Ecg reader
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative material from multiple textbooks. Here is a complete guide to ST elevation and STEMI on ECG:
ST Elevation & STEMI - ECG Guide
Why Does ST Elevation Happen?
Severe transmural (full-thickness) ischemia lowers the resting membrane potential and shortens action potential duration in affected myocytes. This creates a voltage gradient between ischemic and normal tissue, generating a current of injury. The ST vector shifts outward toward the epicardium - overlying leads record ST elevation.

Panel A = subendocardial ischemia → ST depression. Panel B = transmural ischemia → ST elevation. (Harrison's, 22e)
Diagnostic Criteria for STEMI (4th Universal Definition, 2018)
New ST elevation at the J-point in ≥2 contiguous leads:
| Leads | Cutoff |
|---|---|
| All leads except V2-V3 | ≥ 1 mm (0.1 mV) |
| V2-V3 in men ≥40 yrs | ≥ 2 mm (0.2 mV) |
| V2-V3 in men <40 yrs | ≥ 2.5 mm (0.25 mV) |
| V2-V3 in women (any age) | ≥ 1.5 mm (0.15 mV) |
A new (or presumed new) LBBB is treated as a STEMI equivalent.
The presence of reciprocal ST depression in mirror leads strongly supports the diagnosis and helps distinguish true STEMI from mimics. - Symptom to Diagnosis, 4e
Localization by Lead Territory
| Affected Wall | Leads with ST Elevation | Reciprocal Depression | Likely Culprit Artery |
|---|---|---|---|
| Anterior | V1-V4 | II, III, aVF | LAD (proximal) |
| Anterolateral | V1-V6, I, aVL | II, III, aVF | LAD or LCx |
| High lateral | I, aVL | III, aVF | LCx or 1st diagonal |
| Inferior | II, III, aVF | I, aVL | RCA (most common) or LCx |
| Posterior | Reciprocal ST depression V1-V3 + tall R wave | - | RCA or LCx |
| Right ventricular | II, III, aVF + right-sided leads (V3R-V4R) | Lateral leads | Proximal RCA |
| Left main / multivessel | aVR (>0.5 mV) + diffuse ST depression | - | LMCA |
Posterior STEMI tip: ST depression in V1-V3 with a dominant R wave is a "STEMI equivalent" - flip those leads 180° mentally and you'll see the elevation.
Temporal Evolution of ECG Changes
- Minutes: Hyperacute T waves (tall, peaked, broad) - earliest sign, often missed
- Hours: ST elevation develops at the J-point
- Hours-Days: T-wave inversions appear in the same leads as the ST elevation
- Days-Weeks: Pathologic Q waves develop (transmural necrosis)
- Weeks-Months: ST elevation usually resolves; persistent elevation suggests ventricular aneurysm
