neuro muscular junction
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Here is a complete answer on the neuromuscular junction:
Neuromuscular Junction (NMJ)
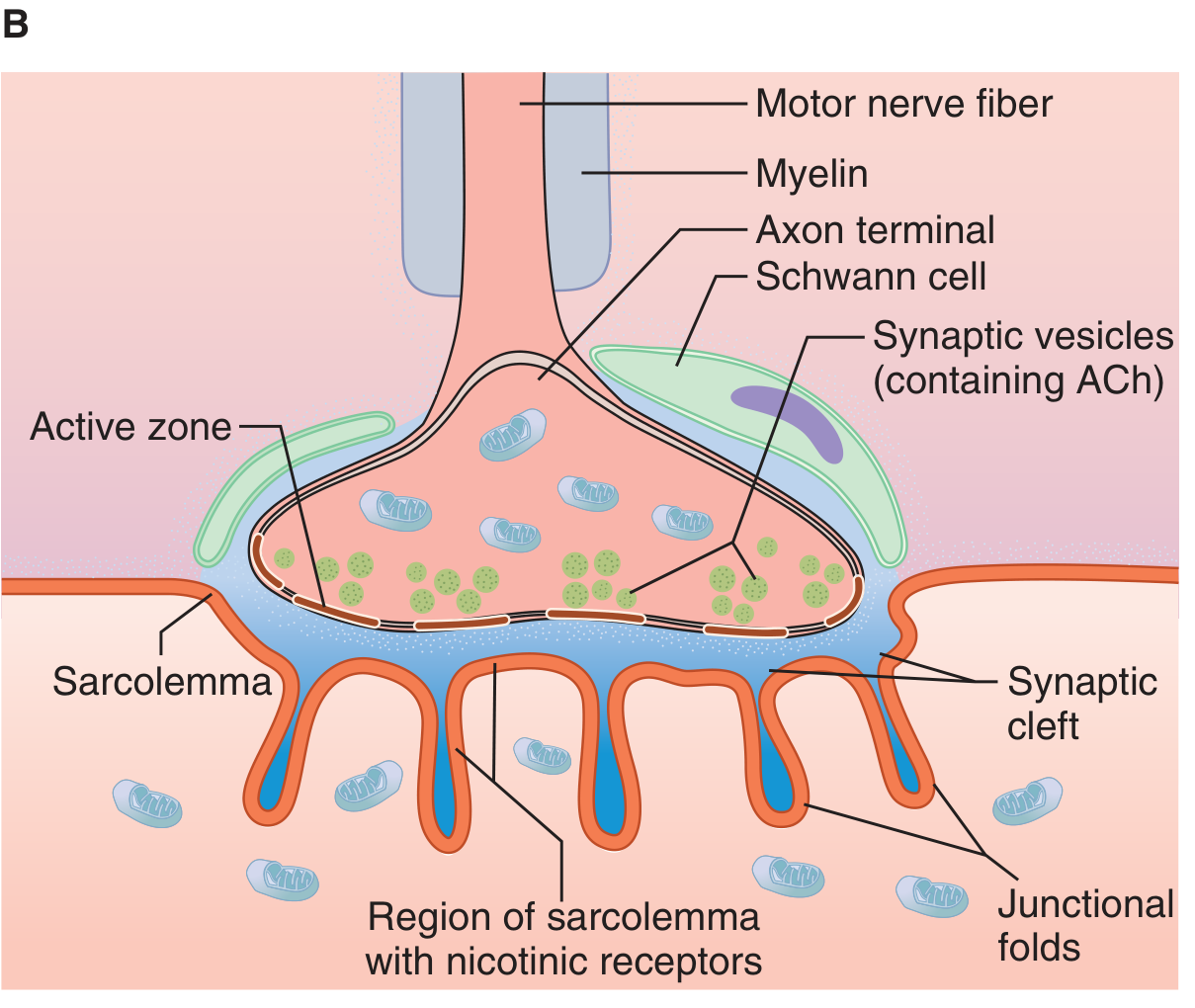
Anatomy and Structure
The neuromuscular junction (NMJ) is the specialized chemical synapse between a motor neuron axon terminal and a skeletal muscle fiber. It is the most intensely studied synapse in the nervous system, and its principles apply broadly to other chemical synapses.
Key structural components:
- Motor nerve terminal (presynaptic bouton): The myelinated axon loses its myelin sheath as it approaches the muscle and divides into multiple terminal boutons. Each bouton sits in a groove in the muscle surface called the synaptic gutter or junctional trough.
- Active zone: The area of the presynaptic membrane where synaptic vesicles dock and fuse; it is directly opposite the postjunctional folds.
