Explain tuberculosis
Reading File
Finding Sources
Searching PubMed
tuberculosis pathogenesis treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Antituberculotic drugs
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer on antituberculotic drugs.
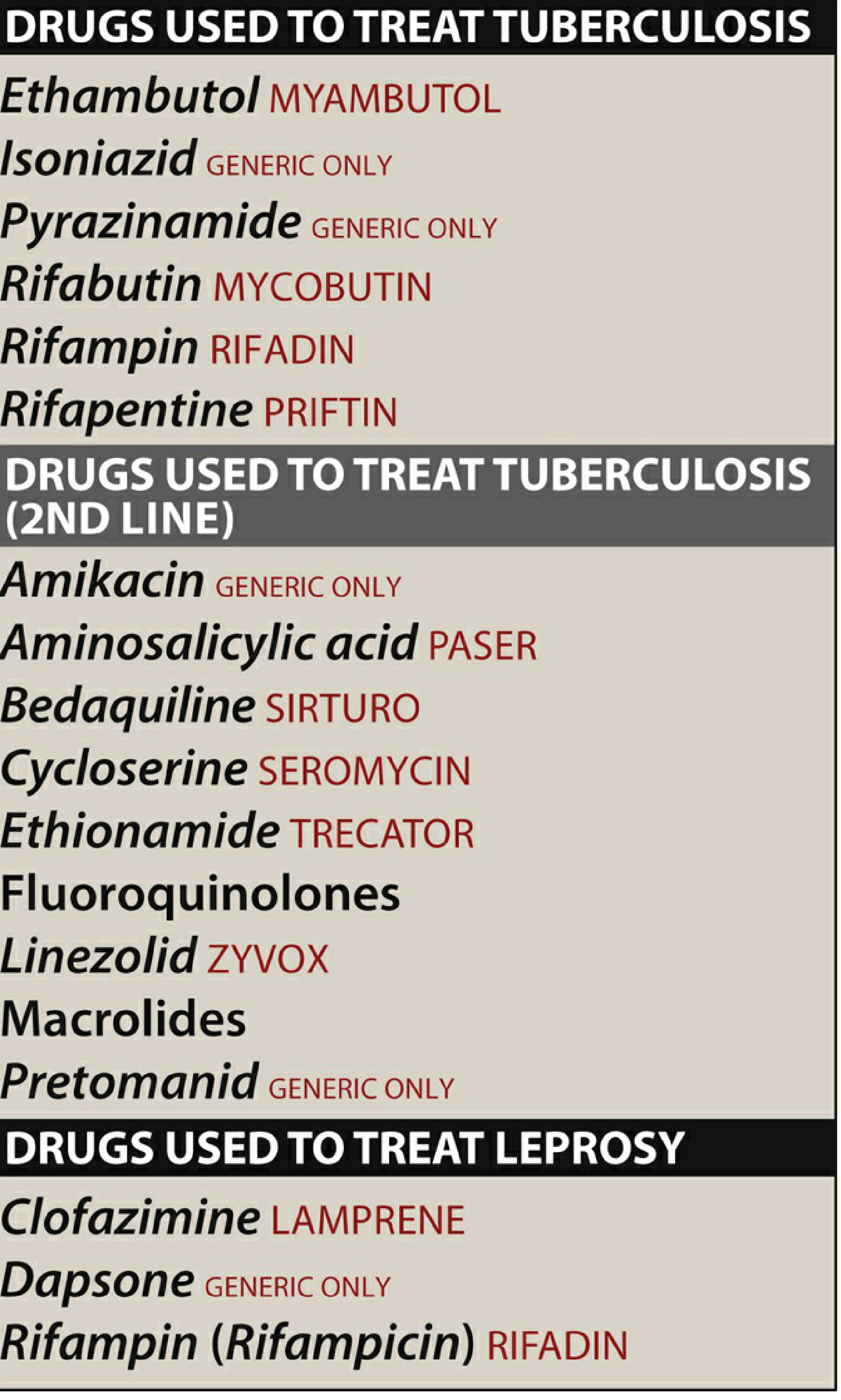
Antituberculotic Drugs
Overview
M. tuberculosis is intrinsically resistant to most antibiotics because it grows slowly, can exist in a dormant state, has a lipid-rich cell wall that is impermeable to many agents, and lives intracellularly inside macrophages. For these reasons, combination therapy with at least two (and usually four) drugs is mandatory to prevent emergence of