ACS Pathway (Diagnosis Framework)
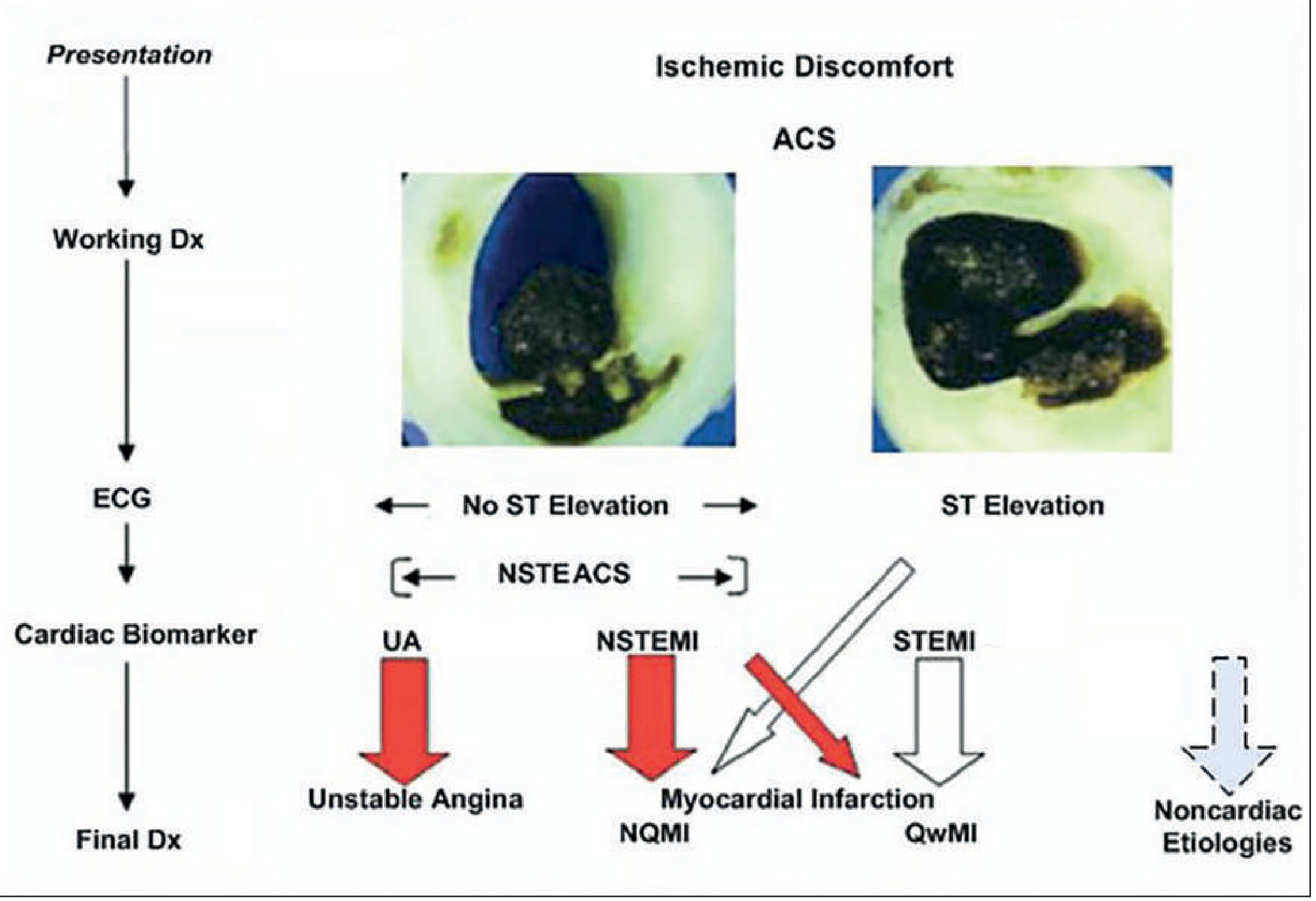
Goldman-Cecil Medicine
Pathologic Q Waves (Criteria)
- In V2-V3: Q wave ≥0.02 sec, or QS complex
- In all other leads: Q wave ≥0.03 sec AND ≥1 mm deep, in ≥2 contiguous leads
- Not an indication for reperfusion on their own - compare with old ECG to determine chronicity
Washington Manual
STEMI Differentials - When ST Elevation Is NOT a STEMI
| Cardiac | Non-Cardiac |
|---|---|
| Pericarditis (diffuse, saddle-shaped, PR depression) | Pulmonary embolism |
| Myocarditis | Hyperkalemia |
| LV aneurysm (persistent STE with old Q waves) | - |
| Hypertrophic cardiomyopathy | - |
| Brugada syndrome (V1-V2, coved pattern) | - |
| Early repolarization (normal variant - J-point notch, no reciprocal changes) | - |
| Prinzmetal/vasospasm angina | - |
| Aortic dissection with coronary involvement | - |
Always get an old ECG for comparison - it is often the single most useful step in sorting out chronic from acute STE.
Special Patterns
- De Winter pattern: J-point depression + upsloping ST depression + tall peaked T waves in precordial leads + ST elevation in aVR - proximal LAD occlusion, treat as STEMI equivalent
- aVR elevation: ST elevation ≥0.5 mV in aVR with diffuse depression elsewhere - 78% sensitive, 83% specific for left main disease
- Posterior STEMI: V7-V9 placement (posterior leads) shows ST elevation >0.5 mm when standard leads only show reciprocal V1-V3 depression
Diagnostic Performance of ECG in Chest Pain
From Symptom to Diagnosis, 4e:
- New ST elevation >1 mm: LR+ = 5.7-53 (very high specificity)
- Any ST elevation: LR+ = 11.2
- 80% of ED chest pain patients with new 1 mm ST elevation have confirmed MI
Key Action Thresholds
- ECG must be obtained and interpreted within 10 minutes of ED arrival when MI is suspected
- Do not wait for troponin results before activating the STEMI pathway - treatment decisions are made on ECG findings
- Thrombolytics are contraindicated in NSTEMI (no benefit, added risk)
- Primary PCI is preferred over thrombolysis when door-to-balloon time can be achieved within guideline targets
Sources: Harrison's Principles of Internal Medicine 22e | Goldman-Cecil Medicine | Rosen's Emergency Medicine | Washington Manual of Medical Therapeutics | Symptom to Diagnosis 4e | Textbook of Family Medicine 9e
In hindi
ST Elevation और STEMI - ECG गाइड (हिंदी में)
ST Elevation क्यों होता है?
