
bef6bfc2-bf77-43b6-a1f9-3d3fb3ef0ab2.jpeg
ok so im starting ans pharmacology so i want everything in detail topics wise and the attached photo is my syllabus so one my one start the explanation
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
TOPIC 1: Introduction to Autonomic Pharmacology
Your syllabus covers 5 major topics. We start with Topic 1. Let me know when you want Topic 2 and I'll continue.
1. What is the Autonomic Nervous System (ANS)?
The ANS is the division of the peripheral nervous system that controls involuntary functions - things you never have to consciously think about: heart rate, blood pressure, digestion, glandular secretions, smooth muscle tone, and more.
It is sometimes called the "involuntary nervous system" because it operates without conscious effort. It innervates:
- Smooth muscle (blood vessels, gut, bladder, bronchi)
- Cardiac muscle and pacemaker cells
- Exocrine and endocrine glands
- Adipose tissue and liver
Important: Skeletal muscle is the ONLY innervated structure NOT controlled by the ANS.
The ANS has 3 divisions:
- Sympathetic nervous system (fight-or-flight)
- Parasympathetic nervous system (rest-and-digest)
- Enteric nervous system (gut)
2. Anatomy - The Two-Neuron Chain
Unlike the somatic system (which uses a single neuron from CNS to skeletal muscle), the ANS uses a two-neuron chain at every autonomic pathway:
| Preganglionic neuron | Postganglionic neuron | |
|---|---|---|
| Origin | CNS (brain or spinal cord) | Autonomic ganglion |
| Fibre type | Myelinated (B-fibre) | Unmyelinated (C-fibre) |
| Neurotransmitter | Acetylcholine (ACh) - ALWAYS | NE (sympathetic) / ACh (parasympathetic) |
3. Sympathetic vs. Parasympathetic - Key Differences
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Outflow | Thoracolumbar (T1-L2) | Craniosacral (CN III, VII, IX, X; S2-S4) |
| Ganglia location | Near vertebral column (paravertebral/prevertebral) - FAR from effector | Near or within effector organ - CLOSE to effector |
| Preganglionic fibre | Short | Long |
| Postganglionic fibre | Long | Short |
| Postganglionic NT | Norepinephrine (NE) | Acetylcholine (ACh) |
| Effector receptor | Adrenergic receptor | Muscarinic receptor |
One exception: Sympathetic postganglionic fibres to sweat glands and to some blood vessels use ACh (not NE). These are called "sympathetic cholinergic" fibres.
Adrenal medulla exception: The adrenal medulla is directly innervated by preganglionic fibres (no postganglionic neuron). Stimulation releases epinephrine (80%) + norepinephrine (20%) directly into the bloodstream - acting like an endocrine organ.
4. Neurotransmitters and Receptor Summary
Here is the master diagram from Lippincott's Pharmacology - study this carefully:
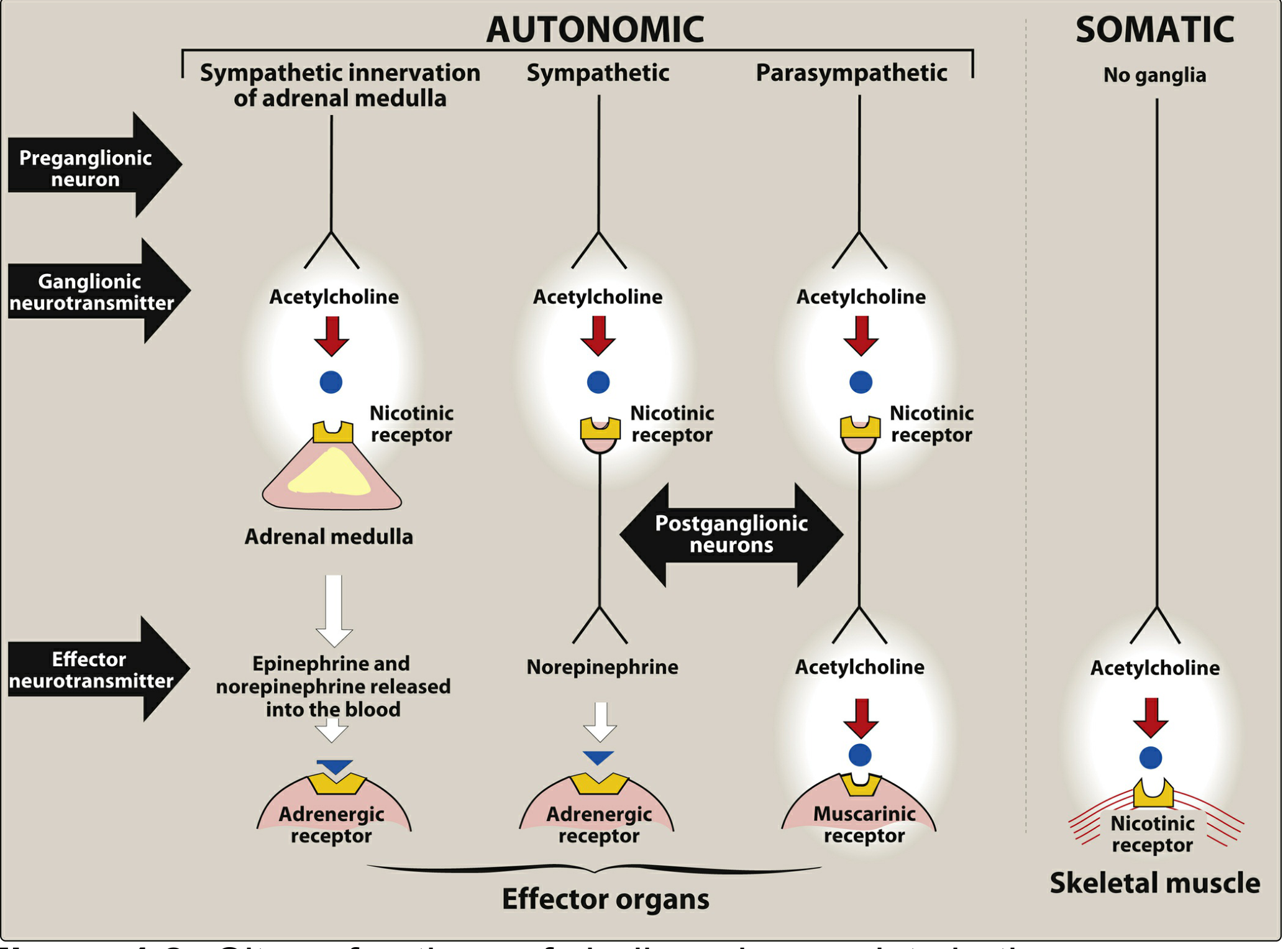