resistance. Treatment must continue for months because of "persister" organisms that survive in a drug-tolerant state. - Katzung's Basic and Clinical Pharmacology, 16e
Treatment Regimens
Standard 6-Month Regimen (Drug-Susceptible Active TB)
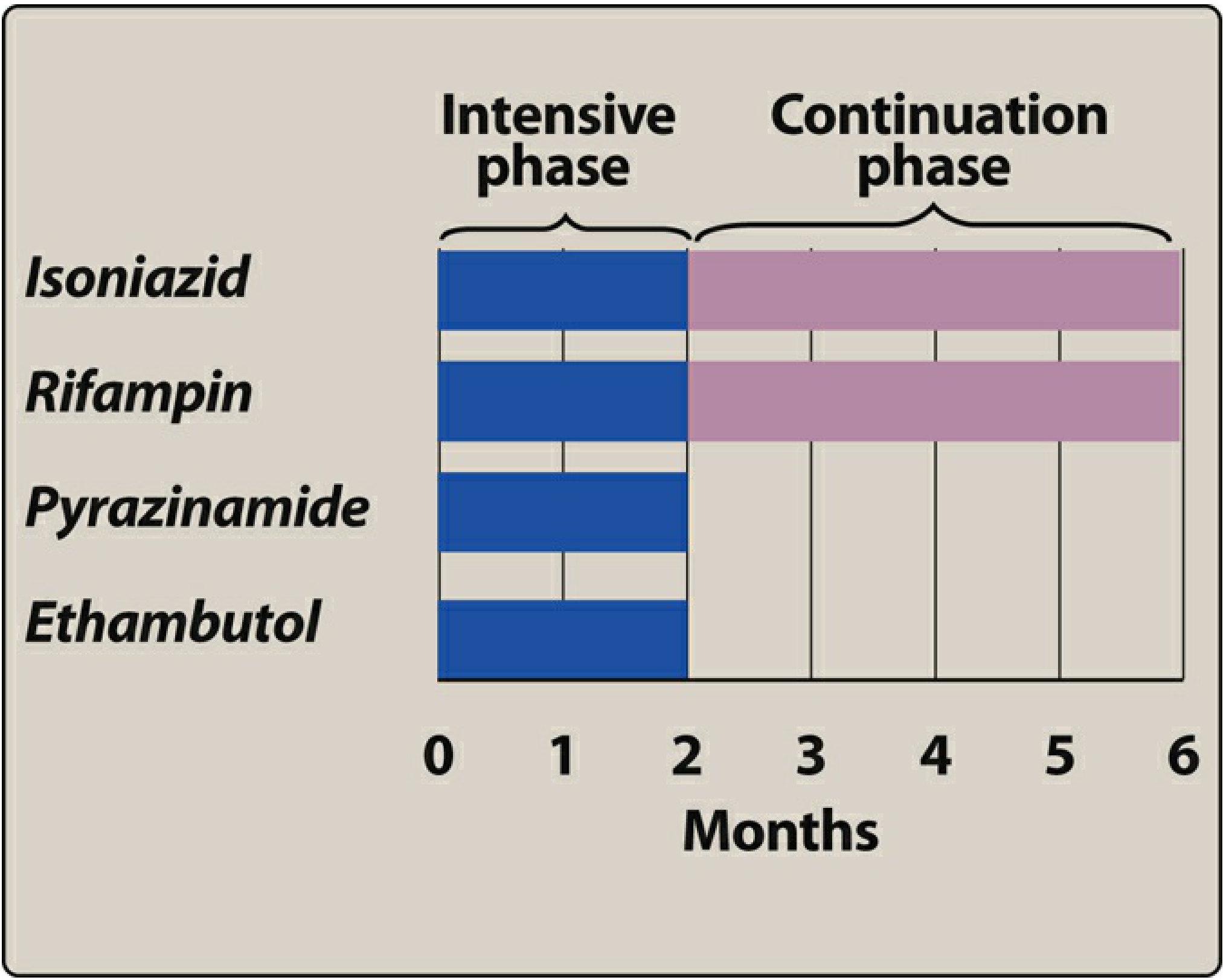
- Intensive phase (months 1-2): Isoniazid + Rifampin + Pyrazinamide + Ethambutol (RIPE)
- Continuation phase (months 3-6): Isoniazid + Rifampin
The four-drug intensive phase covers against isoniazid or rifampin resistance while susceptibility results are pending. Pyrazinamide shortens the total treatment duration. Ethambutol does not reduce duration further but protects against pre-existing resistance.