जब हृदय की मांसपेशी को पूरी तरह खून नहीं मिलता (transmural ischemia), तो प्रभावित कोशिकाओं में electrical changes आते हैं। इससे एक "current of injury" बनता है - ST vector बाहर की तरफ (epicardium की ओर) shift होता है, और overlying leads में ST elevation दिखता है।

- Panel A = अंदरी परत में ischemia → ST नीचे जाता है
- Panel B = पूरी दीवार में ischemia → ST ऊपर जाता है
(Harrison's Principles of Internal Medicine, 22e)
STEMI की ECG Diagnostic Criteria
(4th Universal Definition, 2018)
J-point पर ≥2 contiguous (साथ वाले) leads में नया ST elevation:
| Leads | कितना Elevation चाहिए |
|---|---|
| V2-V3 को छोड़कर सभी leads | ≥ 1 mm (0.1 mV) |
| V2-V3 - पुरुष ≥40 साल | ≥ 2 mm (0.2 mV) |
| V2-V3 - पुरुष <40 साल | ≥ 2.5 mm (0.25 mV) |
| V2-V3 - महिला (किसी भी उम्र) | ≥ 1.5 mm (0.15 mV) |
नया LBBB (Left Bundle Branch Block) भी STEMI equivalent माना जाता है।
Reciprocal ST depression (mirror leads में ST का नीचे जाना) - यह असली STEMI की पहचान है और diagnosis confirm करता है।
कौन सी Lead में Elevation = कौन सी दीवार प्रभावित
| प्रभावित दीवार | जहाँ ST Elevation | Reciprocal Depression | Culprit Artery |
|---|---|---|---|
| Anterior (आगे) | V1-V4 | II, III, aVF | LAD (proximal) |
| Anterolateral | V1-V6, I, aVL | II, III, aVF | LAD या LCx |
| High Lateral | I, aVL | III, aVF | LCx या 1st Diagonal |
| Inferior (नीचे) | II, III, aVF | I, aVL | RCA (ज़्यादातर) |
| Posterior (पीछे) | V1-V3 में ST depression + tall R | - | RCA या LCx |
| Right Ventricle | II, III, aVF + V3R-V4R | Lateral leads | Proximal RCA |
| Left Main / Multivessel | aVR में elevation + सब जगह depression | - | LMCA |
Posterior STEMI याद रखने का तरीका:
V1-V3 में ST depression + बड़ा R wave = पीछे की दीवार का STEMI - इन leads को उल्टा पढ़ो, elevation नज़र आएगा।
ECG में समय के साथ बदलाव (Temporal Evolution)
| समय | ECG बदलाव |
|---|---|
| मिनटों में | Hyperacute T waves - लंबी, नुकीली, चौड़ी (सबसे पहला संकेत, अक्सर miss हो जाता है) |
| घंटों में | J-point पर ST elevation दिखना शुरू |
| घंटे - दिन | T wave inversion (उन्हीं leads में जहाँ ST elevation था) |
| दिन - हफ्ते | Pathologic Q waves बनते हैं (transmural necrosis की निशानी) |