Key rules from this diagram:
- ALL preganglionic fibres (sympathetic and parasympathetic) release ACh onto Nicotinic receptors (Nn) at the ganglion
- Parasympathetic postganglionic fibres release ACh onto Muscarinic receptors at effectors
- Sympathetic postganglionic fibres release NE onto Adrenergic receptors at effectors
- The somatic system releases ACh onto Nicotinic (Nm) receptors at skeletal muscle
5. Cholinergic Receptors - Detailed
These receptors respond to acetylcholine. Named after chemicals that mimic ACh:
A. Muscarinic Receptors (M1-M5)
- Type: G protein-coupled receptors (GPCRs) - metabotropic
- Named after: Muscarine (from poisonous mushrooms)
- Location: Effector organs of parasympathetic system; also heart, smooth muscle, glands, CNS
| Subtype | Location | G-protein | Effect |
|---|---|---|---|
| M1 | CNS, gastric parietal cells, autonomic ganglia | Gq → PLC → IP3/DAG | Increased gastric acid; CNS excitation |
| M2 | Heart (SA node, AV node), smooth muscle | Gi → ↓cAMP, ↑K+ conductance | Decreased heart rate and force; slows conduction |
| M3 | Smooth muscle (bladder, gut, bronchi), glands, eye | Gq → PLC → IP3/DAG | Contraction of smooth muscle; glandular secretion |
| M4 | CNS | Gi | CNS modulation |
| M5 | CNS | Gq | CNS |
Clinically most important: M1, M2, M3
Signal transduction:
- M1/M3: Gq → activates Phospholipase C → produces IP3 and DAG → IP3 raises intracellular Ca²+ → smooth muscle contraction, gland secretion; DAG activates protein kinase C
- M2: Gi → inhibits adenylyl cyclase → ↓cAMP + ↑K+ conductance → slows heart
B. Nicotinic Receptors (Nn and Nm)
- Type: Ligand-gated ion channels (ionotropic) - fast response
- Named after: Nicotine (from tobacco)
- Mechanism: Opening of cation channel → Na+/Ca²+ influx → depolarisation
| Subtype | Location | Effect |
|---|---|---|
| Nn (neuronal) | Autonomic ganglia (both divisions), adrenal medulla, CNS | Ganglionic transmission; epinephrine release from adrenal medulla |
| Nm (muscle) | Neuromuscular junction (skeletal muscle) | Skeletal muscle contraction |
6. Adrenergic Receptors - Overview
These receptors respond to catecholamines (norepinephrine, epinephrine). Full detail comes in Topic 4, but here is the orientation:
| Receptor | Type | Coupling | Primary locations |
|---|---|---|---|
| α1 | GPCR | Gq → ↑IP3/DAG | Vascular smooth muscle, iris, bladder neck |
| α2 | GPCR | Gi → ↓cAMP | Presynaptic nerve terminals, pancreatic β-cells, platelets |
| β1 | GPCR | Gs → ↑cAMP | Heart (SA, AV node, ventricles), kidney (JGA) |
| β2 | GPCR | Gs → ↑cAMP | Bronchial smooth muscle, uterus, vascular smooth muscle |
| β3 | GPCR | Gs → ↑cAMP | Adipose tissue (lipolysis) |
7. Outline of Effects: Sympathetic vs. Parasympathetic
| Organ | Sympathetic (Adrenergic) | Parasympathetic (Muscarinic) |