Newer 4-Month Regimen
Rifapentine + Moxifloxacin + Isoniazid + Pyrazinamide (PMIP) - approved as an alternative for drug-susceptible pulmonary TB in patients ≥12 years weighing ≥40 kg.
Latent TB (LTBI) Options
- 3 months of once-weekly isoniazid + rifapentine
- 4 months of daily rifampin (monotherapy acceptable for LTBI)
- 6-9 months of daily isoniazid monotherapy
- Lippincott Illustrated Reviews: Pharmacology
First-Line Drugs
1. Isoniazid (INH)
Dose: 300 mg/day orally (adult)
Mechanism of action: INH is a prodrug activated by a mycobacterial catalase-peroxidase enzyme (KatG). The activated form inhibits InhA (enoyl-ACP reductase) and KasA (β-ketoacyl-ACP synthase), both essential enzymes in mycolic acid synthesis. This collapses the mycobacterial cell wall. - Lippincott Pharmacology
Spectrum: Highly specific for M. tuberculosis (and M. kansasii at higher concentrations). Very effective against rapidly dividing bacilli and intracellular organisms.
Resistance: Mutations in katG (prevents prodrug activation), mutations in inhA or kasA, or overexpression of InhA. Cross-resistance with ethionamide is possible.
Pharmacokinetics:
- Well absorbed orally; absorption impaired by fatty food
- Penetrates all body fluids, caseous material, and CSF (CSF levels ≈ serum levels)
- Undergoes N-acetylation in the liver - genetically regulated
- Fast acetylators: half-life ~90 minutes
- Slow acetylators: half-life 3-4 hours (higher plasma levels, more neuropathy risk)
- Excreted renally as metabolites
Adverse effects:
| Effect | Details |
|---|---|
| Hepatitis | Most serious; incidence rises with age (0.3% age 21-35, up to 2.3% over 50), alcohol use, co-administration with rifampin |
| Peripheral neuropathy | Due to pyridoxine (B6) deficiency - prevent with pyridoxine 10-25 mg/day |
| CNS toxicity | Memory loss, psychosis, seizures (rare) |
| Drug interactions | Inhibits CYP2E1/CYP2C19 - raises phenytoin and carbamazepine levels (nystagmus, ataxia) |
2. Rifampin (Rifampicin)
Dose: 600 mg/day orally (10 mg/kg/day)
Mechanism of action: Binds the β-subunit of bacterial DNA-dependent RNA polymerase, blocking RNA transcription. Human RNA polymerase is not affected. Bactericidal for both intracellular and extracellular mycobacteria. Penetrates phagocytes and abscesses. - Katzung
Resistance: Point mutations in rpoB (gene encoding β-subunit of RNA polymerase) reduce rifampin binding. Resistance to rifampin is the main proxy marker for MDR-TB. Complete cross-resistance exists within the rifamycin class (rifabutin, rifapentine).
