ABG analysis basic to clinical
Reading File
Finding Sources
Finding Sources
Searching the Web
ABG arterial blood gas analysis stepwise approach clinical interpretation
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full ABG analysis guide:
Arterial Blood Gas (ABG) Analysis: Basic to Clinical
What Is an ABG?
An ABG samples arterial blood (usually radial artery) and directly measures:
| Parameter | Normal Value | What It Reflects |
|---|---|---|
| pH | 7.35 - 7.45 | H+ ion concentration; overall acid-base status |
| PaCO2 | 35 - 45 mmHg | Respiratory component; CO2 elimination |
| HCO3- | 22 - 26 mEq/L | Metabolic component (calculated from pH + PaCO2) |
| PaO2 | 80 - 100 mmHg | Dissolved O2 in arterial blood |
| SaO2 | 95 - 100% | Hemoglobin O2 saturation |
| Base Excess (BE) | -2 to +2 | Net metabolic acid/base deviation from normal |
The arterial sample reflects oxygenation and CO2 content after pulmonary circulation, before peripheral gas exchange. - Tintinalli's Emergency Medicine, p. 121
The Henderson-Hasselbalch Equation (Foundation)
$$pH = 6.1 + \log\frac{[HCO_3^-]}{0.03 \times PaCO_2}$$
This explains the relationship between the three primary ABG parameters. A pH change can result from:
- A change in HCO3- (metabolic)
- A change in PaCO2 (respiratory)
- Or both simultaneously (mixed disorder)
Step-by-Step ABG Interpretation
STEP 1 - Assess Oxygenation
Is the patient hypoxic?
- PaO2 < 80 mmHg = hypoxemia
- PaO2 < 60 mmHg = significant hypoxemia (SpO2 ~90%, threshold for O2 supplementation)
Calculate the A-a gradient to find the cause of hypoxia:
Alveolar Gas Equation: $$P_AO_2 = [FiO_2 \times (P_{atm} - P_{H_2O})] - \frac{PaCO_2}{R}$$ At room air (FiO2=0.21): PAO2= 150 - (PaCO2 / 0.8)
A-a Gradient = PAO2- PaO2
- Normal: 5-20 mmHg on room air; 20-65 mmHg on 100% O2
- Normal A-a gradient + hypoxia = pure hypoventilation (e.g., sedation, NMJ disease)
- Elevated A-a gradient = V/Q mismatch, shunt, or diffusion limitation (e.g., PE, pneumonia, pulmonary edema)
Harriet Lane Handbook, 23rd ed., p. 53
STEP 2 - Determine the Primary Acid-Base Disorder
Is there acidemia or alkalemia?
| pH | Status |
|---|---|
| < 7.35 | Acidemia |
| 7.35 - 7.45 | Normal |
| > 7.45 | Alkalemia |
Identify the primary process by checking PaCO2 and HCO3-:
| Primary Disorder | pH | Primary Change | Direction |
|---|---|---|---|
| Metabolic acidosis | ↓ | ↓ HCO3- | Same direction as pH |
| Metabolic alkalosis | ↑ | ↑ HCO3- | Same direction as pH |
| Respiratory acidosis | ↓ | ↑ PaCO2 | Opposite to pH |
| Respiratory alkalosis | ↑ | ↓ PaCO2 | Opposite to pH |
Key rule: In respiratory disorders, pH and PaCO2 change in opposite directions. In metabolic disorders, pH and HCO3- change in the same direction. - American Thoracic Society
STEP 3 - Assess Compensation
Compensation is always incomplete (never overshoots). Respiratory compensation for metabolic disorders is rapid (hours); renal compensation for respiratory disorders takes 3-5 days.