|---|---|---|
| Heart rate | ↑ (β1) | ↓ (M2) |
| Heart contractility | ↑ (β1) | ↓ slight |
| Blood vessels | Constriction (α1) | Dilation (some - via NO) |
| Bronchi | Dilation (β2) | Constriction (M3) |
| GI motility | ↓ (α2, β2) | ↑ (M3) |
| GI sphincters | Contract (α1) | Relax (M3) |
| Urinary bladder (detrusor) | Relax (β2) | Contract (M3) |
| Urinary sphincter | Contract (α1) | Relax (M3) |
| Eye (pupil) | Dilate - mydriasis (α1) | Constrict - miosis (M3) |
| Eye (ciliary muscle) | Relax for far vision (β2) | Contract for near vision - accommodation (M3) |
| Salivary glands | Thick, scant saliva (α1) | Profuse, watery saliva (M3) |
| Sweat glands | Secretion (muscarinic - exception!) | - |
| Adrenal medulla | Epinephrine release (Nn) | - |
| Liver | Glycogenolysis (α1, β2) | - |
| Pancreas (insulin) | ↓ secretion (α2) | ↑ secretion |
Memory trick for Sympathetic: "Fight or Flight" - pupils dilate (see the enemy), heart pounds, bronchi open (breathe harder), blood goes to muscles (vasoconstriction elsewhere), digestion stops.
Memory trick for Parasympathetic: "Rest and Digest" - SLUD: Salivation, Lacrimation, Urination, Defecation.
8. Summary of Pharmacological Targets in the ANS
Drugs affecting the ANS can act at several points:
- Synthesis of neurotransmitter (e.g., reserpine blocks NE storage)
- Storage in vesicles
- Release from nerve terminals (e.g., guanethidine blocks NE release)
- Receptor activation (agonists - mimic NT)
- Receptor blockade (antagonists - block NT)
- Degradation of NT (e.g., anticholinesterases - prevent ACh breakdown)
- Reuptake inhibition (e.g., cocaine blocks NE reuptake)
Quick Recall Points (for exams)
- All preganglionic fibres → ACh → Nicotinic receptor
- Parasympathetic postganglionic → ACh → Muscarinic receptor
- Sympathetic postganglionic → NE → Adrenergic receptor (exception: sweat glands use ACh → Muscarinic)
- Adrenal medulla = modified sympathetic ganglion, releases EPI + NE into blood
- Muscarinic receptors = GPCRs (slow)
- Nicotinic receptors = ion channels (fast)
- M2 on heart: Gi → ↓HR; M1/M3: Gq → smooth muscle/gland effects
Sources: Lippincott Illustrated Reviews: Pharmacology, Chapter 4; Ganong's Review of Medical Physiology, Chapter 13
That's Topic 1 fully covered! Your syllabus has 4 more topics:
Introduction to Autonomic Pharmacology✅- Cholinergic Receptor Agonists / Cholinomimetics (acetylcholine, bethanechol, pilocarpine, neostigmine + glaucoma/MG/OP poisoning management)
- Cholinergic Receptor Antagonists (atropine and substitutes)
- Adrenergic Receptor Agonists / Sympathomimetics (epinephrine, NE, dopamine, alpha/beta agonists)
- Adrenergic Receptor Antagonists (alpha blockers, beta blockers)
Just say "next" or "Topic 2" whenever you're ready to continue!
