Diabetes mellitus type 1 and type 2 difference
Reading File
Finding Sources
Searching PubMed
"type 1 diabetes" AND "type 2 diabetes" AND differences
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and diagrams. Here is the full, detailed comparison:
Type 1 vs. Type 2 Diabetes Mellitus
Overview
Diabetes mellitus is defined as elevated blood glucose associated with absent or inadequate pancreatic insulin secretion, with or without concurrent impairment of insulin action. The four recognized categories are: Type 1, Type 2, other specific types, and gestational diabetes. - Katzung's Basic and Clinical Pharmacology, 16th Ed.
At-a-Glance Comparison Table
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| Prevalence | 5-10% of all DM | 90-95% of all DM |
| Age of onset | Any age, most common in children & young adults | More common with advancing age; can occur in children/adolescents |
| Mechanism | Autoimmune destruction of beta cells → absolute insulin deficiency | Insulin resistance + progressive relative insulin deficiency |
| Autoimmunity | Yes (CD4+/CD8+ T cells, macrophages; insulitis) | No |
| Autoantibodies | GAD65, IA-2, IAA, ZnT8 (present in >90%) | Absent |
| C-peptide | Very low or undetectable | Detectable (though decreases over time) |
| Beta cell mass | Near-total destruction | Reduced but not eliminated |
| HLA association | Strong (DR4-DQ8, DR3-DQ2 in ~90% of children) | Not HLA-linked |
| Twin concordance | ~30-40% in identical twins | ~80-90% in identical twins |
| Ketoacidosis risk | High (insulin is essential to prevent ketosis) | Low (enough insulin to prevent ketosis in most cases) |
| Body habitus | Usually normal weight | Often overweight/obese |
| Onset | Usually acute/symptomatic | Often insidious; may be asymptomatic for years |
| First-line treatment | Insulin (absolutely required) | Lifestyle changes, oral agents (metformin first-line), insulin as needed |
- Henry's Clinical Diagnosis and Management by Laboratory Methods
Pathogenesis
Type 1 DM - Autoimmune Beta Cell Destruction
In T1DM, a complex interplay of genetic, environmental, and autoimmune factors selectively targets and destroys insulin-producing pancreatic islet beta cells. This leads to an absolute deficiency of insulin. - Goldman-Cecil Medicine
How it happens:
- Beta cell destruction is mediated primarily by CD8+ and CD4+ T cells, macrophages, and antibodies causing apoptosis. The lymphocytic infiltration of the islets is called insulitis.
- Over time, the islets become completely devoid of beta cells, while other pancreatic cell types remain intact - illustrating the specificity of the autoimmune attack.