Compensation Formulas:
| Primary Disorder | Expected Compensation | Formula |
|---|---|---|
| Metabolic acidosis | ↓ PaCO2 | ΔPaCO2 = 1.3 × ΔHCO3- (Winters' formula) |
| Metabolic alkalosis | ↑ PaCO2 | ΔPaCO2 = 0.6 × ΔHCO3- |
| Respiratory acidosis (acute) | ↑ HCO3- | +1 mEq/L per 10 mmHg ↑ PaCO2 |
| Respiratory acidosis (chronic) | ↑ HCO3- | +4 mEq/L per 10 mmHg ↑ PaCO2 |
| Respiratory alkalosis (acute) | ↓ HCO3- | -2 mEq/L per 10 mmHg ↓ PaCO2 |
| Respiratory alkalosis (chronic) | ↓ HCO3- | -5 mEq/L per 10 mmHg ↓ PaCO2 |
Roberts and Hedges' Clinical Procedures in Emergency, p. 4814
The Rule of 15 (quick check for metabolic acidosis):
HCO3- + 15 ≈ last two digits of pH (and ≈ expected PaCO2) If PaCO2 matches: simple metabolic acidosis with respiratory compensation If PaCO2 > expected: also has respiratory acidosis If PaCO2 < expected: also has respiratory alkalosis
Rosen's Emergency Medicine, p. 2506
STEP 4 - Calculate the Anion Gap (for metabolic acidosis)
$$AG = Na^+ - (Cl^- + HCO_3^-)$$
Normal AG = 8-12 mEq/L (some labs use 9-15; always check your baseline)
| AG Status | Meaning | Common Causes |
|---|---|---|
| Elevated (>12) | Accumulation of unmeasured anions | MUDPILES: Methanol, Uremia, DKA, Propylene glycol/Paraldehyde, Isoniazid/Iron, Lactic acidosis, Ethylene glycol, Salicylates |
| Normal (non-gap) | HCO3- replaced by Cl- | HARDUP: Hyperalimentation, Acetazolamide, RTA, Diarrhea, Ureteral diversion, Pancreatic fistula |
Rosen's Emergency Medicine
Important: Correct for albumin if hypoalbuminemia present:
Corrected AG = Measured AG + 2.5 × (4 - albumin in g/dL)
STEP 5 - Delta-Delta Ratio (in high-AG metabolic acidosis)
Used to detect a hidden concurrent metabolic disorder within a high-AG acidosis:
$$\Delta\Delta = \frac{\Delta AG}{\Delta HCO_3^-} = \frac{(AG - 12)}{(24 - HCO_3^-)}$$
| Delta-Delta | Interpretation |
|---|---|
| < 0.4 | Normal AG acidosis (non-gap component) |
| 0.4 - 1.0 | Mixed high-gap + normal-gap acidosis |
| 1.0 - 2.0 | Pure high-gap metabolic acidosis |
| > 2.0 | High-gap acidosis + concurrent metabolic alkalosis |
Harrison's Principles of Internal Medicine, 22nd ed.
STEP 6 - Identify Mixed Disorders
If compensation is absent or exceeds expected ranges, a mixed disorder is present. Use the Acid-Base Map:
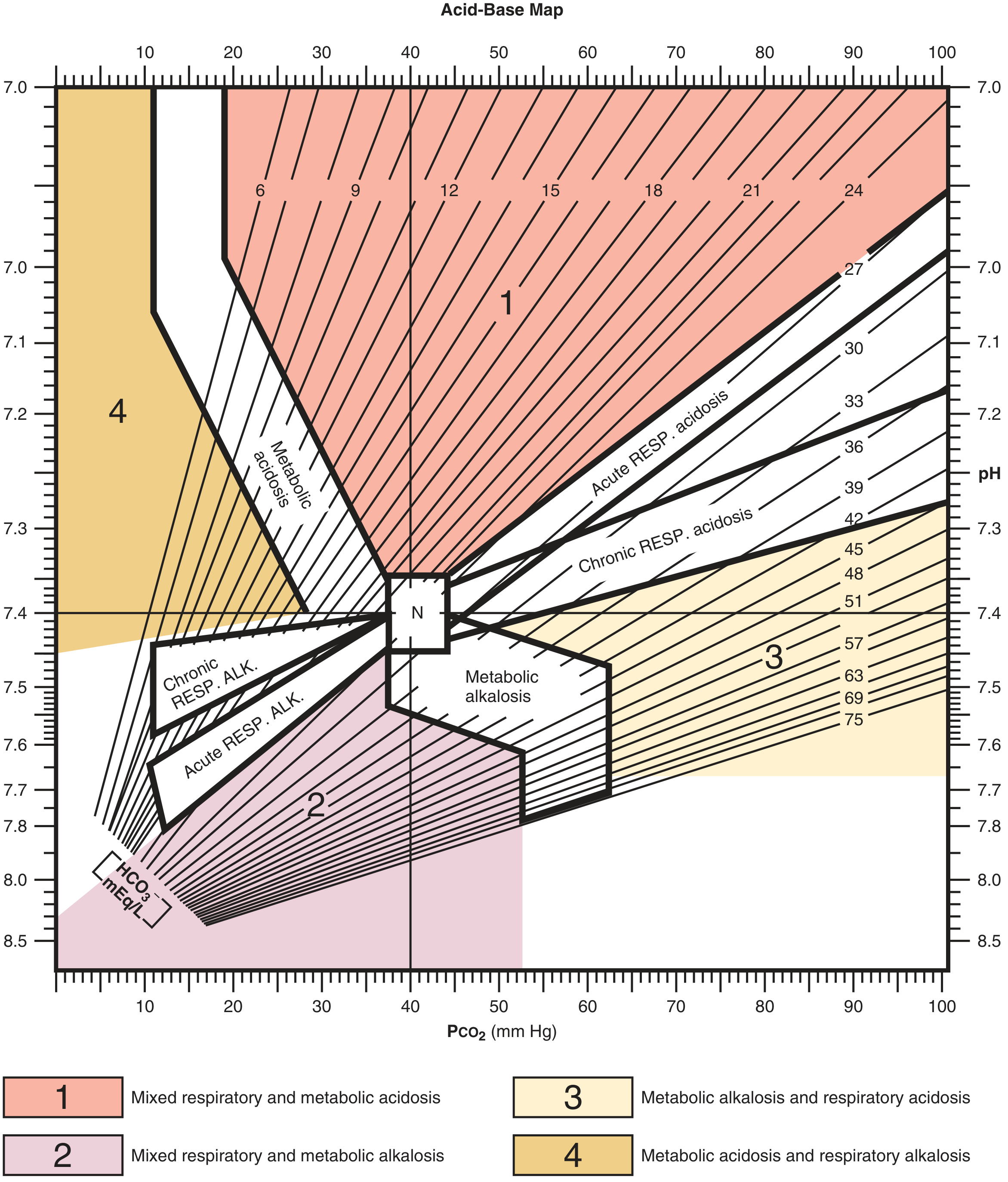
Points falling outside the compensation bands indicate a mixed disorder. - Roberts and Hedges' Clinical Procedures
Mixed Disorder Examples (Harrison's, 22nd ed.)
| Mixed Disorder | Key Finding | Classic Example |
|---|---|---|
| High-AG acidosis + respiratory alkalosis | PaCO2 below predicted | Sepsis-related lactic acidosis in ICU |
| High-AG acidosis + respiratory acidosis | PaCO2 above predicted | Severe pneumonia or pulmonary edema |
| Metabolic alkalosis + respiratory alkalosis | pH much higher than expected | End-stage liver disease + diuretics |