Start Topic 2: Cholinergic Agonists & Cholinomimetics
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
All content gathered. Now delivering the full Topic 2 explanation.
TOPIC 2: Cholinergic Receptor Agonists / Cholinomimetics
1. Definition & Classification
Cholinergic agonists (cholinomimetics) are drugs that mimic the effects of acetylcholine (ACh) by acting on cholinergic receptors (muscarinic and/or nicotinic).
They are classified into two major groups:
CHOLINERGIC AGONISTS
├── DIRECT-ACTING (bind receptors directly)
│ ├── Choline Esters → Acetylcholine, Bethanechol, Carbachol, Methacholine
│ └── Alkaloids → Pilocarpine, Muscarine, Nicotine
└── INDIRECT-ACTING (inhibit AChE → ↑ ACh at synapse)
├── Reversible AChE inhibitors → Physostigmine, Neostigmine, Pyridostigmine
└── Irreversible AChE inhibitors → Organophosphates (parathion, echothiophate, nerve agents)
2. Direct-Acting Agents - Choline Esters
Key Properties Table
| Drug | Hydrolysis by AChE | Muscarinic | Nicotinic | Route | Duration |
|---|---|---|---|---|---|
| Acetylcholine | ++++ (very fast) | +++ | +++ | IV only | Very short (5-20 sec) |
| Methacholine | + (slow) | ++++ | None | Inhaled/SC | Longer |
| Carbachol | Negligible | ++ | +++ | Topical/Oral | Long |
| Bethanechol | Negligible | ++ | None | Oral/SC | ~1 hour |
Why no oral ACh? It is rapidly hydrolysed in the gut and blood - too short-acting to be clinically useful.
β-methyl group (in methacholine, bethanechol) → reduces nicotinic activity, preserves muscarinic. This is why bethanechol has ZERO nicotinic activity.
A. Acetylcholine (ACh)
- Quaternary ammonium compound - cannot cross cell membranes or BBB
- Acts on BOTH muscarinic and nicotinic receptors
- Not clinically used systemically (too rapid degradation, too diffuse effects)
- Clinical use: Topical ophthalmic solution → produces miosis during cataract/lens implant surgery
Systemic actions (if given IV):
- Heart: Bradycardia, ↓ cardiac output (M2 on SA node)
- Blood vessels: Vasodilation + ↓ BP via M3 on endothelium → NO production → smooth muscle relaxation
- GI: ↑ motility, ↑ salivation, ↑ gastric acid
- Lungs: Bronchoconstriction, ↑ secretions
- Bladder: Contracts detrusor → urination
- Eye: Miosis + accommodation (ciliary muscle contraction)
B. Bethanechol ⭐ (Most Clinically Important Ester)
- Pure muscarinic agonist - NO nicotinic activity
- Not hydrolysed by AChE - carbamic acid ester
- Strong action on bladder and GI smooth muscle
- Oral or SC administration
Actions:
- ↑ intestinal motility and tone
- Stimulates detrusor muscle of bladder → relaxes trigone and sphincter → urination
Therapeutic Uses:
- Postoperative/postpartum urinary retention (non-obstructive, atonic bladder) - main use
- Neurogenic bladder atony
- Toxic megacolon (rarely)
Adverse Effects:
- Sweating, salivation, flushing
- ↓ BP with reflex tachycardia
- Nausea, abdominal cramps, diarrhea
- Bronchospasm
Contraindications:
- Asthma (bronchoconstriction)
- Peptic ulcer (↑ gastric acid)
- Urinary or GI obstruction (never give if mechanical obstruction exists!)
