Esophagus varicesls
Reading File
Finding Sources
Searching PubMed
"esophageal varices"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from authoritative textbooks. Let me compile the full answer.
Esophageal Varices
Definition and Pathophysiology
Esophageal varices are dilated submucosal veins in the lower esophagus that develop as collateral channels when portal hypertension elevates portal venous pressure. They are most commonly a complication of cirrhosis (especially alcohol-associated liver disease) but can also result from any cause of portal hypertension (pre-hepatic, intrahepatic, or post-hepatic).
The key hemodynamic threshold is the hepatic venous pressure gradient (HVPG):
- Normal HVPG: 1-5 mm Hg
- Varices form at HVPG > 10 mm Hg
- Risk of bleeding is virtually absent when HVPG < 12 mm Hg
- HVPG > 20 mm Hg is a predictor of treatment failure and death
Epidemiology and Natural History
- Esophageal varices are present in ~40% of all cirrhotic patients, and up to 60% of those with cirrhosis + ascites
- In cirrhotic patients without varices at initial endoscopy, new varices develop at ~5% per year
- Progression from small to large varices: ~10% per year, related to degree of liver dysfunction
- Alcohol abstinence can lead to decrease or even disappearance of varices
Bleeding risk:
- Up to 25% of patients with newly diagnosed varices will bleed within 2 years
- Varices < 5 mm: 7% bleeding risk at 2 years
- Varices > 5 mm: 30% bleeding risk at 2 years
- Once bleeding occurs, initial treatment controls bleeding in 80-90% of cases
- ~50% stop bleeding spontaneously (hypovolemia → splanchnic vasoconstriction → ↓ portal pressure)
- ~1/3 of patients who stopped bleeding will rebleed within 6 weeks
- Mortality: 5-8% at 1 week; ~20% at 6 weeks
(Sleisenger and Fordtran's Gastrointestinal and Liver Disease)
Classification (Grading)
| Size | Description |
|---|---|
| Small | < 5 mm, flat or slightly raised above mucosa |
| Large | > 5 mm, tortuous, occupy >1/3 of esophageal lumen |
Endoscopic risk signs for imminent bleeding include:
- Cherry-red spots
- Red wale signs
- Hematocystic spots
Management Framework
Treatment is classified into three phases:
1. Primary Prophylaxis (Prevention of First Bleed)
Primary prophylaxis algorithm:
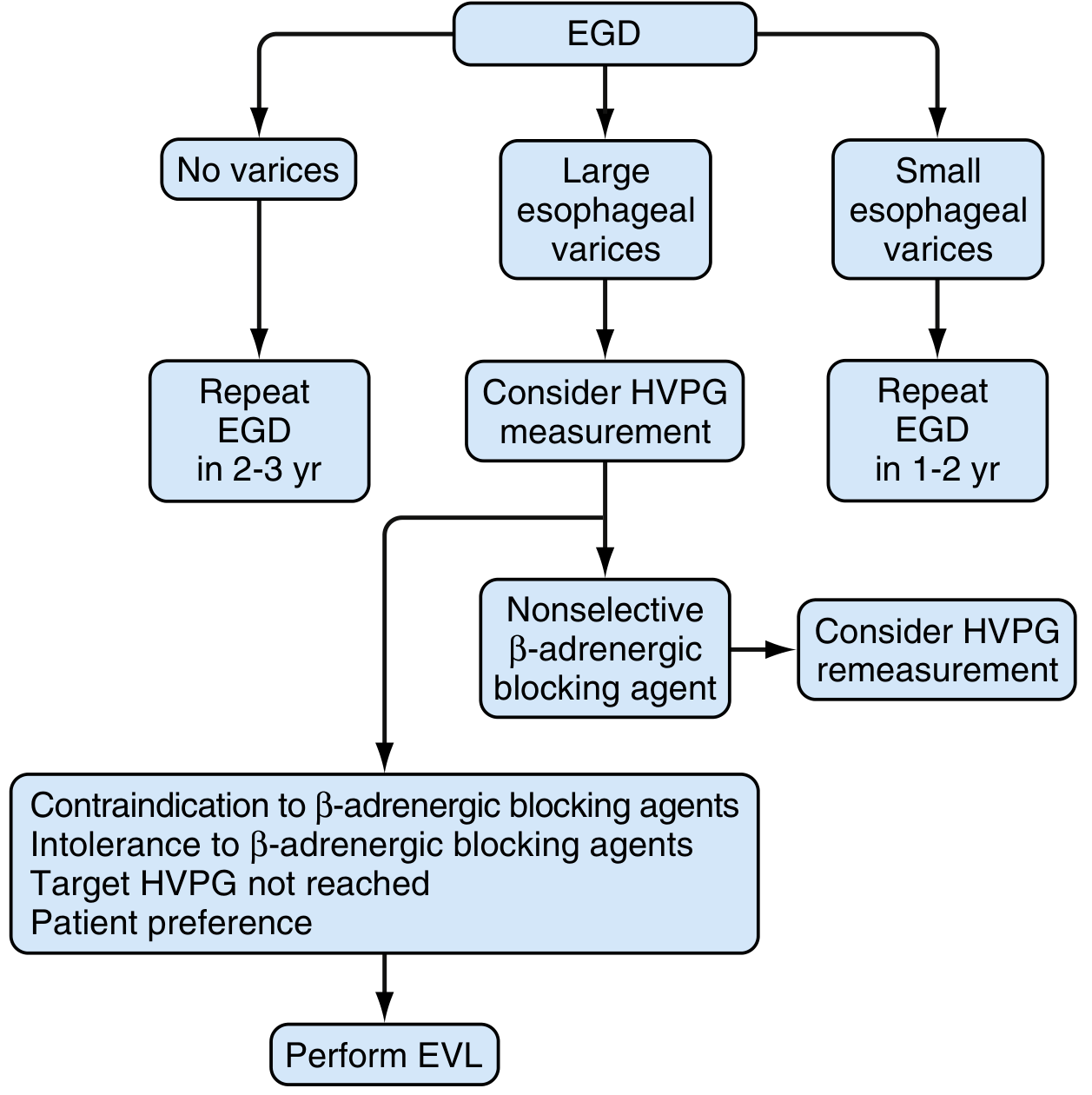
Fig. 92.13 - Algorithm for primary prophylaxis of esophageal variceal bleeding (Sleisenger & Fordtran)
Pharmacologic (Beta-Blockers):
- Non-selective beta-blockers (propranolol, nadolol, carvedilol) are first-line for large varices
