Reading File
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile the full response.
Q1: Argyll-Robertson Pupil - Complete Answer
1. What is Argyll-Robertson Pupil? (2 marks)
The Argyll-Robertson (AR) pupil is a bilateral, small (< 2 mm), irregular pupil that:
- Fails to constrict to light (direct and consensual light reflex absent)
- Constricts normally to accommodation/convergence (near response preserved)
- This is called "light-near dissociation"
Additional features:
- Bilateral and asymmetric
- Irregular shape (due to iris atrophy)
- Poor dilation in darkness
- Near-response is brisk (distinguishes it from chronic tonic pupils, which have a slow near-response)
It is classically associated with neurosyphilis (tabes dorsalis, general paresis of the insane). Other causes include diabetes mellitus, chronic alcoholism, encephalitis, multiple sclerosis, and Lyme disease.
- Localization in Clinical Neurology, 8e; Guyton and Hall Textbook of Medical Physiology
2. Sites of Lesion (1 mark)
The block in AR pupil occurs at the level of the pretectal region of the midbrain (dorsal midbrain, at or near the superior colliculus level).
Specifically, the lesion affects the internuncial (second-order) neurons that connect the pretectal nuclei to the Edinger-Westphal nuclei. These fibers travel through the posterior commissure and are located dorsal to the near-reflex fibers (which travel more ventrally). This explains why the near reflex is spared while the light reflex is abolished.
Key mechanistic point from Guyton & Hall: the final nerve fibers through the pretectal area to the Edinger-Westphal nucleus are inhibitory. Loss of these fibers causes:
- Chronic activation of the Edinger-Westphal nucleus → persistent miosis
- Loss of response to light
- Preserved near response (via a more ventral, spared pathway)