- Synaptic vesicles: Contain acetylcholine (ACh), stored in packets called quanta (~5,000–10,000 ACh molecules per vesicle).
- Synaptic cleft: ~50 nm wide; filled with connective tissue and acetylcholinesterase (AChE) anchored to it.
- Motor endplate (postsynaptic membrane): The thickened portion of the sarcolemma beneath the bouton, folded into junctional folds that dramatically increase surface area. Nicotinic ACh receptors (nAChR) are concentrated at the crests of these folds; voltage-gated Na⁺ channels are concentrated in the depths.
- Schwann cells: Cap the nerve terminal from above.
Each muscle fiber receives input from only one motor neuron; each motor neuron can innervate many fibers - this assembly is the motor unit.
Sequence of Events at the NMJ (8 Steps)
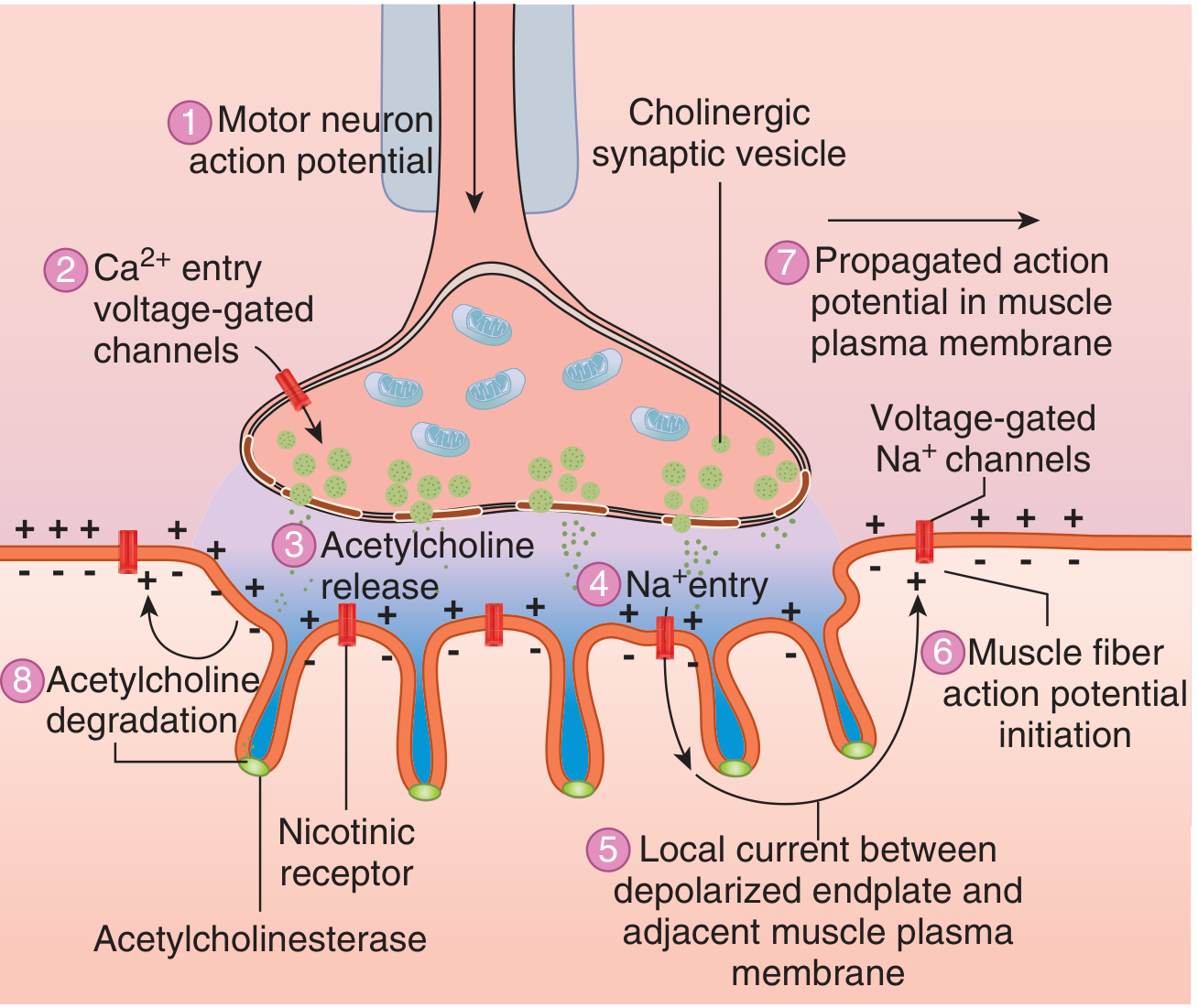
- Action potential arrives at the motor nerve terminal.