- Starting dose: long-acting propranolol 60 mg once daily or nadolol 20 mg once daily (evening dosing preferred - bleeding risk is greatest at night)
- Titrate every 3-5 days to target heart rate 55-60 bpm or 25% below baseline, as long as systolic BP stays > 90 mm Hg
- Carvedilol (initial 6.25 mg/day, max 25 mg/day) preferred in patients with hypertension or coronary artery disease
- Goal: HVPG reduction to < 12 mm Hg or ≥ 20% decrease
- Only 30-40% of patients respond to beta-blockers; patients with better liver function respond best
Endoscopic (EVL):
- Endoscopic variceal ligation (EVL/band ligation) is used when beta-blockers are contraindicated, not tolerated, or HVPG target is not reached
- Repeat EGD every 1-2 weeks until variceal obliteration, then surveillance every 3-6 months
- Note: Prophylactic sclerotherapy cannot be recommended due to higher complication rates
2. Acute Variceal Bleeding - Emergency Management
This is a life-threatening emergency requiring a multidisciplinary team (hepatology, endoscopy, ICU, radiology, surgery).
Resuscitation:
- Two large-bore IV lines immediately
- Restrictive transfusion strategy: transfuse packed RBCs only when Hgb < 7 g/dL (associated with improved survival vs. transfusing at < 9 g/dL in Child-Pugh A/B)
- Target hematocrit ~25% - avoid excessive transfusions (increase risk of hypocoagulability and portal pressure rebound)
- Normal saline until blood products available
- Airway protection: endotracheal intubation for active bleeders
- Correct coagulopathy as needed
Antibiotic prophylaxis (mandatory for all patients):
- Norfloxacin 400 mg PO twice daily × 7 days (preferred)
- If unavailable (e.g., USA): ciprofloxacin 500 mg PO twice daily × 7 days
- If oral intake not possible: IV ceftriaxone 1 g every 24 hours × 7 days, or IV ciprofloxacin 400 mg every 12 hours
- Failure to control infection significantly increases mortality and rebleeding risk
Vasoactive pharmacologic therapy (start as early as possible - even in transit):
- Octreotide - most common in the USA (reduces splanchnic blood flow)
- Terlipressin - preferred in many countries; only agent associated with improved survival
- Somatostatin or vapreotide - alternatives
- Continue vasoactive agents for up to 5 days to prevent early rebleeding
- Combination of endoscopic + vasoactive therapy is superior to either alone
Endoscopy (EGD):
- Perform as soon as patient is hemodynamically stabilized
- Endoscopic variceal ligation (EVL) is the preferred treatment at time of initial endoscopy