| Metabolic alkalosis + respiratory acidosis | PaCO2 high, pH near-normal; both PaCO2 and HCO3- abnormal | COPD patient on diuretics |
| High-AG acidosis + metabolic alkalosis | ΔAG >> ΔHCO3- | DKA with vomiting; uremia with vomiting |
Causes of Each Primary Disorder
Metabolic Acidosis (High-AG)
MUDPILES: Methanol - Uremia - DKA/starvation - Propylene glycol - Isoniazid/Iron - Lactic acidosis - Ethylene glycol - Salicylates
Metabolic Acidosis (Normal-AG / Hyperchloremic)
HARDUP: Hyperalimentation - Acetazolamide - Renal tubular acidosis - Diarrhea - Ureteroenteric diversion - Pancreatic fistula
Lactic acidosis is the most common cause of wide-AG metabolic acidosis, accounting for ~50% of cases. - Rosen's Emergency Medicine
Metabolic Alkalosis
Chloride-responsive (urine Cl- < 20): Vomiting, NG suction, contraction alkalosis, diuretics (prior use)
Chloride-unresponsive (urine Cl- > 20): Hyperaldosteronism, Cushing's, Bartter/Gitelman syndrome, Mg2+ deficiency, severe hypokalemia
Respiratory Acidosis
- Primary lung disease (COPD, pneumonia, pulmonary edema)
- Chest wall disease (flail chest, obesity hypoventilation)
- Respiratory muscle weakness (Guillain-Barré, myopathies, hypokalemia, hypophosphatemia)
- Decreased respiratory drive (CNS lesions, opioids, sedatives)
- Mechanical ventilation (iatrogenic hypoventilation)
Respiratory Alkalosis
- Anxiety/hyperventilation (most common ER presentation)
- Hypoxemia-induced hyperventilation (PE, pneumonia at altitude)
- Salicylate toxicity (early), hepatic encephalopathy, sepsis
- CNS disease (stroke, tumor), pregnancy
- Mechanical ventilation (iatrogenic hyperventilation)
Clinical note: Acute respiratory alkalosis causes hypocalcemia symptoms (paresthesias, carpal-pedal spasm, syncope) from increased albumin-calcium binding. - Rosen's Emergency Medicine
Worked Clinical Examples
Example 1 - Diarrhea
Values: pH 7.26, PaCO2 13, HCO3- 5, Na 133, K 2.8, Cl 118
- pH < 7.35 → acidemia
- HCO3- low → metabolic acidosis
- Check compensation: ΔPaCO2 = 1.3 × (25-5) = 26; predicted PaCO2 = 40-26 = 14 ≈ measured 13 ✓
- AG = 133 - (118+5) = 10 → normal anion gap (hyperchloremic from diarrhea - GI HCO3- loss)
- Diagnosis: Simple metabolic acidosis with appropriate respiratory compensation (diarrhea)
Roberts and Hedges' Clinical Procedures, p. 4824
Example 2 - Sepsis (Respiratory Alkalosis)
Values: pH 7.49, PaCO2 25, HCO3- 22, Na 138, K 3.2, Cl 105
- pH > 7.45 → alkalemia
- PaCO2 low → respiratory alkalosis
- Acute compensation: ΔHCO3- = -2 × (40-25)/10 = -3; expected HCO3- = 24-3 = 21 ≈ 22 ✓
- Diagnosis: Acute respiratory alkalosis (typical of early sepsis/anxiety)
Roberts and Hedges' Clinical Procedures, p. 4862
Example 3 - Mixed: Lactic Acidosis + Respiratory Alkalosis (Sepsis ICU)
Values: Na 140, K 4.0, Cl 106, HCO3- 14, AG 20, PaCO2 24, pH 7.39