- Ca²⁺ influx through voltage-gated Ca²⁺ channels in the presynaptic membrane.
- Exocytosis of ACh - Ca²⁺ triggers fusion of synaptic vesicles with the presynaptic membrane via SNARE proteins; ACh quanta are released into the cleft.
- ACh diffuses across the synaptic cleft (~50 nm) and binds to nicotinic N_M receptors at the crests of junctional folds.
- Endplate potential (EPP): Binding of two ACh molecules opens the nAChR ion channel, allowing Na⁺ influx (and lesser K⁺ efflux) → local depolarization of 50-75 mV called the end plate potential. Note: The inward Na⁺ current dominates because the electrochemical driving force for Na⁺ (~160 mV inward) far exceeds that for K⁺ (~10 mV outward).
- Action potential initiation: The EPP depolarizes adjacent sarcolemma beyond threshold, opening voltage-gated Na⁺ channels concentrated in the depths of the junctional folds.
- Propagated action potential spreads along the entire muscle fiber → muscle contraction.
- ACh degradation: Acetylcholinesterase rapidly hydrolyzes ACh into choline + acetate within milliseconds, terminating the signal. Choline is recycled back into the terminal for ACh resynthesis.
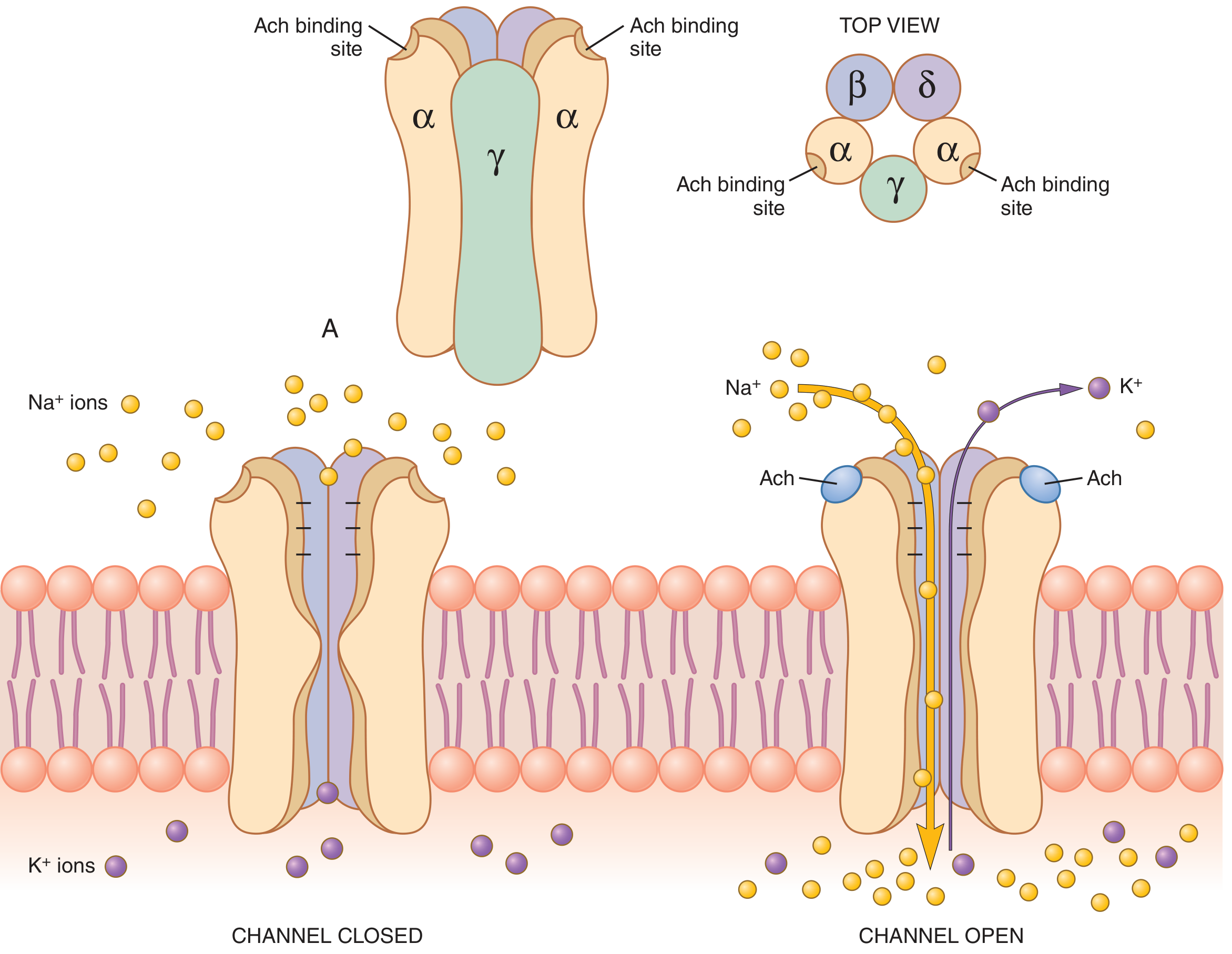
The Nicotinic ACh Receptor (nAChR)
The postsynaptic receptor is a pentameric ligand-gated ion channel:
- Subunit composition: 2α + 1β + 1δ + 1γ (fetal) or 1ε (adult)
- ACh binds to both α subunits simultaneously - both must be occupied to open the channel
- Ion selectivity: Permeable to Na⁺ and K⁺ (not Cl⁻, due to negative charges at the channel mouth); net Na⁺ influx dominates
- Opening: Conformational change opens the central channel pore
Safety Factor
Each arriving nerve impulse generates an EPP approximately 3x larger than the threshold needed to fire a muscle action potential. This large safety margin ensures reliable neuromuscular transmission even when ACh release is somewhat reduced (e.g., in disease or fatigue). - Guyton and Hall Textbook of Medical Physiology
ACh Synthesis and Recycling
- ACh is synthesized in the nerve terminal from choline + acetyl-CoA by choline acetyltransferase (ChAT)
- Packed into vesicles by a vesicular ACh transporter (VAChT) using H⁺ exchange
- After degradation by AChE, choline is taken back up by a high-affinity choline transporter in the presynaptic membrane
Disorders of the NMJ
| Disorder | Site | Mechanism | Key Feature |
|---|---|---|---|
| Myasthenia Gravis | Postsynaptic | Autoantibodies to AChR (85%) or MuSK (most of the rest); complement-mediated destruction of junctional folds | Fatigable weakness; ocular/bulbar onset; decremental response on repetitive nerve stimulation |