- Variceal bleeding confirmed if: active spurting/oozing from varix, white fibrin plug or red clot over varix, risk signs (cherry-red spot, hematocystic spot, red wale sign), or varices without any other bleeding source
Salvage therapy:
- Balloon tamponade (Sengstaken-Blakemore tube): temporizing measure when endoscopy fails or is unavailable - gastric balloon inflates first to occlude the gastroesophageal junction, then esophageal balloon if needed
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): preferred definitive rescue procedure; as effective as distal splenorenal shunt for Child-Pugh A cirrhosis
- Surgical portosystemic shunt: reserved for centers without TIPS expertise
3. Secondary Prophylaxis (Prevention of Rebleeding)
Secondary prophylaxis algorithm:
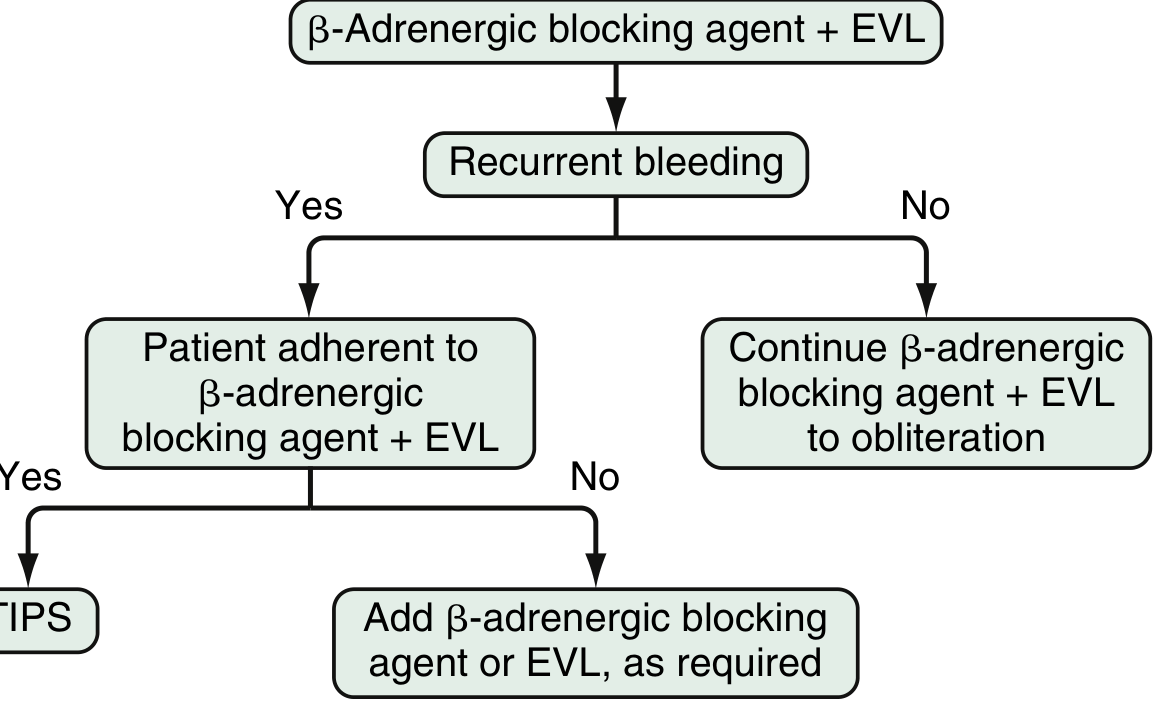
Fig. 92.16 - Algorithm for prevention of recurrent esophageal variceal bleeding (Sleisenger & Fordtran)
- Standard of care: combination of non-selective beta-blocker + EVL (superior to either alone)
- Beta-blocker + EVL reduces rebleeding in Child-Pugh A patients; reduces mortality in Child-Pugh B and C
- If recurrent bleeding despite optimal pharmacologic + endoscopic therapy → TIPS or portosystemic shunt
- Patients with rebleeding, MELD > 18, > 4 units pRBC transfusion, or renal failure have highest mortality risk
Predictors of Poor Outcome
| Factor | Significance |
|---|---|
| HVPG > 20 mm Hg | Failure to control bleeding, death |
| Active bleeding at endoscopy | Failure, rebleeding |
| MELD > 18 | High mortality |
| Renal failure | High mortality |
| > 4 units pRBC needed | High mortality |
| Bacterial infection | Rebleeding, mortality |
| Child-Pugh C | Poor prognosis |
| Portal vein thrombosis | Failure to control |
| Gastric varices (vs. esophageal) | Higher rebleed risk |
Gastric Varices (Sarin Classification)
| Type | Description |
|---|---|
| GOV1 | Extend 2-5 cm below GEJ, continuous with esophageal varices (~70% of all gastric varices) |
| GOV2 | Cardia/fundus, continuous with esophageal varices |
| IGV1 | Isolated fundal varices (e.g., splenic vein thrombosis) |
| IGV2 | Isolated varices in gastric body, antrum, or pylorus |
- Gastric varices bleed less often but with greater severity
- Preferred treatment for bleeding gastric varices: cyanoacrylate glue injection (not banding)
(Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Tintinalli's Emergency Medicine)
This is a shared conversation. Sign in to Orris to start your own chat.