- Hyperthyroidism, coronary artery disease
Antidote for overdose: Atropine
C. Pilocarpine ⭐ (Most Clinically Important Alkaloid)
- Tertiary amine alkaloid - lipid soluble, well absorbed, can cross BBB
- Mainly muscarinic activity
- Source: leaves of Pilocarpus jaborandi (plant)
Actions:
- Powerful stimulant of exocrine glands (sweating, salivation, lacrimation)
- Eye: Miosis + ciliary muscle contraction (spasm of accommodation) → ↓ intraocular pressure (IOP)
Therapeutic Uses:
- Glaucoma - most important use (open-angle AND narrow-angle)
- Xerostomia (dry mouth) after radiation therapy for head/neck cancer
- Sjögren's syndrome (dry mouth/eyes)
Adverse Effects: Sweating, salivation, GI cramps, blurred vision (miosis)
D. Carbachol
- Both muscarinic AND nicotinic activity
- Resistant to AChE hydrolysis
- Uses: Topical ophthalmic - miosis during surgery; alternative to pilocarpine in glaucoma (when tolerance develops)
E. Methacholine
- Mainly muscarinic, resistant to AChE
- Methacholine challenge test - inhaled provocatively to diagnose bronchial hyperresponsiveness in asthma
F. Muscarine
- Naturally occurring alkaloid (from Amanita muscarina mushrooms)
- Purely muscarinic activity
- Not used clinically - toxicological importance (mushroom poisoning)
- Causes: SLUD syndrome (Salivation, Lacrimation, Urination, Defecation) + bradycardia, bronchospasm
3. Indirect-Acting Agents - Anticholinesterases
These drugs do NOT directly activate receptors. Instead, they inhibit acetylcholinesterase (AChE), the enzyme that breaks down ACh, causing ACh to accumulate at all cholinergic synapses.
How AChE Normally Works:
ACh + AChE → Choline + Acetic acid (ACh is destroyed in microseconds)
By inhibiting AChE, ACh accumulates → prolonged muscarinic + nicotinic effects
Reversible AChE Inhibitors
A. Physostigmine (Eserine) ⭐
- Natural alkaloid from Calabar bean (Physostigma venenosum)
- Tertiary amine → lipid soluble → crosses BBB → acts in CNS
- Carbamic acid ester - reversibly binds AChE for 30 min - 2 hours
Actions:
- Stimulates muscarinic receptors (GI motility, ↑ secretions, bradycardia, miosis)
- Stimulates skeletal muscle (via ↑ ACh at NMJ)
- CNS effects (since it crosses BBB) - can reverse CNS anticholinergic effects
Therapeutic Uses:
- Glaucoma (historically, now replaced by better agents)
- Antidote for atropine poisoning / anticholinergic overdose - key use! (including tricyclic antidepressant OD)
- Reversal of CNS effects of antimuscarinics
Adverse Effects:
- Bradycardia, ↓ BP
- GI cramps, diarrhea
- Convulsions at high doses
- Skeletal muscle paralysis (rarely)
B. Neostigmine ⭐
- Synthetic compound, carbamic acid ester
- Quaternary ammonium → does NOT cross BBB → no CNS effects
- Greater effect on skeletal muscle (NMJ) than physostigmine
- Duration: 30 min - 2 hours
Actions:
- Strong stimulation of GI tract and bladder
- Strong facilitation of NMJ (↑ skeletal muscle contraction)
- No CNS penetration