- Guyton and Hall Textbook of Medical Physiology; Kanski's Clinical Ophthalmology 10th ed.
3. Transverse Section of Midbrain at Level of Superior Colliculus (6 marks)
Here is a textbook cross-section of the rostral midbrain at the level of the superior colliculus:
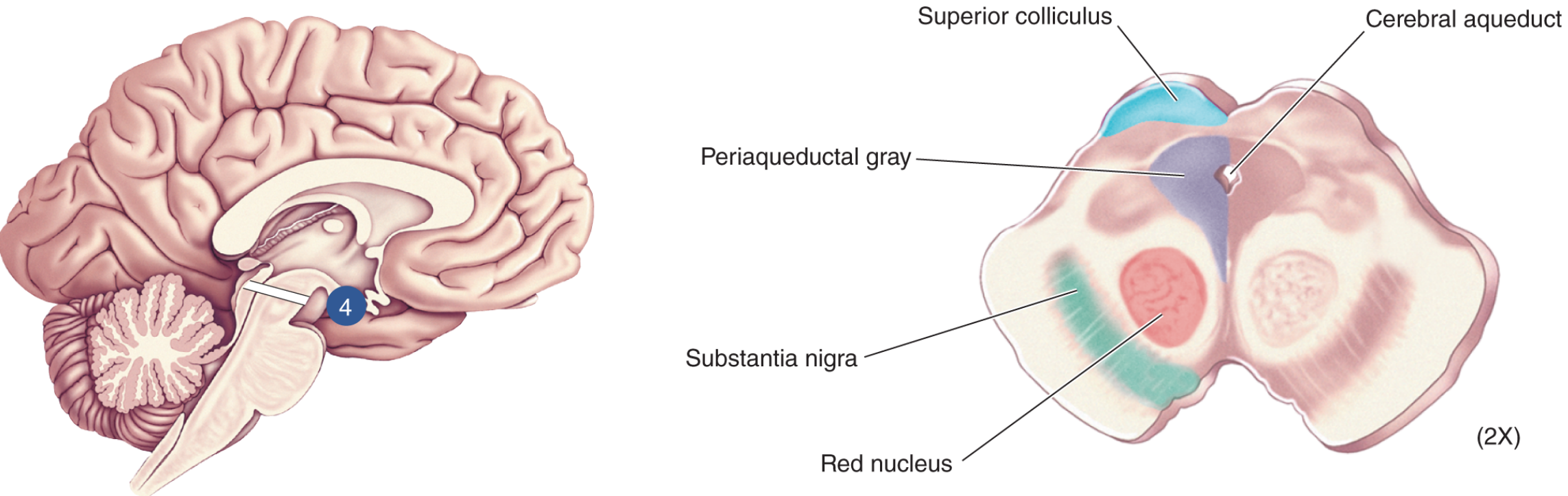
- Neuroscience: Exploring the Brain, Fifth Edition
Structures (from dorsal to ventral):
| Region | Structure | Function |
|---|---|---|
| Tectum (roof) | Superior colliculus (bilateral) | Reflex turning of eyes and head toward visual/auditory stimuli |
| Tegmentum | Cerebral aqueduct (of Sylvius) | CSF passage connecting 3rd and 4th ventricles |
| Periaqueductal gray (PAG) | Pain modulation; autonomic control; contains nuclei | |
| Oculomotor nucleus (CN III) | Movement of eyeball (extra-ocular muscles); contains Edinger-Westphal nucleus (parasympathetic) | |
| Pretectal nucleus | Light reflex relay | |
| Mesencephalic nucleus of trigeminal (CN V) | Proprioception from jaw muscles | |
| Red nucleus | Motor coordination, movement control (rubrospinal tract) | |
| Basis pedunculi | Substantia nigra | Motor control (dopaminergic, basal ganglia circuit) |
| Cerebral peduncles (crus cerebri) | Descending corticospinal, corticobulbar, corticopontine tracts |
Your notes summarize this well:
- SC = Superior colliculus - reflex turning of eyes and head
- Pretectal Nu = Light reflex relay
- Oculomotor Nu = Moves eyeball
- Mesencephalic Nu (Trigeminal) = Proprioception of jaw
- Red Nu = Motor coordination (movement control)
- Central grey = Periaqueductal grey, contains nuclei
4. Pathway for Light Reflex (3 marks)
Here is the complete pathway diagram from Adams & Victor's Principles of Neurology:
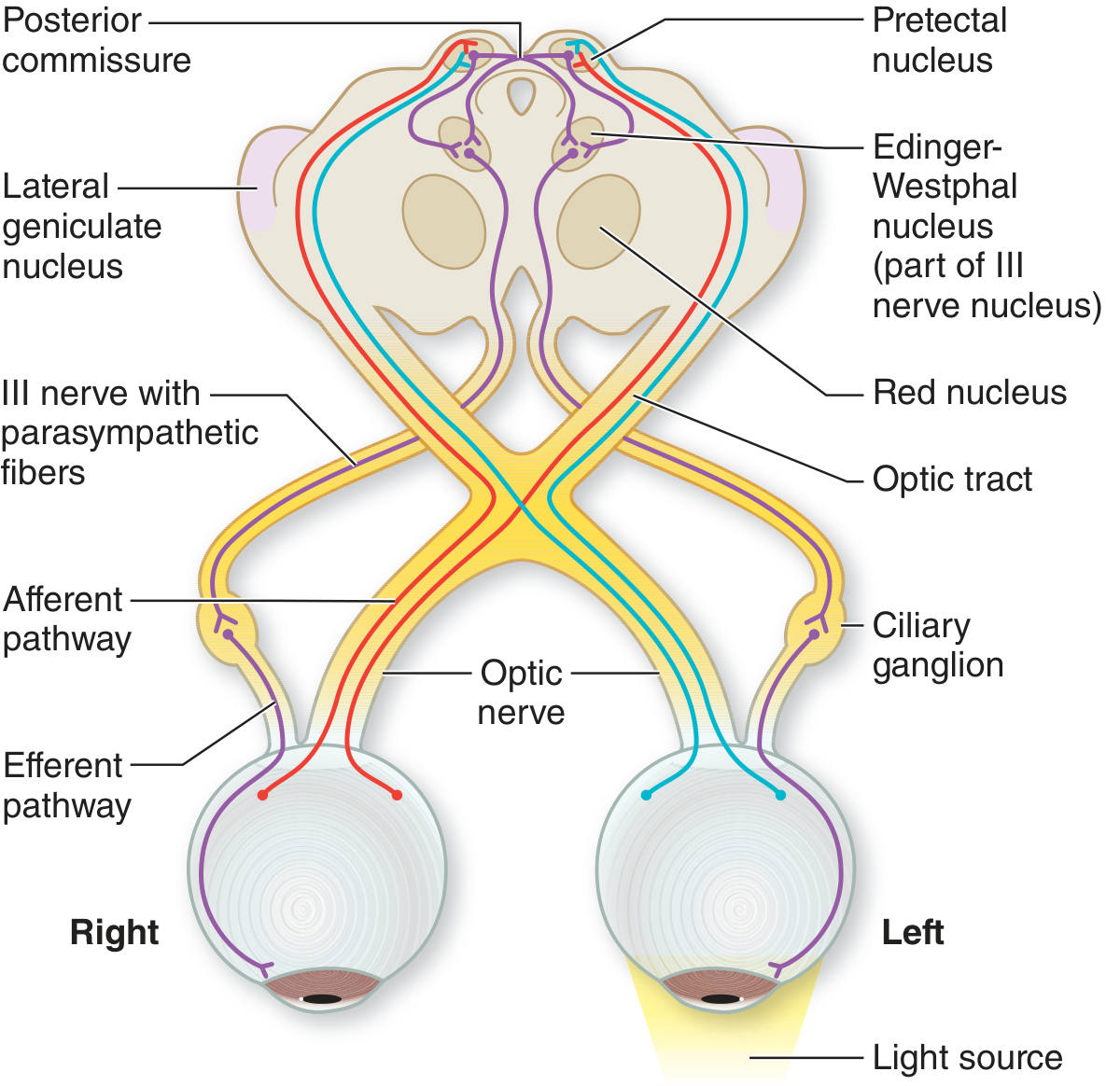
- Adams and Victor's Principles of Neurology, 12th Edition