| हफ्ते - महीने | ST elevation ठीक हो जाता है; अगर बना रहे → Ventricular Aneurysm सोचें |
ACS का पूरा Flow
- ST Elevation + Biomarkers बढ़े → STEMI
- ST Elevation नहीं + Biomarkers बढ़े → NSTEMI
- ST Elevation नहीं + Biomarkers नहीं बढ़े → Unstable Angina
(Goldman-Cecil Medicine)
Pathologic Q Wave की पहचान
- V2-V3 में: Q wave ≥0.02 sec, या QS complex
- बाकी सभी leads में: Q wave ≥0.03 sec और ≥1 mm गहरा, ≥2 contiguous leads में
- Q wave अकेले reperfusion therapy का indication नहीं है
- पुरानी ECG से compare करें - यह सबसे ज़रूरी कदम है
ST Elevation के दूसरे कारण (STEMI नहीं)
Cardiac कारण:
| कारण | कैसे पहचानें |
|---|---|
| Pericarditis | Diffuse leads में saddle-shaped STE + PR depression |
| Brugada Syndrome | V1-V2 में coved pattern, right bundle branch block |
| LV Aneurysm | पुराने Q waves के साथ persistent STE |
| Early Repolarization | J-point notch, कोई reciprocal changes नहीं, युवा healthy व्यक्ति |
| Prinzmetal Angina | Vasospasm, आता-जाता रहता है |
| HCM / Aortic Stenosis | Strain pattern |
Non-Cardiac कारण:
- Pulmonary Embolism - RV strain pattern, S1Q3T3
- Hyperkalemia - peaked T waves पहले, फिर wide QRS + STE
Special Patterns जो याद रखने चाहिए
De Winter Pattern (LAD Occlusion का संकेत)
- Precordial leads में J-point depression + upsloping ST depression + tall T waves
- aVR में ST elevation
- STEMI equivalent माना जाता है - proximal LAD occlusion
aVR Elevation (Left Main Disease)
- aVR में ST elevation ≥0.5 mm + बाकी जगह diffuse depression
- Left Main Coronary Artery disease के लिए 78% sensitive, 83% specific
Clinical Action Points
| क्या करें | कब |
|---|---|
| ECG करो और interpret करो | ED में आते ही 10 मिनट के अंदर |
| STEMI pathway activate करो | ECG criteria पूरे होते ही - Troponin का इंतज़ार मत करो |
| Primary PCI | पहली पसंद - जहाँ available हो |
| Thrombolysis | जब PCI उपलब्ध न हो; NSTEMI में बिल्कुल नहीं |
| पुरानी ECG देखो | हमेशा - chronic vs acute STE की पहचान के लिए |
ECG की Diagnostic Value (Chest Pain में)
- नई ST elevation >1 mm: LR+ = 5.7 से 53 (बहुत high specificity)
- जिन ED patients को नई 1mm ST elevation हो, उनमें 80% को confirmed MI होता है
- नई ST depression या T inversion: सिर्फ 20% को MI