Pharmacokinetics:
- Well absorbed orally; undergoes enterohepatic recycling
- Deacetylated metabolite excreted mainly in feces; small amount in urine
- Potent inducer of CYP450 enzymes and P-glycoprotein - major source of drug interactions
- Undergoes autoinduction: its own half-life shortens over the first 1-2 weeks
- Colors urine, sweat, saliva, sputum, and tears orange-red (warn patients; soft contact lenses may be permanently stained)
Adverse effects:
- Hepatitis (rare but potentially fatal; use with caution in liver disease)
- GI upset, rash
- Flu-like syndrome with intermittent/high-dose therapy (fever, chills, myalgias, hemolytic anemia, thrombocytopenia, acute renal failure) - seen with dosing less than twice weekly
- Thrombocytopenia, nephritis, cholestatic jaundice
Other uses: Meningococcal prophylaxis (600 mg × 2 days); H. influenzae b contacts; staphylococcal prosthetic device infections.
3. Rifapentine (Rifamycin analogue)
Dose: 1200 mg once daily (4-month regimen); 600 mg once weekly (LTBI regimen with INH)
Same mechanism as rifampin (RNA polymerase inhibitor). Elimination half-life ~13 hours (longer than rifampin). Less induction of CYP450 enzymes when dosed intermittently. Used in the 4-month PMIP regimen and in the 3-month once-weekly LTBI regimen with isoniazid. Toxicity profile similar to rifampin.
4. Rifabutin
An alternative to rifampin in patients on HIV antiretrovirals (especially protease inhibitors) because it is a weaker CYP450 inducer and there are fewer interactions with antiretroviral drugs.
5. Ethambutol
Dose: 15-25 mg/kg/day orally
Mechanism of action: Inhibits arabinosyl transferase (EmbB), an enzyme responsible for arabinogalactan synthesis - a key component of the mycobacterial cell wall. This impairs polymerization of arabinose into arabinan. - Katzung
Role: Primarily bacteriostatic. Included in the initial four-drug regimen as a "protective" fourth drug pending susceptibility results. Also used for MAC and M. kansasii infections.
Resistance: Rapidly emerges when used as monotherapy; always combine.
Adverse effects:
- Retrobulbar (optic) neuritis - most serious; causes loss of visual acuity and red-green color blindness. Dose-dependent: more common at 25 mg/kg/day. Monitor visual acuity and color vision at baseline and monthly.
- Relatively contraindicated in young children who cannot reliably report visual changes.
- Hypersensitivity reactions are rare.
6. Pyrazinamide (PZA)
Dose: 25 mg/kg/day orally
Mechanism of action: A pyridine analogue of nicotinamide. It is inactive at neutral pH but at pH 5.5 (within acidic macrophage lysosomes) it inhibits tubercle bacilli. It is a prodrug: mycobacterial pyrazinamidase (encoded by pncA) converts it to pyrazinoic acid, which disrupts mycobacterial membrane metabolism and transport. - Katzung
Key property: Specifically active against organisms residing inside macrophages in the acidic lysosomal environment. This is why PZA is indispensable during the first 2 months - it kills a population of bacilli that other drugs cannot easily reach.
Resistance: Mutations in pncA that impair drug conversion; impaired PZA uptake.