| Lambert-Eaton Syndrome | Presynaptic | Autoantibodies against voltage-gated Ca²⁺ channels → reduced ACh release | Proximal weakness; incremental response on high-frequency stimulation; associated with small cell lung cancer (2/3 of cases) |
| Botulism | Presynaptic | Botulinum toxin cleaves SNARE proteins → blocks ACh exocytosis | Flaccid descending paralysis |
| Tetanus | Spinal interneurons | Tetanus toxin blocks inhibitory neurotransmitter release → excess ACh effect | Spastic paralysis, trismus |
| Congenital Myasthenic Syndromes | Pre/synaptic/post | Mutations in NMJ proteins | Mimics MG or Lambert-Eaton |
Myasthenia Gravis - Expanded
- Autoantibodies are classified as binding (complement activation), blocking (prevent ACh binding), or modulating (cross-link and internalize receptors)
- Thymic abnormalities in ~75-85%: thymic hyperplasia (60-70%) or thymoma (10-15%)
- Bimodal incidence: young women (2nd-3rd decade) and older men (6th-8th decade)
- Treatment: acetylcholinesterase inhibitors (pyridostigmine), steroids, other immunosuppressants, complement inhibitors (eculizumab), IVIg, plasmapheresis, thymectomy - Robbins & Kumar Basic Pathology
Lambert-Eaton Syndrome - Expanded
- Presynaptic Ca²⁺ channel antibodies reduce quantal ACh release
- Paradoxically, strength improves with brief exercise (Ca²⁺ accumulates with repeated stimulation)
- Treatment: 3,4-diaminopyridine (blocks presynaptic K⁺ channels, prolongs AP, increases Ca²⁺ influx); unlike MG, cholinesterase inhibitors are NOT effective
- Paraneoplastic in ~2/3; associated with small cell lung carcinoma - Robbins & Kumar Basic Pathology
Drugs Acting at the NMJ
| Drug/Agent | Mechanism | Use |
|---|---|---|
| Neostigmine, pyridostigmine | AChE inhibitors - prolong ACh in cleft | Myasthenia gravis; reversal of neuromuscular blockade |
| Succinylcholine | Depolarizing NMB - persistent agonist at nAChR | Rapid-sequence intubation |
| Rocuronium, vecuronium, atracurium | Non-depolarizing NMB - competitive antagonists at nAChR | Surgical paralysis |
| Botulinum toxin (Botox) | SNARE cleavage → blocks ACh release | Cosmetic use; blepharospasm; spasticity |
| Organophosphates | Irreversible AChE inhibition | Nerve agents/insecticides (toxin) |
Sources: Ganong's Review of Medical Physiology (26th ed.), Guyton and Hall Textbook of Medical Physiology, Medical Physiology (Boron & Boulpaep), Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.