombotic complications
- Outpatient: Mild-moderate edema with close nephrology follow-up
Nephrotic vs. Nephritic Syndrome (Key Distinction)
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | >3.5 g/day (massive) | Subnephrotic |
| Hematuria | Absent (no RBC casts) | Present (RBC casts) |
| Edema | Prominent | Mild-moderate |
| Hypertension | Variable | Common |
| Mechanism | Permeability defect | Inflammation |
| Examples | MCD, FSGS, MN | Post-strep GN, IgA nephropathy, lupus nephritis |
Recent Evidence (2024-2026)
Three recent high-quality Cochrane reviews are relevant:
- Non-corticosteroid immunosuppressives in steroid-sensitive pediatric NS (Larkins et al., Cochrane 2024, PMID 39513526) - systematic review of alternatives in children
- Interventions for idiopathic steroid-resistant NS in children (Liu et al., Cochrane 2025, PMID 40337980) - most current evidence on steroid-resistant cases
- NS associated with solid malignancies (Liu et al., BMC Nephrol 2024, PMID 38965515) - systematic review highlighting paraneoplastic nephrotic syndrome
Sources: Brenner and Rector's The Kidney | Comprehensive Clinical Nephrology, 7th Ed. | Robbins & Kumar Basic Pathology | Frameworks for Internal Medicine | Tintinalli's Emergency Medicine | Washington Manual of Medical Therapeutics | National Kidney Foundation Primer on Kidney Diseases, 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.