Pharmacokinetics:
- Well absorbed orally; distributed to all tissues including inflamed meninges
- Half-life 8-11 hours
- Renally cleared metabolites; reduce dosing frequency in CrCl <30 mL/min
Adverse effects:
- Hyperuricemia (most common) - inhibits renal tubular secretion of uric acid; may precipitate gout
- Hepatotoxicity (dose-dependent) - monitor LFTs
- Nausea, rash, arthralgias
- Fever, photosensitivity
Second-Line Drugs
Used when first-line drugs fail, cause intolerable toxicity, or when MDR-TB/XDR-TB is present.
| Drug | Mechanism | Key Toxicity |
|---|---|---|
| Cycloserine | Inhibits D-alanine synthesis (cell wall) | CNS toxicity: depression, anxiety, psychosis, seizures. Monitor renal function. |
| Ethionamide | Inhibits mycolic acid synthesis (InhA, similar to INH) | GI intolerance (majority of patients), hepatotoxicity, hypothyroidism. Cross-resistance with INH possible. |
| Para-aminosalicylic acid (PAS) | Inhibits folate synthesis and iron acquisition by mycobacteria | GI intolerance, hepatotoxicity, hypothyroidism. Risk of hemolytic anemia in G6PD deficiency. |
| Aminoglycosides (Amikacin, Kanamycin, Streptomycin) | Bind 30S ribosome; inhibit protein synthesis | Nephrotoxicity, ototoxicity (vestibular and auditory). Not available orally. |
| Capreomycin | Cyclic polypeptide; inhibits protein synthesis (similar site to aminoglycosides) | Nephrotoxicity, ototoxicity. |
| Fluoroquinolones (Levofloxacin, Moxifloxacin) | Inhibit DNA gyrase (topoisomerase II/IV) | GI intolerance, tendonitis, QTc prolongation, CNS effects. Avoid with antacids. |
| Linezolid | Inhibits 50S ribosome (protein synthesis) | Bone marrow suppression, peripheral neuropathy, optic neuritis with prolonged use. |
Newer Drugs for MDR/XDR-TB
Bedaquiline (Sirturo)
- Mechanism: Inhibits mycobacterial ATP synthase (subunit c) - completely novel target, no cross-resistance with other drugs
- Dose: 400 mg/day × 2 weeks, then 200 mg 3×/week × 22 weeks (with food)
- Toxicities: Nausea, arthralgia, headache; hepatotoxicity; QT prolongation (FDA black-box warning)
- Indicated for pulmonary MDR-TB when other options are not available
Pretomanid (FDA approved 2019)
- Mechanism: Nitroimidazole - requires bacterial reduction to become active
- Under aerobic conditions (replicating bacteria): inhibits mycolic acid synthesis
- Under anaerobic conditions (dormant bacteria): releases reactive nitrogen species toxic to intracellular organisms
- Dose: 200 mg/day orally; half-life ~16 hours
- Used as part of the BPaL regimen (Bedaquiline + Pretomanid + Linezolid) for 6 months for XDR-TB and treatment-nonresponsive MDR-TB
- Metabolized by CYP3A4; avoid potent CYP3A4 inducers
Summary: Mechanisms by Drug Target
| Target | Drug(s) |
|---|---|
| Mycolic acid synthesis | Isoniazid, Ethionamide, Pretomanid (aerobic) |
| Cell wall (arabinan) | Ethambutol |
| RNA polymerase | Rifampin, Rifapentine, Rifabutin |
| DNA gyrase | Fluoroquinolones |
| Protein synthesis (30S) | Streptomycin, Amikacin, Kanamycin, Capreomycin |
| Protein synthesis (50S) | Linezolid |
| D-alanine synthesis | Cycloserine |
| ATP synthase | Bedaquiline |
| Membrane/transport (acid pH) | Pyrazinamide |
Mnemonic for First-Line Drugs
RIPE = Rifampin + Isoniazid + Pyrazinamide + Etambutol
Key Monitoring Points
- INH: Baseline LFTs; pyridoxine supplementation to prevent neuropathy; watch for hepatitis
- Rifampin: Baseline LFTs + CBC; warn about orange body fluids; extensive drug interactions
- Ethambutol: Baseline and monthly visual acuity + red-green color vision
- Pyrazinamide: Baseline LFTs and uric acid; watch for gout
- Bedaquiline: ECG monitoring (QTc); liver function
Sources: Katzung's Basic and Clinical Pharmacology, 16e; Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.