- Autoantibodies to GAD65, IA-2, IAA, and ZnT8 are found in >90% of newly diagnosed patients. The presence of two or more antibodies in normoglycemic relatives is highly predictive of T1DM within 5 years.
Stages of T1DM progression (Robbins & Kumar):
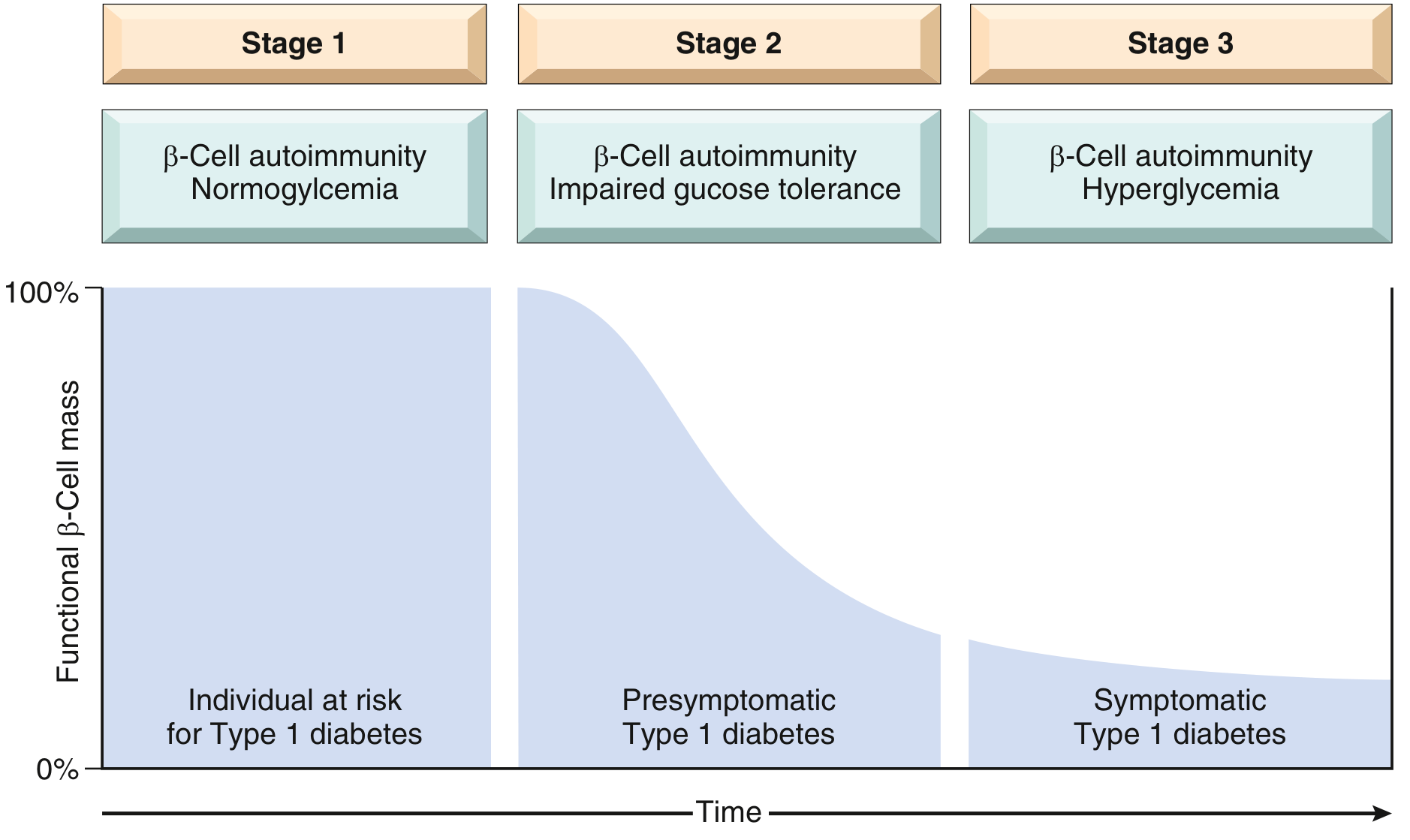
Genetic factors:
- About 60 T1DM susceptibility genes are known. HLA genes on chromosome 6p contribute ~50% of genetic susceptibility.
- Haplotypes DR4-DQ8 and DR3-DQ2 are present in ~90% of children with T1DM.
- The DR15-DQ6 haplotype is protective - found in only 1% of T1DM children vs. 20% of the general population.
- 30-40% concordance in identical twins (vs. 80-90% in T2DM), indicating a significant environmental trigger component.
Environmental triggers:
- Epidemics of mumps, rubella, and coxsackievirus have been associated with increased T1DM frequency - these viruses may contain molecules resembling beta-cell proteins, triggering autoimmunity in genetically predisposed individuals.
- Increased new-onset T1DM presenting as acute hyperglycemic emergencies was observed during the SARS-CoV-2 pandemic. - Goldman-Cecil Medicine
Type 2 DM - Insulin Resistance + Beta Cell Dysfunction
T2DM involves two core defects:
- Decreased ability of peripheral tissues (liver, muscle, adipose) to respond to insulin - insulin resistance
- Beta cell dysfunction - inadequate insulin secretion despite insulin resistance and hyperglycemia - Robbins & Kumar Basic Pathology
How it happens:
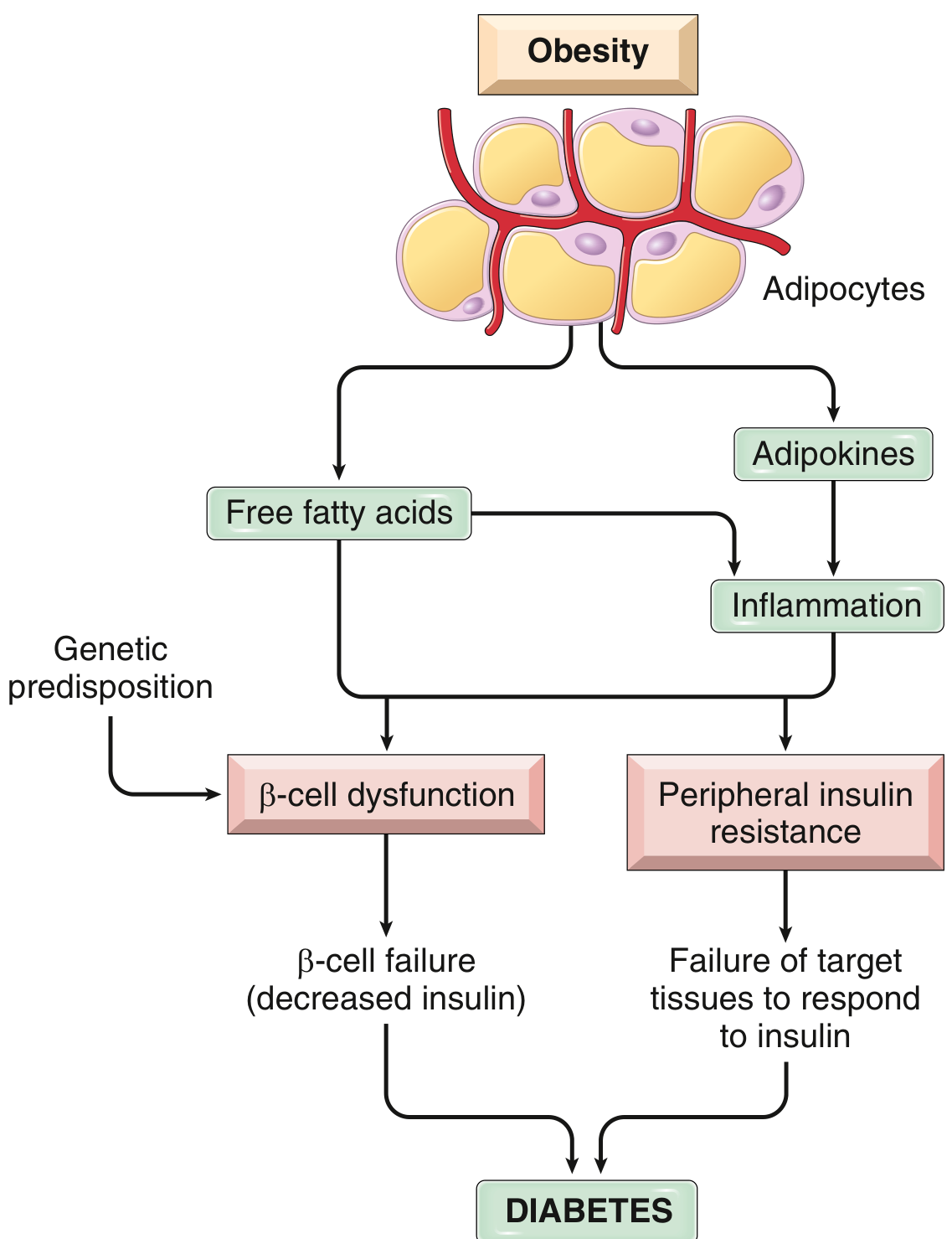
- Obesity-driven free fatty acids and adipokines cause inflammation, promoting both peripheral insulin resistance and beta cell dysfunction.
- T2DM is not an autoimmune disease - no insulitis, no islet-directed antibodies.
- T2DM is NOT linked to HLA genes; rather, dozens of diabetogenic genes identified in genome-wide association studies contribute.
- The circulating endogenous insulin is sufficient to prevent ketoacidosis but inadequate to prevent hyperglycemia.
A given T2DM patient may have predominantly insulin resistance or predominantly beta cell failure - the disease is heterogeneous. - Katzung's Pharmacology, 16th Ed.
Clinical Presentation
| Type 1 DM | Type 2 DM | |
|---|---|---|
| Symptoms at onset | Often acute: polyuria, polydipsia, polyphagia, weight loss, fatigue | Often asymptomatic for years; diagnosis may follow routine screening or after complications develop |