The pathway involves 4 neurons (mediated by both parasympathetic and sensory fibers):
1st Neuron - Afferent (Sensory) Arc:
- Retinal photoreceptors (rods/cones + intrinsically photosensitive retinal ganglion cells containing melanopsin) → ganglion cell axons → optic nerve → optic chiasm (partial decussation: nasal fibers cross, temporal fibers stay ipsilateral) → optic tract → fibers leave the optic tract just before the lateral geniculate nucleus (without synapsing in it) → enter the rostral midbrain → synapse in the pretectal nucleus (olivary pretectal nucleus)
2nd Neuron - Internuncial (Commissural):
- From each pretectal nucleus, fibers pass bilaterally to both Edinger-Westphal nuclei (some cross via the posterior commissure)
- This bilateral connection explains why a light in one eye causes constriction in BOTH pupils (direct + consensual reflexes)
3rd Neuron - Preganglionic Efferent (Parasympathetic):
- From the Edinger-Westphal nucleus → travels with the oculomotor nerve (CN III) → enters its inferior division → synapses in the ciliary ganglion (in the orbit)
4th Neuron - Postganglionic Efferent:
- From the ciliary ganglion → short ciliary nerves → innervate the sphincter pupillae → pupillary constriction (miosis)
- Kanski's Clinical Ophthalmology 10th ed.; Adams and Victor's Principles of Neurology 12th ed.
Summary Table: Why Light-Near Dissociation Occurs in AR Pupil
| Test | Result in AR Pupil | Explanation |
|---|---|---|
| Light reflex | Absent | Internuncial neurons (dorsal pretectal → EW pathway) are destroyed |
| Near reflex | Preserved (brisk) | Near-reflex fibers travel more ventrally and are spared |
| Pupil size | Small (< 2 mm) | Loss of tonic inhibition → EW chronically active → persistent miosis |
| Shape | Irregular | Iris atrophy from syphilitic iridocyclitis |
This is a shared conversation. Sign in to Orris to start your own chat.