(Symptom to Diagnosis, 4e)
Sources: Harrison's 22e | Goldman-Cecil Medicine | Rosen's Emergency Medicine | Washington Manual | Symptom to Diagnosis 4e | Textbook of Family Medicine 9e
ST Elevation के साथ patients को manage करने की protocol
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
मेरे पास अब सभी ज़रूरी जानकारी है। अब पूरी STEMI Management Protocol हिंदी में प्रस्तुत करता हूँ।
STEMI Management Protocol - हिंदी में पूरी गाइड
याद रखें: STEMI एक medical emergency है। बिना इलाज के mortality >30% होती है। जितना जल्दी reperfusion, उतनी जान बचती है।
⏱️ Time is Muscle - हर मिनट मायने रखता है
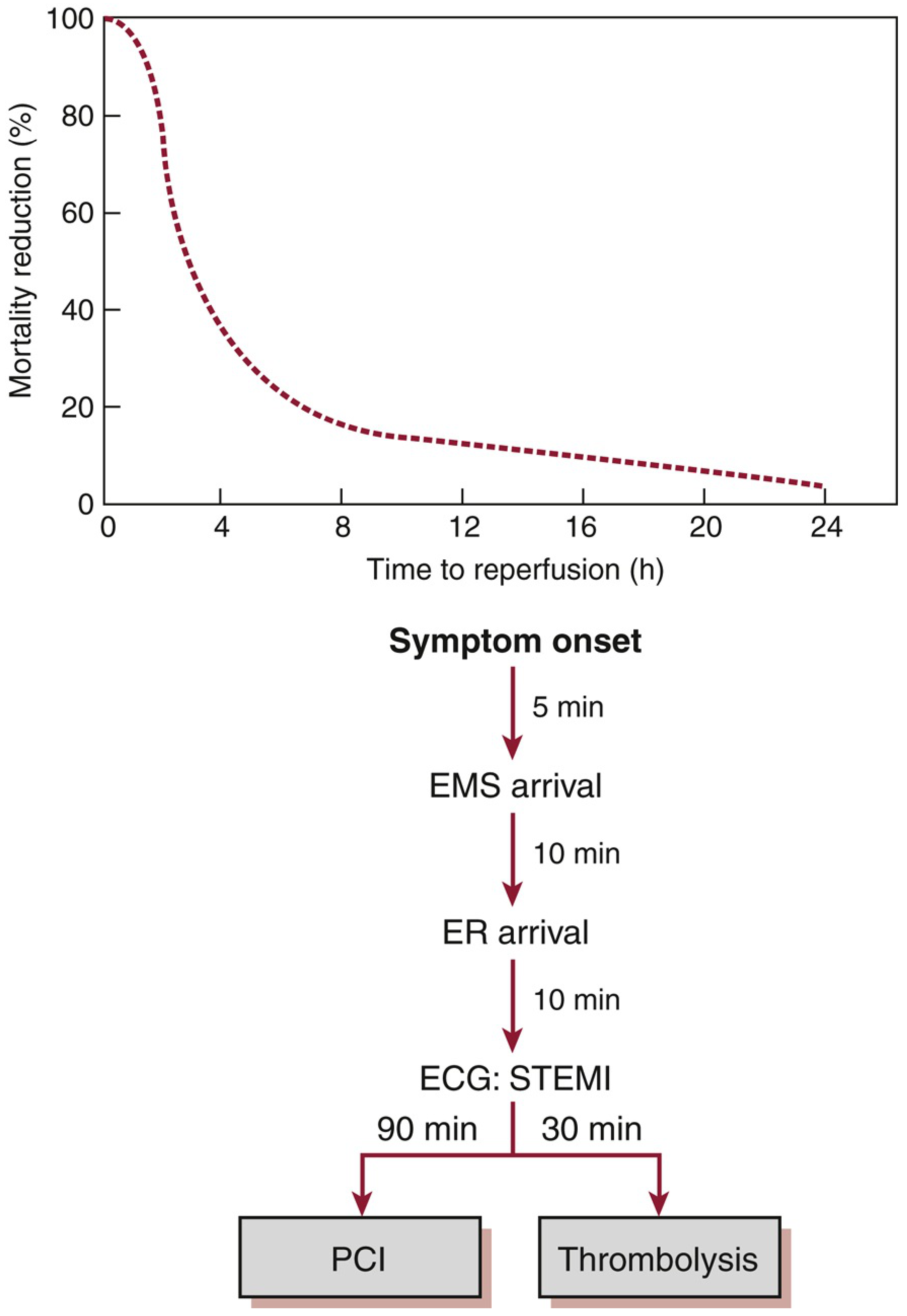
| समयसीमा (Time Target) | लक्ष्य |
|---|---|
| ED में आने के बाद ECG | ≤ 10 मिनट |
| Door-to-Balloon (Primary PCI) | ≤ 90 मिनट |
| Door-to-Needle (Thrombolysis) | ≤ 30 मिनट |
STEP 1 - तुरंत शुरुआती कदम (First 10 Minutes)
A - Assessment
- 12-lead ECG - 10 मिनट के अंदर
- STEMI criteria confirm करें
- Troponin का इंतज़ार मत करो - treatment ECG पर based है
- Vitals, SpO₂, IV access (2 lines), Telemetry
- Portable Chest X-Ray (aortic dissection rule out)
- Labs: Troponin, CBC, BMP, Coagulation, Lipid panel, Magnesium
B - Contraindications Check करें
- Aortic dissection तो नहीं? (ST elevation के साथ tearing chest pain → पहले dissection rule out)
- Thrombolytics के contraindications check करें
C - Oxygen
- SpO₂ < 90% हो तभी Oxygen दें - routine oxygen नहीं देनी (harm हो सकता है)
STEP 2 - Upstream Medical Therapy (सभी STEMI patients को तुरंत)
(Reperfusion strategy decide होने से पहले यह सब शुरू करें)
| दवा | Dose | ज़रूरी बात |
|---|---|---|
| Aspirin (ASA) | 162-325 mg चबाकर | Non-enteric-coated tablet - जल्दी absorb होती है |
| P2Y12 Inhibitor (एक चुनें) | देखें नीचे | PCI vs Thrombolysis के हिसाब से चुनें |
| Anticoagulant | देखें नीचे | - |
| Nitroglycerin | 0.4 mg SL, हर 5 min × 3 dose | SBP < 90, RV infarction, या Sildenafil use में बिल्कुल नहीं |
| Morphine | 2-4 mg IV PRN | सिर्फ refractory pain में; nitroglycerin से राहत नहीं मिले तो |
| Beta-Blocker (BB) | Metoprolol 12.5-25 mg PO | पहले 24 घंटे में दें - अगर कोई contraindication नहीं |
P2Y12 Inhibitors - कौन सा, कब?