Therapeutic Uses:
- Myasthenia gravis (symptomatic treatment) ⭐
- Reversal of non-depolarising neuromuscular blockade (post-surgery, e.g., reversal of tubocurarine, rocuronium)
- Postoperative urinary retention and abdominal distension (Ogilvie syndrome)
Adverse Effects:
- Salivation, nausea, diarrhea, abdominal cramps
- Bronchospasm
- Bradycardia
- No CNS effects (cannot cross BBB - important distinction from physostigmine)
Contraindications:
- Intestinal or urinary bladder obstruction (mechanical)
- Asthma
C. Pyridostigmine
- Similar to neostigmine (quaternary amine, no CNS penetration)
- Longer duration than neostigmine (3-6 hours)
- Main use: Chronic management of myasthenia gravis (preferred over neostigmine for long-term)
- Also used as prophylaxis against nerve agent (soman) poisoning in military
D. Edrophonium
- Very short-acting (5-15 min), reversible AChE inhibitor
- Tensilon test - IV injection used to diagnose myasthenia gravis (brief improvement in muscle strength confirms diagnosis)
- Now largely replaced by antibody tests, but still classic exam question
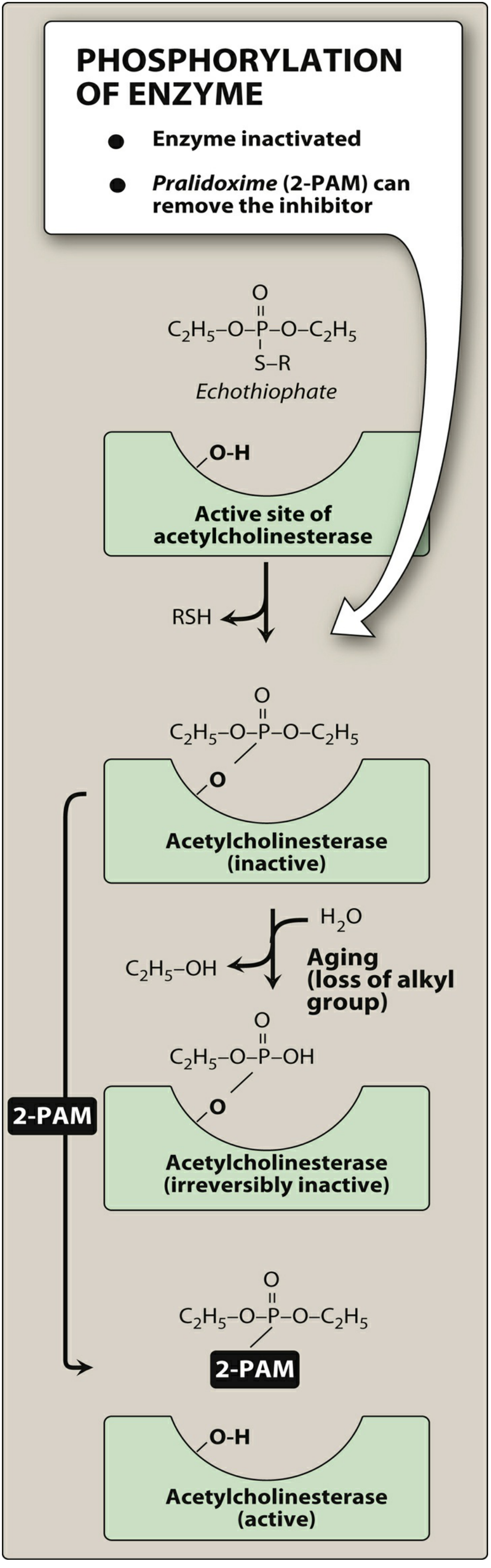
Irreversible AChE Inhibitors - Organophosphates
These form a covalent bond with AChE. The enzyme cannot be reactivated unless an antidote is given quickly.
Mechanism: Organophosphate binds to serine -OH at active site of AChE → phosphorylated enzyme → AChE permanently inactivated
"Aging" phenomenon: Over time, one alkyl group is lost from the phosphorylated enzyme - making it IMPOSSIBLE to reactivate, even with antidotes.
Examples:
- Agricultural insecticides: Parathion, Malathion, Diazinon
- Nerve agents (chemical warfare): Sarin, Soman, Tabun, VX
- Ophthalmic (historical): Echothiophate (open-angle glaucoma - now withdrawn)
4. Organophosphate (OP) Poisoning - Principles of Management ⭐⭐
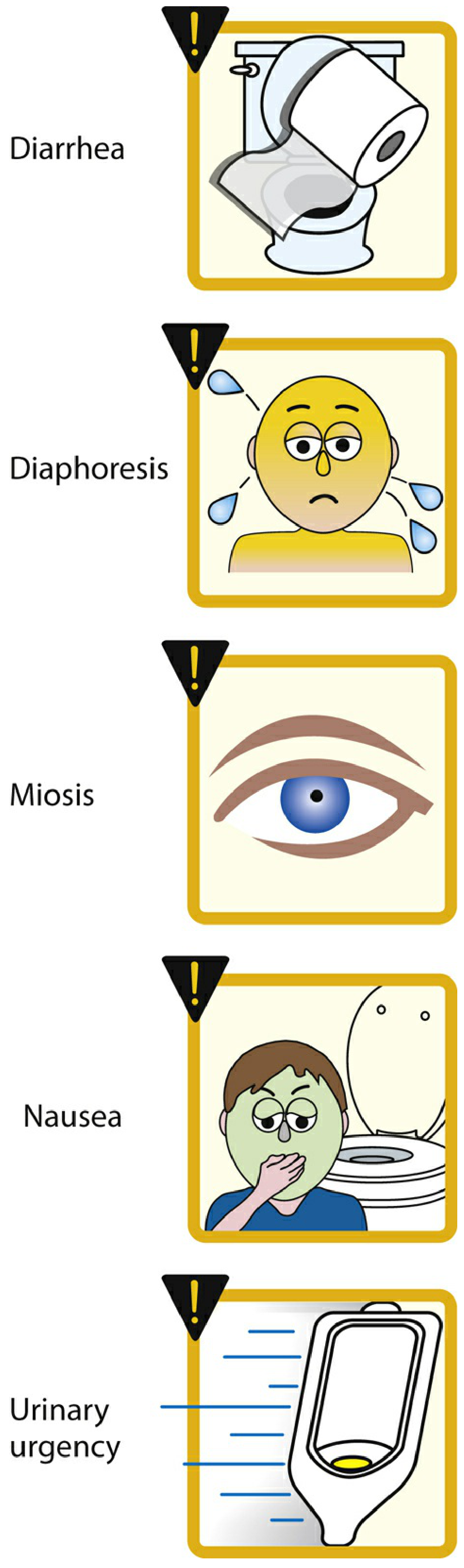
Signs and Symptoms - "Cholinergic Crisis"
Excess ACh at ALL cholinergic synapses produces a predictable pattern:
Muscarinic effects (mnemonic: DUMBELS or SLUDGE):
| Mnemonic | Feature |
|---|---|
| D - Defecation, Diarrhea | GI overactivity |
| U - Urination | Detrusor contraction |
| M - Miosis | Pupil constriction |
| B - Bradycardia, Bronchospasm, Bronchorrhea | Cardiac + respiratory |
| E - Emesis | Nausea/vomiting |
| L - Lacrimation | ↑ tear secretion |
| S - Salivation, Sweating | ↑ gland secretion |
Nicotinic effects (at NMJ and ganglia):
- Muscle fasciculations → weakness → paralysis (including respiratory muscles - LETHAL)
- Tachycardia, hypertension (at ganglia)
- Pallor, diaphoresis
CNS effects:
- Anxiety, restlessness, seizures, coma
- Respiratory depression (central + peripheral)
The lethal triad: Bronchospasm + Bronchorrhea + Respiratory muscle paralysis
Management of OP Poisoning
Step 1 - Decontamination: Remove clothing, wash skin with soap and water (protect the rescuer!)
Step 2 - Stabilise: Airway, Breathing, Circulation (ABC). Suctioning of secretions. Intubation if needed.