| DKA | Common (life-threatening emergency at onset or during illness) | Rare; hyperosmolar hyperglycemic state (HHS) more typical |
| Weight | Usually normal or low | Usually overweight or obese |
| Acanthosis nigricans | Absent | May be present (marker of insulin resistance) |
| Associated conditions | Other autoimmune diseases (thyroid, celiac, Addison's) | Metabolic syndrome, hypertension, dyslipidemia, PCOS, NAFLD |
Diagnosis
Both types are diagnosed by the same criteria:
- Fasting glucose ≥126 mg/dL
- 2-hour glucose ≥200 mg/dL on OGTT
- HbA1c ≥6.5%
- Random glucose ≥200 mg/dL with symptoms
Differentiating labs:
- C-peptide: near-zero in T1DM; measurable in T2DM
- Autoantibodies (GAD65, IA-2, ZnT8): positive in T1DM; absent in T2DM
Treatment
| Type 1 DM | Type 2 DM | |
|---|---|---|
| Insulin | Absolutely required; multiple daily injections (MDI) or insulin pump | Often needed as disease progresses, but not always initially |
| Oral agents | Not used as primary therapy | Metformin (first-line); followed by sulfonylureas, DPP-4 inhibitors, SGLT-2 inhibitors, GLP-1 agonists, etc. |
| Lifestyle | Important for glucose management | Central to treatment and prevention (weight loss, exercise) |
| Prevention | No proven method; teplizumab (anti-CD3 antibody) delays onset by ~25 months in high-risk Stage 2 patients aged ≥8 years | Lifestyle modification (weight loss + exercise) and metformin can prevent or delay onset in high-risk individuals |
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Important Special Note: LADA
Latent Autoimmune Diabetes of Adulthood (LADA) is a milder, slower-progressing form of T1DM that initially resembles T2DM. Up to 10-15% of patients diagnosed as "type 2" in northern Europeans may actually have LADA. These patients retain enough beta cell function initially to avoid ketosis but eventually require insulin as beta cell function declines. Autoantibody testing (especially GAD65) distinguishes LADA from true T2DM. - Katzung's Pharmacology, 16th Ed.
Complications
Both types share the same spectrum of complications due to hyperglycemia:
- Microvascular: diabetic retinopathy, nephropathy, neuropathy
- Macrovascular: coronary artery disease, stroke, peripheral artery disease
- T2DM patients are often diagnosed after complications are already present, because onset is insidious
Sources:
- Goldman-Cecil Medicine (International Edition, 2-volume set)
- Robbins & Kumar Basic Pathology
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Katzung's Basic and Clinical Pharmacology, 16th Edition
This is a shared conversation. Sign in to Orris to start your own chat.