| दवा | Loading Dose | Maintenance | कब दें |
|---|---|---|---|
| Clopidogrel | 600 mg | 75 mg/day | Thrombolysis के साथ; या PCI |
| Prasugrel | 60 mg | 10 mg/day | PCI के साथ (>75 yr, <60 kg, stroke/TIA में मत दो) |
| Ticagrelor | 180 mg | 90 mg BD | PCI के साथ; ASA dose 100 mg से ज़्यादा नहीं |
Anticoagulants - कौन सा, कब?
| दवा | Dose | कब |
|---|---|---|
| UFH (Unfractionated Heparin) | 60 U/kg IV bolus (max 4000 U), फिर 12 U/kg/hr (max 1000 U/hr); aPTT target 1.5-2× | PCI या Thrombolysis दोनों के साथ |
| Enoxaparin (LMWH) | 30 mg IV bolus + 1 mg/kg SC q12h | Thrombolysis के साथ preferred; >75 yr: loading नहीं, 0.75 mg/kg SC |
| Bivalirudin | 0.75 mg/kg IV bolus, 1.75 mg/kg/hr | सिर्फ PCI के साथ |
| Fondaparinux | 2.5 mg IV, फिर 2.5 mg SC daily | Thrombolysis के साथ - UFH से कम bleeding |
Beta-Blocker कब नहीं देना (Contraindications):
- SBP < 120 mmHg
- Heart rate > 110 या < 60
- नई Heart Failure / Pulmonary edema
- Cardiogenic Shock (Killip Class II या इससे ऊपर)
- Age > 70 years
- Advanced Heart Block
STEP 3 - Reperfusion Strategy चुनें
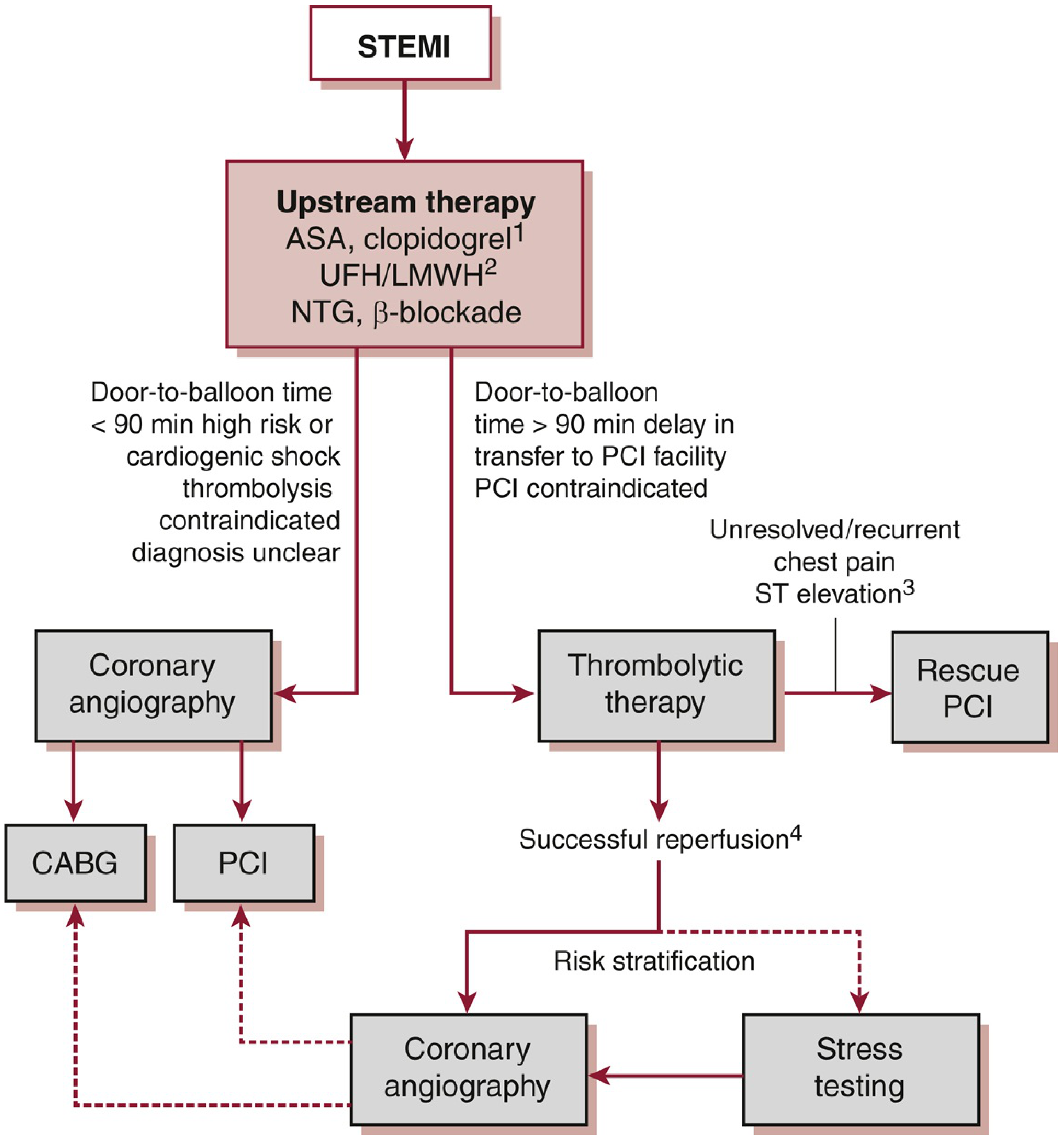
Option A - Primary PCI (पहली पसंद)
कब करें:
- Door-to-balloon time ≤ 90 मिनट संभव हो
- Cardiogenic shock हो
- Thrombolysis contraindicated हो
- Diagnosis unclear हो
- Symptoms > 2-3 घंटे पुराने हों (clot lyse करना मुश्किल)
फायदे:
- Thrombolysis से बेहतर artery खुलती है
- Short-term और long-term outcomes बेहतर
- Bleeding का खतरा कम
Non-culprit vessels:
- Shock नहीं है → Non-culprit PCI भी करें (उसी दिन या 45 दिन के अंदर) - PRAMI, COMPLETE trials
- Cardiogenic shock है → सिर्फ culprit artery का PCI करें (non-culprit PCI में mortality बढ़ती है)
Option B - Thrombolysis (जब PCI उपलब्ध नहीं)
कब करें:
- Primary PCI ≤ 120 मिनट में संभव नहीं
- Door-to-balloon > 90 मिनट की देरी हो
लक्ष्य: Door-to-Needle ≤ 30 मिनट
Thrombolytic Drugs:
| दवा | Dose | विशेष बात |
|---|---|---|
| Tenecteplase (TNK) | Weight-based (30-50 mg IV single bolus) | Bolus - आसान; preferred |