Step 3 - Atropine ⭐⭐ (FIRST and most important drug)
- Blocks muscarinic effects only
- Dose: 2-4 mg IV every 5-10 minutes until drying of secretions (atropinisation)
- Endpoint: dry mouth, clear lungs - NOT pupil dilation
- Very large doses may be needed (10s to 100s of mg in severe cases)
- Does NOT reverse nicotinic effects (muscle weakness/paralysis)
Step 4 - Pralidoxime (2-PAM) ⭐⭐ (Oxime - AChE reactivator)
- Must be given early (before aging occurs!)
- Reactivates phosphorylated AChE by binding the organophosphate and removing it from the enzyme
- Restores both muscarinic AND nicotinic function
- Dose: 1-2 g IV over 15-30 minutes
- Ineffective after aging - hence urgency of early administration
- Cannot cross BBB well - poor for CNS effects
Step 5 - Benzodiazepines (diazepam) - for seizures
Step 6 - Avoid: Morphine, aminophylline, phenothiazines (contraindicated)
5. Myasthenia Gravis - Principles of Management ⭐⭐
What is Myasthenia Gravis?
An autoimmune disease where antibodies against nicotinic (Nm) receptors at the neuromuscular junction (NMJ) are produced. This destroys and blocks Nm receptors → impaired neuromuscular transmission → skeletal muscle weakness.
- Characteristic: fatigable weakness - worse with activity, better with rest
- Commonly affects ocular muscles (ptosis, diplopia), facial, bulbar, limb, and respiratory muscles
- Thymoma association (20% of patients have thymoma; thymus is removed in treatment)
Pharmacological Management
1. Anticholinesterases - Symptomatic treatment:
- Pyridostigmine (Mestinon) - drug of choice for chronic management
- Inhibits AChE → ↑ ACh at NMJ → stimulates remaining functional Nm receptors
- Dose: 30-60 mg orally every 4-6 hours
- Adverse effects: muscarinic (SLUDGE symptoms), controlled with atropine/glycopyrrolate
- Neostigmine - used for acute/short-term management, quicker onset
2. Immunosuppression - Disease-modifying:
- Prednisolone (corticosteroids) - first-line immunosuppressant
- Azathioprine - steroid-sparing agent
- Mycophenolate, cyclosporine - alternatives
3. Plasma exchange (Plasmapheresis) and IVIG:
- For myasthenic crisis (acute severe deterioration)
- Rapidly removes anti-AChR antibodies from circulation
4. Thymectomy:
- Indicated if thymoma present or in generalised MG in patients < 60 years
- Can induce long-term remission
5. Eculizumab, Efgartigimod - newer biologics for refractory MG
Warning - Cholinergic Crisis vs Myasthenic Crisis:
| Myasthenic Crisis | Cholinergic Crisis | |
|---|---|---|
| Cause | Too LITTLE ACh (under-medication) | Too MUCH ACh (over-medication with anticholinesterase) |
| Pupil | Normal/dilated | Miosis |
| Secretions | Normal | Excessive (SLUDGE) |
| Tensilon test | Improves muscle strength | Worsens muscle strength |
| Treatment | More anticholinesterase | Atropine + stop anticholinesterase |
6. Glaucoma - Principles of Management ⭐⭐
What is Glaucoma?