- pH near normal but AG = 20 (elevated) → high-AG metabolic acidosis present
- PaCO2 < predicted for metabolic acidosis alone → additional respiratory alkalosis
- The near-normal pH is a false reassurance - two disorders are fighting each other
- Diagnosis: Mixed high-AG metabolic acidosis + respiratory alkalosis (sepsis)
Harrison's Principles, 22nd ed.
Example 4 - COPD + Diuretics (Mixed Metabolic Alkalosis + Respiratory Acidosis)
Values: Na 140, K 3.5, Cl 88, HCO3- 42, AG 10, PaCO2 67, pH 7.42
- pH essentially normal but PaCO2 markedly elevated and HCO3- markedly elevated
- Normal pH in this setting indicates two opposing processes
- Diagnosis: Mixed metabolic alkalosis (diuretics) + respiratory acidosis (COPD)
Harrison's Principles, 22nd ed.
Osmolar Gap (Extra Tool in Toxic Alcohol Ingestion)
$$Osmolar Gap = Measured Osmolality - Calculated Osmolarity$$
$$Calculated = 2[Na^+] + \frac{Glucose}{18} + \frac{BUN}{2.8} + \frac{EtOH}{3.7}$$
- Normal osmolar gap < 10 mOsm/kg
- Elevated gap + high-AG metabolic acidosis → suspect methanol or ethylene glycol
- Estimated ethylene glycol concentration (mg/dL) ≈ osmolar gap × 6
Rosen's Emergency Medicine
Venous vs. Arterial Blood Gas
| Parameter | Arterial-Venous Correlation |
|---|---|
| pH | VBG closely correlates (difference ≤ 0.05) - clinically useful |
| PaCO2 | VBG trends correlate; difference up to ±20 mmHg - less reliable |
| PaO2 | Does NOT correlate - never use VBG to assess oxygenation |
| Lactate | Normal/markedly high venous lactate correlates; mildly elevated may not |
- Tintinalli's Emergency Medicine, p. 122
ABG Management Principles
The key steps to managing any acid-base disorder are:
- Identify the type of disorder(s) present
- Identify the underlying cause
- Treat the cause - not just the pH
- For DKA: insulin (not just bicarbonate)
- For lactic acidosis from sepsis: restore perfusion
- For toxic alcohol: specific antidotes (fomepizole)
- NaHCO3 is a reasonable adjunct in severe metabolic acidosis from bicarbonate loss or renal failure, while the underlying cause is addressed
Rosen's Emergency Medicine
Quick Reference Summary Card
Normal ABG: pH 7.35-7.45 | PaCO2 35-45 | HCO3- 22-26 | PaO2 80-100
STEP 1: Oxygenate? → PaO2, SaO2, A-a gradient
STEP 2: pH → acidemia or alkalemia?
STEP 3: Primary disorder? → PaCO2 (resp) vs HCO3- (metabolic)
STEP 4: Compensation adequate? → Use formulas / Rule of 15
STEP 5: Anion gap? → AG = Na - (Cl + HCO3-) [normal 8-12]
STEP 6: Delta-delta? → Hidden 2nd metabolic disorder?
STEP 7: Osmolar gap? → If toxic ingestion suspected
If compensation ≠ expected → MIXED DISORDER
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine, 22nd ed.; Tintinalli's Emergency Medicine; Harriet Lane Handbook, 23rd ed.
Here is a Geeky Medics video walking through ABG interpretation with an OSCE approach:
This is a shared conversation. Sign in to Orris to start your own chat.