| Alteplase (tPA) | 15 mg bolus → 50 mg over 30 min → 35 mg over 60 min | UFH के साथ दें |
| Reteplase (rPA) | 10 U IV, 30 min बाद 10 U IV | Double bolus |
| Streptokinase | 1.5 million IU IV over 60 min | Cheap; anaphylaxis का खतरा; UFH की ज़रूरत नहीं |
Absolute Contraindications:
- Intracranial hemorrhage का history
- Known intracranial tumor या vascular lesion
- Active bleeding (menses छोड़कर)
- 3 महीने के अंदर ischemic stroke
- Suspected aortic dissection
- 3 महीने के अंदर significant head/face trauma
Relative Contraindications:
- SBP > 180 mmHg या DBP > 110 mmHg (uncontrolled)
- CPR > 10 min, recent surgery < 3 weeks
- Pregnancy
- High INR (anticoagulation पर)
- Streptokinase - पहले इस्तेमाल किया हो या allergy हो
Successful Reperfusion के Signs (60-90 मिनट बाद देखें):
- ✅ Chest pain में राहत
- ✅ ST elevation में ≥50% कमी
- ✅ Reperfusion arrhythmia (idioventricular rhythm)
अगर Thrombolysis fail हो → Rescue PCI करें अगर:
- Chest pain बना रहे
- ST elevation normal न हो
- Unstable arrhythmias
- Heart failure develop हो
STEP 4 - Admission Orders (CCU में)
| Category | Details |
|---|---|
| Ward | Coronary Care Unit (CCU) with continuous telemetry |
| Vitals | हर घंटे जब तक stable नहीं; SpO₂ monitoring ≥24 hr |
| Activity | Bed rest ≥12 hr; Stable होने पर light activity |
| Diet | NPO initially; pain-free होने पर 2g Na, heart-healthy diet |
| Notify | HR >100 या <50; SBP <90 या >150; SpO₂ <90%; RR <8 या >20 |
| IV | D5W या NS - keep vein open; 2 lines |
STEP 5 - Arrhythmia Management
| Arrhythmia | Treatment |
|---|---|
| VF / Pulseless VT | Unsynchronized DC shock 200 J (biphasic) immediately |
| Sustained VT (hemodynamically stable) | Amiodarone 150 mg IV over 10 min → 1 mg/min × 6 hr → 0.5 mg/min |
| Isolated VPCs | कोई treatment नहीं - prophylactic antiarrhythmics contraindicated |
| Bradycardia / Heart Block | Atropine; temporary pacing if needed |
| Electrolytes | K⁺ ≥ 4.5 mmol/L रखें; Mg²⁺ ≥ 2.0 mmol/L रखें |
याद रखें: VF STEMI में 50% mortality का कारण है और अक्सर पहले घंटे में होती है - इसीलिए early monitoring ज़रूरी है।