Pathological increase in intraocular pressure (IOP) leading to optic nerve damage and eventual blindness.
- Normal IOP: 10-21 mmHg
- Aqueous humor is produced by the ciliary body and drains via the trabecular meshwork into the Canal of Schlemm
Types:
- Open-angle glaucoma (most common, 90%) - trabecular meshwork gradually becomes less efficient; drainage is not blocked
- Narrow/Closed-angle glaucoma (acute angle closure) - iris physically blocks the drainage angle; medical emergency
How Cholinergic Drugs Lower IOP:
Pilocarpine and Carbachol:
- Contract the ciliary muscle (M3 activation) → pulls on trabecular meshwork → opens drainage channels → aqueous humor outflow increases → ↓ IOP
- Contract the sphincter pupillae → miosis → iris is pulled away from the drainage angle → especially useful in narrow-angle glaucoma
Complete Management of Glaucoma (Drug Classes):
| Drug Class | Examples | Mechanism |
|---|---|---|
| Cholinergic agonists | Pilocarpine, Carbachol | ↑ aqueous outflow via trabecular meshwork (miosis + ciliary contraction) |
| Prostaglandin analogues (1st line) | Latanoprost, Bimatoprost | ↑ uveoscleral outflow |
| Beta blockers (topical) | Timolol, Betaxolol | ↓ aqueous humor production (↓ cAMP in ciliary epithelium) |
| Alpha-2 agonists | Brimonidine | ↓ production + ↑ outflow |
| Carbonic anhydrase inhibitors | Dorzolamide (topical), Acetazolamide (systemic) | ↓ aqueous humor production (inhibit HCO3- formation) |
| Hyperosmotic agents | Mannitol, Glycerol | ↓ vitreous volume - acute emergencies |
Acute angle-closure glaucoma: Emergency - use IV acetazolamide + IV mannitol to rapidly lower IOP, then pilocarpine 2% drops + laser iridotomy (definitive)
7. Adverse Effects of Cholinergic Agonists - Visual Summary
Mnemonic for adverse effects: DUMBELS
Diarrhea, Urination, Miosis, Bradycardia/Bronchospasm, Emesis, Lacrimation, Salivation/Sweating
8. Physostigmine vs. Neostigmine - Key Comparison (High Yield)
| Feature | Physostigmine | Neostigmine |
|---|---|---|
| Source | Natural (Calabar bean) | Synthetic |
| Chemical type | Tertiary amine | Quaternary amine |
| Crosses BBB | YES | NO |
| CNS effects | Yes | None |
| NMJ stimulation | Moderate | Strong |
| Main uses | Atropine OD, anticholinergic OD | MG, NMJ reversal, urinary retention |
| GI absorption | Good | Poor |
Quick Recall Points
- Bethanechol = muscarinic only (no nicotinic), used for urinary retention
- Pilocarpine = best for glaucoma and dry mouth (Sjögren's, radiation)
- Methacholine = bronchial challenge test for asthma diagnosis
- Physostigmine = crosses BBB → antidote for atropine/anticholinergic OD
- Neostigmine = does NOT cross BBB → myasthenia gravis + NMJ reversal
- Pyridostigmine = chronic MG management (longer acting)
- Pralidoxime (2-PAM) = reactivates AChE in OP poisoning - give EARLY before aging
- Atropine = first drug in OP poisoning - treats muscarinic symptoms
Sources: Lippincott Illustrated Reviews: Pharmacology, Chapter 4; Katzung's Basic & Clinical Pharmacology, 16th Ed, Chapter 7
Topic 2 complete! Your syllabus topics remaining:
- Cholinergic Receptor Antagonists (Atropine prototype + substitutes)
- Adrenergic Receptor Agonists (Epinephrine, NE, Dopamine, α & β agonists)
- Adrenergic Receptor Antagonists (α-blockers, β-blockers, Propranolol)
Say "Topic 3" whenever you're ready!
This is a shared conversation. Sign in to Orris to start your own chat.