STEP 6 - Special Situations
Right Ventricular (RV) Infarction
- Inferior STEMI (II, III, aVF) के साथ suspect करें
- V3R-V4R leads लगाएं (ST >0.5 mm = RV infarction)
- Signs: JVD + Hypotension + Clear lungs (Kussmaul's sign)
- Treatment: IV fluids (volume expansion) - nitrates और diuretics बिल्कुल नहीं (preload drop होगी, shock बढ़ेगा)
Cardiogenic Shock
- Dopamine / Norepinephrine vasopressors
- IABP (Intra-aortic balloon pump) consider करें
- Early PCI - लेकिन non-culprit PCI नहीं
Posterior STEMI (अक्सर miss होता है)
- V7-V9 leads लगाएं - ST >0.5 mm = posterior STEMI
- V1-V3 में ST depression + tall R wave देखें
- Treatment same as STEMI
STEP 7 - Secondary Prevention (Discharge पर)
| दवा | Duration | कारण |
|---|---|---|
| Aspirin 75-100 mg | आजीवन | 27% reduction in recurrent MI/stroke/CV death |
| P2Y12 inhibitor (DAPT) | 12 महीने (Clopidogrel/Prasugrel/Ticagrelor) | STEMI के बाद standard care |
| Statin (high-intensity) | आजीवन | LDL <70 mg/dL target |
| Beta-Blocker | आजीवन (EF कम हो तो) | Arrhythmia protection, remodeling prevention |
| ACE Inhibitor / ARB | आजीवन (HF/LV dysfunction में) | Ventricular remodeling रोकता है |
| Aldosterone antagonist | EF ≤40% + HF/Diabetes में | Eplerenone/Spironolactone |
Lifestyle Changes:
- Smoking बंद - सबसे ज़रूरी
- Cardiac rehabilitation program
- Exercise tolerance के हिसाब से activity बढ़ाएं
- Uncomplicated STEMI: 2-4 हफ्तों में काम पर वापसी
- Normal sexual activity 1-2 हफ्तों में शुरू कर सकते हैं
Quick Summary - "MONA-B" याद रखें
| Letter | Drug |
|---|---|
| M | Morphine (pain के लिए, PRN) |
| O | Oxygen (सिर्फ SpO₂ <90% पर) |
| N | Nitroglycerin |
| A | Aspirin (चबाकर) + Anticoagulant |
| B | Beta-Blocker + second antiplatelet (P2Y12) |
फिर → Reperfusion (PCI first choice, Thrombolysis if PCI not available)
Sources: Washington Manual of Medical Therapeutics | Harrison's Principles of Internal Medicine 22e | Goldman-Cecil Medicine | Textbook of Family Medicine 9e | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.